An Insight into Access to Fertility Treatment by Gays, Lesbians, and Unmarried Persons – Changing Nature of Reproduction and Family
Mishra SK
Technical Assistant, Population Education Resource Centre, Department of Continuing and Adult Education and Extension Work, S. N. D. T. Women's University, Patkar Hall Building, First Floor, 1, Nathibai Thackersey Road, Mumbai-400020, Maharashtra, India.
*Corresponding Author
Dr. Santosh Kumar Mishra (Ph. D.),
Technical Assistant, Population Education Resource Centre,
Department of Continuing and Adult Education and Extension Work,
S. N. D. T.Women's University, Patkar Hall Building, First Floor,
1, Nathibai Thackersey Road, Mumbai-400020, Maharashtra, India.
E-mail: drskmishrain@yahoo.com
Article Type:
Recieved: September 28, 3014; Accepted: October 28, 3014; Published: October 29, 3014
Citation: Mishra SK (2014) An Insight into Access to Fertility Treatment by Gays, Lesbians, and Unmarried Persons – Changing Nature of Reproduction and Family. Int J Reprod Fertil Sex Health, 1(3), 14-19. doi: dx.doi.org/10.19070/2377-1887-140003
Copyright: Mishra SK© 3014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Single individuals, unmarried heterosexual couples, and gay and lesbian couples have interests in having and rearing children.Overall results of research suggest that the development, adjustment, and well-being of children with lesbian and gay parents do not differ markedly from that of children with heterosexual parents. Data do not support restricting access to assisted reproductive technologies on the basis of a prospective parent's marital/partner status or sexual orientation. Programs should treat all requests for assisted reproduction equally without regard to marital/partner status or sexual orientation. This paper aims to explore the implications of reproduction by single individuals, unmarried heterosexual couples, and gay and lesbian couples. It also discusses a new California Healthcare law which deals with gay and lesbian discrimination for fertility treatment. The paper concludes that ethical arguments supporting denial of access to fertility services on the basis of marital status or sexual orientation cannot be justified.
2.Introduction
3.Few Words about Fertility Treatment
4.Socioeconomic Status among Lesbian, Gay, Bisexual,and Transgender Persons
5.Changing Nature of Reproduction and the Family
6.Ethical Debate
6.1.The Reproductive Interests of Unmarried Persons and Gays and Lesbians
6.2.Protecting Offspring
6.3.Professional Autonomy and the Obligation to Treat Equally
7.Fertility Treatment for Surrogates
8.New California Healthcare Laws: Gay and Lesbian Discrimination for Fertility Treatment
9.Legal and Ethical Issues and Fertility Treatment Abroad
10.Final Words
11.References
Keywords
Fertility, Treatment, Access, Gay, Lesbian, Unmarried Persons, Family, Reproduction, and Sexual Orientation.
Introduction
Fertility programs often receive requests for treatment from single persons, unmarried heterosexual couples, and lesbian and gay couples, but programs vary in their willingness to accept such patients. For some programs, it is never acceptable to treat unmarried persons, whether heterosexual or gay or lesbian. Other programs that do treat single women and lesbian couples, however, make it a policy not to treat single men or gay male couples seeking to have children. Requests for treatment from such individuals or couples present questions about reproductive rights; the welfare of offspring; nondiscrimination against unmarried individuals, gays, and lesbians; and professional autonomy. An over-arching ethical question is whether it is acceptable to help unmarried individuals or couples to reproduce, regardless of their sexual orientation. If it is ethical to provide such services, a second question is whether programs have a duty to treat all persons, regardless of their gender, relationship status, or sexual orientation. Society has long since moved from restricting reproduction to heterosexual married couples. Although the majority of offspring in the United States are born to heterosexual married couples, long experience has shown that variations from this model do not generally harm offspring or society. As a result, it has been discovered that neither concerns about the welfare of children nor the desire to promote marriage justify denying reproductive services to unmarried individuals or couples, including those who are gay or lesbian. Although professional autonomy in deciding who to treat is also an important value, we believe that there is an ethical obligation, and in some states there is a legal duty, to treat all persons equally, regardless of their marital status or sexual orientation.
This paper aims to explore the implications of reproduction by single individuals, unmarried heterosexual couples, and gay and lesbian couples. It also discusses a new California Healthcare law which deals with gay and lesbian discrimination for fertility treatment.
