Mifepristone Plus Vaginal Misoprostol V/S Vaginal Misoprostol Alone for Medical Termination of Pregnancy
Sreeja G R1*, Patsy Vargese2, Anitha3 K G
1 Asst.Professor Department of Obstetrics & Gynaecology, Shri.B.M.Patil Medical College and Research Centre, Bijapur, India.
*Corresponding Author
Sreeja G R,
Asst.Professor Department of Obstetrics & Gynaecology,
Shri.B.M.Patil Medical College and Research Centre,
Bijapur, India.
E-mail: dr.sreejagr@yahoo.com
Received: July 30, 2014; Accepted: August 21,2014; Published: August 23, 2014
Citation: Sreeja G R, Patsy Vargese, Anitha K G (2014) Mifepristone Plus Vaginal Misoprostol V/S Vaginal Misoprostol Alone for MedicalTermination of Pregnancy, Int J Reprod Fertil Sex Health. 1(2), 7-13. doi: dx.doi.org/10.19070/2377-1887-140002
Copyright: Sreeja G R © 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium,provided the original author and source are credited.
Abstract
Medical abortion has been investigated as a non-invasive option for early abortions as it avoids the risk of anesthesia and surgical trauma to the cervix, uterus and other organs.
The main aim of the study was to compare the efficacy and safety of abortion using the drugs mifepristone and vaginal misprostol V/s misoprostol alone.
A randomized control study was done in 100 women who came for termination of pregnancy up to 63 days in family planning unit at Government Medical College Hospital, Kottayam, India for one year period.
The mean age of the study group was 25.4 years of age. Complete abortion occurred in 94% with Mifepristone and Misiopristol regime (Group A) and 86% of Misoprostol alone regimn(Goup B). There was a 100% complete abortion rate with mifepristone and misoprostol in POGs up to 49 days. Complete abortion showed better compliance with Misoprolstol alone regimn in Primigravida (100%) and, Mefepristone and Misoprostol regime with multigravida (97%). The mean period of bleeding was 5.7 in Group A and 7.6 in Group B.
Mifepristone and Misiopristol regime showed better outcome than Misoprostol alone for medical termination of pregnancy till first 9 weeks of gestation
2.Abbreviations
3.Introduction
4.Objectives
5.Material and Methods
5.1.Study design
5.2.Study setting
5.3.Case definition
6.Inclusion Criteria
7.Exclusion Criteria
7.1.Sampling
8.Study Method
8.1.Analysis
9.Discussion
10.Observations
11.References
Keywords
Mifepristone, Misiopristol, Medical termination of pregnancy
Abbreviations
MTP -Medical Termination of Pregnancy
IUD -Intra Uterine Device
MVA - Manual Vacuum Aspiration
EVA - Electric Vacuum Aspiration
D&E - Dilatation and Evacuation
Introduction
Abortion is defined as the termination of pregnancy by the removal or expulsion from the uterus of a fetus or embryo prior to viability. An abortion can occur spontaneously, in which case it is usually called a miscarriage, or it can be purposely induced. The term abortion most commonly refers to the induced abortion of a human pregnancy.
Medical abortion besides being private, convenient and less invasive has been found to alleviate the complication of surgically performed abortion. For termination of early pregnancy, the efficacy and tolerability of mifepristone in combination with vaginal misoprostol have already been established.
The Indian abortion laws fall under the Medical Termination of Pregnancy (MTP) Act, which was enacted by the Indian Parliament in the year 1971. The MTP Act came into effect from April 1, 1972 and was once amended in 1975.
The Medical Termination of Pregnancy (MTP) Act of India clearly states the conditions under which a pregnancy can be ended or aborted, the persons who are qualified to conduct the abortion and the place of implementation.
Mifepristone is a synthetic steroid compound used as a pharmaceutical. It is a progesterone receptor antagonist used as an abortifacient in the first months of pregnancy, and in smaller doses as an emergency contraceptive.
Misoprostol, a prostaglandin, binds to myometrial cells to cause strong myometrial contractions leading to expulsion of tissue. Misoprostol is commonly used for labor induction. It causes uterine contractions and the ripening (effacement or thinning) of the cervix.
Oral mifepristone (Ru 486) in doses of 200-600 μg has been successfully used in pregnancy termination up to 63 days, in combination with misoprostol administered orally in doses of 400 – 800 μg or vaginally either simultaneously or increasing dosing intervals. Antiprogestin Ru 486 discovered in France is widely popular in the country of its origin where it is used in association with orally administered mifepristone, unlike the vaginally inserted that is favour in other centers.
The combination of mifepristone is acceptable in various European nations such as the UK, USA or any other affluent nation where the high cost of mifepristone is not a big problem. Where as for women living in developing countries, misprostol, a prostaglandin E1 analogue like gemeprost, became more acceptable as it is cheaper and can potentially induce uterine contractions, thereby facilitating abortion with a successful rate of above 85%. Misoprostol has been combined with methotrexate (both oral and intramuscular) with similar results or with tamoxifen which has given mixed results.
In this respect, I tried to adopt a World Health Organization – developed, effective, evidence-based regimen (developed in 2003) for early trimester pregnancy termination, consisting of 200 mg mifepristone given orally followed 24 hrs by vaginal misoprostol 400 μg 4th hourly to a maximum of five doses which has been found to be more effective than same dose of misoprostol alone used vaginally.
My aim was to explore whether the combination of mifepristone and misoprostol could bring an improvement in the complete abortion rate in women, which was 85% with the use of vaginal misoprostol alone and to compare the side effects.
Objectives
1. To determine the clinical advantage of pre treatment with Mifepristone in early pregnancy termination
2. To compare the efficacy of a combination of Mifepristone with vaginal Misoprostol with vaginal Misoprostol alone for medical abortion.
3. To compare the side effects