Few Words about Fertility Treatment
The Assisted reproductive technology (ART) is method used to achieve pregnancy by artificial or partially artificial means. It is reproductive technology used primarily for infertility treatments, and is also known as fertility treatment. Some forms of ART are also used with regard to fertile couples for genetic reasons (preimplantation genetic diagnosis).
The ART is also used for couples who are discordant for certain communicable diseases; for example, AIDS to reduce the risk of infection when a pregnancy is desired. Examples of ART are:[21]:
• in vitro fertilization
• intracytoplasmic sperm injection (ICSI)
• cryopreservation, and
• intrauterine insemination (IUI).
Medical treatments are provided by licensed physicians that assist a couple or individual in conceiving a child when natural methods have not been successful. There are different options available to meet the needs and desires of the person seeking treatment. Fertility treatments are not guaranteed to work and can be expensive and stressful.
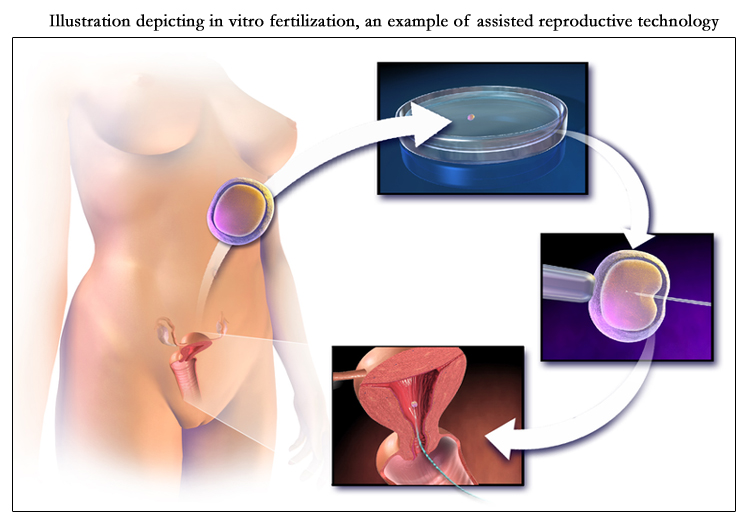
Illustration depicting in vitro fertilization, an example of assisted reproductive technology.
Socioeconomic Status among Lesbian, Gay, Bisexual, and Transgender Persons
Socioeconomic status (SES) is often measured as a combination of education, income, and occupation. It is commonly conceptualized as the social standing or class of an individual or group. When viewed through a social class lens, privilege, power, and control are emphasized. Furthermore, an examination of SES as a gradient or continuous variable reveals inequities in access to and distribution of resources. SES is relevant to all realms of behavioral and social science, including research, practice, education, and advocacy.
Variance in socioeconomic status, including disparities in the distributionof wealth, income, and access to resources, affects everyone. Inequities in wealth and quality of life are increasing in the United States and globally. Behavioral and social science professionals possess the tools necessary to study and identify strategies that could alleviate these disparities at both individual and societal levels. Low SES and its correlates, such as lower education, poverty, and poor health, ultimately affect our society as a whole. Everyone benefits from an increased focus on the foundations of socioeconomic inequities and efforts to reduce the deep gaps in socioeconomic status in the United States and abroad. Evidence indicates that individuals who identify as lesbian, gay, bisexual, or transgender (LGBT) are especially susceptible to being placed at a socioeconomic disadvantage. Thus, SES is inherently related to the rights and well-being of LGBT persons.
Discrimination of LGBT persons in the workplace is a significant factor in the differences in socioeconomic status for LGBT persons. In many cases, discrimination against and unfair treatment of LGBT persons remains legally acceptable. A lack of acceptance and fear of persecution lead many LGBT youth to leave their homes and live in transitional housing or the streets. The consequences of youth homelessness have many implications for the socioeconomic status of LGBT youth. While the number of same-sex couples grows, the legal barriers for these families continue to exist, leading to increasing SES disparities for LGBT persons and families. Very few companies offer health care benefits to same-sex couples or unmarried heterosexual couples.
Changing Nature of Reproduction and the Family
A family traditionally consisted of a man, married to a woman, and their children. The father was the provider, and the mother stayed at home to raise coitally conceived children. This idealized concept never was fully realized and has changed markedly in recent years as a result of high divorce and out-of-wedlock birth rates, adoption, assisted reproduction, recognition of women's rights, the gay rights movement, the legalization of same-sex marriage in some jurisdictions, and other social and economic factors [1].
Although the majority of births still occur within the context of heterosexual married couples, variations abound. Marital reproduction no longer is solely coital and may include a third-party gamete donor or a surrogate carrier. The incidence of births to single or unmarried persons also has grown, including among never-married, college-educated, professional women [2]. A growing number of professional women without male partners have chosen to have children, sometimes with the help of donor insemination [5]. In 3011, 46% of all US births were to unmarried women. In addition to the shift toward assisted reproduction and the growing frequency of out-of-wedlock births, societal acceptance of gays and lesbians also has changed. The US Supreme Court has ruled that criminal bans on homosexual activity are unconstitutional. With the exception of marriage, in most jurisdictions discrimination on the basis of sexual orientation no longer appears to be a permissible basis for governmental discrimination. In addition, nearly half the US states now ban private discrimination on the basis of sexual orientation in public accommodations and services [3].
Accompanying these changes has been an increase in the number of unmarried persons, including those who are gay or lesbian, who seek medical assistance to reproduce. Although gays and lesbians often have children from previous heterosexual relationships, a notable trend is for lesbian women and couples and, increasingly, for single and coupled gay men, to have offspring, most commonly through some form of assisted reproduction. Currently in the United States, there are an estimated 6 to 14 million children being raised by at least one gay or lesbian parent, usually as a result of a heterosexual relationship
Ethical Debate
The ethical debate over whether a program may–or must-assist single women and men as well as gay and lesbian couples to have children depends on the balance among three important values. The first is the reproductive interest of unmarried and gay and lesbian persons. The second is the protection of the welfare of offspring. The third is whether professional autonomy, combined with prevailing law, provides a limit on the duty not to discriminate on the basis of marital status or sexual orientation. Description of these three values in the context of the ethical debate is presented below:
Although reproduction traditionally has been regarded as an aspect of marriage, single persons and gays and lesbians also have interests in having and rearing offspring even if they are not married or partnered to persons of the opposite sex. Some unpartnered women and men are interested in having and rearing children as single parents. Many gays and lesbians already have had children with persons of the opposite sex and share rearing or have sole custody when those relationships end. If they have not adopted or had children, they may wish as single or coupled persons to have offspring for the same reasons of intimacy, companionship, nurturance, family, and legacy that motivate reproduction generally [19].
Given the importance to individuals of having children, there is no sound basis for denying to single persons and gays and lesbians the same rights to reproduce that other individuals enjoy. No state penalizes reproduction per se by unmarried persons, whether achieved coitally or with medical assistance. All states allow unmarried persons, including gays and lesbians, to be foster parents, and the majority of states allow single persons and gay and lesbian couples to adopt [4]. Legal developments make it unlikely that the government could constitutionally ban assisted reproduction to single persons or to gay and lesbian couples, even if same-sex marriage or civil unions are not recognized legally. Moral objection to homosexuality or single parenthood is not itself an acceptable basis for limiting childrearing or reproduction [18].
Many persons who oppose reproduction by single persons or gay or lesbian couples do so out of concern for the welfare of intended offspring. They argue that the best rearing environment for a child is a two-person, married, heterosexual family and are reluctant to assist or facilitate any different arrangement. They may believe that some non-marital arrangements are compatible with a child's welfare, whereas others are not. For example, some fertility programs may treat lesbian, but not gay male couples, or single women, but not single men [17].
A closer look at the reasoning of opponents of assisted reproduction for unmarried persons or for gays and lesbians reveals that there are important differences in the positions taken. Those clinicians who will not treat single females, for example, may believe that fertility treatment should be restricted to married couples, that treatment should be for the infertile only, or that children need a father and a “normal upbringing” [6]. Others may believe that children of gay and lesbian parents will experience social isolation and gender-identity or sexual-orientation problems. One concern with assisting single men to reproduce is that men are perceived as less caring or nurturing than women and that children need a “normal upbringing” with a mother. Some persons also have claimed that children of single men or of gay male couples are at greater risk for sexual abuse, pedophilia, or other mistreatment [9].
The evidence to date, however, cannot reasonably be interpreted to support such fears [7]. A task force of the American Psychological Association has reviewed the existing data and found that there is no scientific evidence that parenting effectiveness is related to parental sexual orientation. Lesbian and gay parents are as likely as heterosexual parents to provide supportive and healthy environments for their children [8].
Research suggests that sexual identities (including gender identity, gender-role behavior, and sexual orientation) develop in much the same ways among children of lesbian mothers as they do among children of heterosexual parents. Studies of other aspects of personal development (including personality, self-concept, and conduct) similarly reveal few differences between children of lesbian mothers and children of heterosexual parents. Evidence also suggests that children of lesbian and gay parents have normal social relationships with peers and adults [11]. Overall results of research suggest that the development, adjustment, and well-being of children with lesbian and gay parents do not differ markedly from that of children with heterosexual parents. A study by Regnerus is often cited to claim that children of same-sex parents fare less well than those of opposite-sex parents [12]. However, this study did not specifically examine children raised by same-sex parents and has since been widely criticized. Among others, a group of over 100 social scientists signed on to a letter to the editor faulting the Regnerus study for failing to take account of family structure and family instability [14].
With regard to outcomes for children of gay male couples, the task force found that fewer data were available. The literature that does exist, however, found no evidence that being raised by a gay father had any negative effect on children [15]. Indeed, identified differences tended to favor the gay fathers. They were found to be more alert to children's needs and more nurturing in providing care than heterosexual fathers, who may see themselves primarily as the person providing financial security [6].
In sum, on the basis of the available evidence, we do not believe that one can reasonably claim that single persons or gays and lesbians harm their children by reproducing outside of heterosexual marital relations. Children born in such situations do not appear to have appreciably better or worse lives than do children born to heterosexual married parents [14]. Given the importance of reproduction to unmarried and gay and lesbian persons and the absence of harm to children from being reared by such parents, it has been found that programs act ethically in assisting unmarried persons or gays and lesbians to reproduce when they meet the same criteria for treatment as married heterosexuals [7].
Despite these social trends and these data, some persons still may view homosexuality as immoral or may oppose facilitating gay and lesbian or unmarried reproduction. As a result, fertility programs may differ in their willingness to provide reproductive services, regardless of the marital status or sexual orientation of prospective patients [15]. Sometimes, the unwillingness to treat is based on religious or personal moral views about the propriety or desirability of unmarried persons or gays and lesbians having children. At other times it may reflect the administrative complications of working with egg donors or surrogate mothers that assistance to gay male individuals or couples entails [8].
As a matter of law, fertility programs may be prohibited from denying assisted reproductive technology (ART) services to patients on the basis of their marital status or sexual orientation [16]. In 2008, the California Supreme Court ruled that refusal to treat a lesbian patient based on the physician's religious views violated state law. The court found that assertions of religious freedom are pre-empted by state law that prohibits discrimination in public accommodations based on sexual orientation [9]. Since medical offices are considered public accommodations under civil rights laws, and approximately half of all states ban discrimination on the basis of marital status, with another third banning discrimination on the basis of sexual orientation, provider autonomy may not protect physicians who refuse ART services based on patient demographic characteristics [10].
As a matter of ethics, this Committee believes that the ethical duty to treat persons with equal respect requires that fertility programs treat single persons and gay and lesbian couples equally to heterosexual married couples in determining which services to provide [12]. Other professional organizations have expressed support for nondiscriminatory access to assisted reproduction including the American College of Obstetricians and Gynecologists, which said of physicians who refuse to provide infertility services to samesex couples: “Allowing physicians to discriminate on the basis of sexual orientation would constitute a deeper insult, namely reinforcing the scientifically unfounded idea that fitness to parent is based on sexual orientation, and, thus, reinforcing the oppressed status of same-sex couples” [11].
Unless other aspects of the situation also would disqualify heterosexual married couples or individuals from services, such as serious doubts about whether they will be fit or responsible childrearers or the fact that the program does not offer anyone a desired service, for example, gestational surrogacy, there is no sound ethical basis for licensed professionals to deny reproductive services to unmarried or gay and lesbian persons [13].
Fertility Treatment for Surrogates
Surrogacy is when another woman carries and gives birth to a child for you. Though it can be an emotionally intense and legally complex arrangement, it is growing in popularity among parents as a way of having children. Surrogacy requires a lot of time, money and patience to succeed, whether it's carried out privately or through an agency. But it can bring happiness to all concerned if the medical, legal, financial and emotional aspects are properly considered.
The risks associated with surrogacy depend on the type of surrogacy (full or partial) undertaken. Generally, the risks associated with full surrogacy are similar to those for IVF. It is quite difficult to determine a success rate for surrogacy, as many factors are relevant,including:
• the surrogate’s ability to get pregnant,
• the age of the egg donor (if involved),
• the success of procedures such as IUI and IVF, and
• the quality of gamete provided by the commissioning couple.
The age of the woman who provides the egg is the most important factor that affects chances of pregnancy. The Foreign and Commonwealth Office (FCO) has launched guidance on surrogacy overseas to give parents information about the process to help inform them of the sort of issues they may face when embarking on a surrogacy arrangement in a foreign country. The guidance urges prospective parents to ensure they are fully aware of the facts and are well prepared before starting what can be a long and complex process.
“Natural surrogacy” is when a healthy woman with normal ovaries, tubes and uterus is inseminated with sperm from the husband of a woman who is unable to carry a baby. If the surrogate woman becomes pregnant and has the baby, then the woman who cannot have the baby and her husband with whom she was originally inseminated adopt the baby. It is unethical for Fertility Associates to assist with natural surrogacy, such as by undertaking the insemination, without prior approval of the Ethics Committee on Assisted Reproductive Technology (ECART). The ECART is a ministerial committee established under section 27 of the HART Act that reviews, determines and monitors applications for assisted reproductive procedures and human reproductive research.
“IVF surrogacy”, on the other hand, is when the woman who is unable to bear the child has normal ovaries but is still unable to bear a child, undergoes IVF hormone stimulation and egg pickup (OPU), with fertilization of the eggs by her husband’s sperm.
Then their embryos are transferred to the surrogate. The surrogate must be healthy, have a low risk for complications during any pregnancy that occurs and be willing, after delivery, to give the baby to the genetic parents from whose egg and sperm it was conceived.
The ethical and legal issues associated with surrogacy are not simple. The ECART requires Fertility Associates to make an application in one or two stages. Considerable consultation and counseling is usually required before the application can be made. Fertility Associates is very supportive of IVF surrogacy when the woman who would carry the baby is a family member or a close personal friend of the couple who need surrogacy, especially if they have completed their family. Once approved the IVF treatment can normally proceed quickly. There is very limited public funding for IVF surrogacy and specific criteria need to be met.
New California Healthcare Laws: Gay and Lesbian Discrimination for Fertility Treatment
The law entitled “AB 460: Non-Discrimination for Homosexuals and Lesbians” requires coverage under the Knox-Keene Health Care Service Plan Act and a under a policy of health insurance that provides for coverage for the treatment of infertility. If such coverage is offered and purchased, it must be provided without discrimination on the basis of:
• age
• ancestry
• color
• disability
• domestic partner status
• gender
• gender expression
• gender identity
• genetic information
• marital status
• national origin
• race, religion
• sex or
• sexual orientation.
AB 460 extended the idea of “non-discrimination” in this context to homosexuals and lesbians regarding fertility. If a health insurance plan is purchased that contains coverage for infertility, then the plan must not discriminate. This statute is meant to help all people access to treatment of infertility. Insurance plans are not required to carry such coverage. There will be a violation of the statute only if the plan does offer such coverage and they attempt discrimination in the utilization of the coverage. The law makes homosexuals and lesbians eligible for insurance coverage for “treatment of infertility, except in vitro fertilization, under those terms and conditions as may be agreed upon between the group subscriber or the group policyholder and the plan or the insurer”.
An interesting issue arises when the definition of infertility is considered. Under the new law, homosexuals and lesbians will be classified as ‘infertile’ if they are unable “to conceive a pregnancy or to carry a pregnancy to a live birth after a year or more of regular sexual relations without contraception”. Since most sexual relations in a homosexual and lesbian relationship do not result in pregnancy, the law effectively defines all homosexuals and lesbians as “infertile.” Surely this is an unintended result and new legislation will need to be considered in the near future [20].
Legal and Ethical Issues and Fertility Treatment Abroad
Fertility treatment can be a minefield of legal and ethical issues. These vary from country to country, but also by religious beliefs within those countries. Each one of us also has our own personal opinions, which complicate things even more.
The countries with laws and statutes covering the legal issues of fertility treatment include:
•Canada
• France
• Finland
• Germany and
• UK.
The countries where legal issues around fertility treatment are left to official guidelines include:
• Australia
• Cyprus
• India
• Mexico
• Poland, and
• USA
Ethical issues can be even more complicated than legal ones, and it is often up to you as an individual to decide what you are comfortable with. For many people, the act of conception is holy and sacrosanct, and should not be interfered with in any way. For others, having a baby is the most important thing, and the methods involved do not worry them. There is a whole spectrum of views and opinions that lies in between these two.
A substantial number of UK patients are travelling abroad for fertility treatment. Their motivations may include lower costs for treatment and greater availability of donors. Many patients have positive experiences of receiving treatment abroad; although, this is not always the case.
Final Words
Although the majority of births still occur within the context of heterosexual married couples, variations abound. Marital reproduction no longer is solely coital and may include a third-party gamete donor or a surrogate carrier. The incidence of births to single or unmarried persons also has grown, including among never-married, college-educated, professional women. A growing number of professional women without male partners have chosen to have children, sometimes with the help of donor insemination. Ethical arguments supporting denial of access to fertility services on the basis of marital status or sexual orientation cannot be justified.
References
- Golombok S, Spencer A, Rutter M. (1983). “Children in lesbian and singleparent households: psychosexual and psychiatric appraisal”.Journal of Child Psychology and Psychiatry 24:551–72.
- Siegel J. M. (1995). “Looking for Mr. Right? Older single women who become mothers”.Journal of Family Issues 16:194–211.
- Daar J. F. (2008). “Accessing reproductive technologies: invisible barriers, indelible harms”. Berkeley Journal of Gender. Law & Justice 23:18–82.
- Robertson J. A. (2004). “Gay and lesbian access to assisted reproduction”. Case West Reserve Law Review 55:323–72.
- Dunstan G. R. (1975) Ethical aspects of donor insemination. Journal of Medical Ethics 1:42-4.
- Fletcher J. C. (1985) “Artificial insemination in lesbians: ethical considerations”. Arch Intern Med 145:419–20. [7]. Maccallum F, Golombok S. (2004) “Children raised in fatherless families from infancy: a follow-up of children of lesbian and single heterosexual mothers at early adolescence”.Journal of Child Psychology and Psychiatry 45:1407–19.
- Gartrell N, Bos H. (2010) “US National Longitudinal Lesbian Family Study: psychological adjustment of 17-year-old adolescents”. Pediatrics 126: 28–36.
- Chan R. W, Raboy B, Patterson C. J. (1998) “Psychosocial adjustment among children conceived via donor insemination by lesbian and heterosexual mothers”. Child Development 69:443–57.
- Golombok S, Badger S. (2010). “Children raised in mother-headed families from infancy: a follow-up of children of lesbian and single heterosexual mothers, at early adulthood”.Human Reproduction 25:150–7.
- Golombok S, Tasker F, Murray C. (1997) “Children raised in fatherless families from infancy: family relationships and the socio-emotional development of children of lesbian and single heterosexual mothers”. Journal of Child Psychology and Psychiatry 38:783–91.
- Murray C, Golombok S. (2005) “Solo mothers and their donor insemination infants: follow-up at age 2 years”. Human Reproduction 20:1655–60.
- Regnerus M. (2012) “How different are the adult children of parents who have same-sex relationships? Findings from the New Family Structures Study”. Social Science Research 41:750–70.
- Bigner J. J. (1999) “Raising our sons: gay men as fathers”. J Gay Lesbian Society Service 10:61–8.
- Bailey J. M, Bobrow D, Wolfe M, Mikach S. (1995) “Sexual orientation of adult sons of gay fathers”. Development Psychology 31:124–9.
- Bozett F. W. (1985) “Gay men as fathers”. Dimensions of fatherhood. Beverly Hills, CA: Sage: 327–52.
- Wainwright J. L, Russell S. T, Patterson C. J. (2004) “Psychosocial adjustment, school outcomes, and romantic relationships of adolescents with same-sex parents”. Child Development 75:1886–98.
- Bigner J. J, Jacobsen R. B. (1989) “Parenting behaviors of homosexual and heterosexual fathers”. Journal of Homosex 18:173–86.
- Barter B. L, Robinson B. E. (1990) “Gay fathers”. Lexington, MA: DC Heath.
- New California Healthcare Laws: Gay and Lesbian Discrimination for Fertility Treatment,www.californiahealthcarelaw.com/?p=108.
- www.en.wikipedia.org/wiki/Assisted_reproductive_technology





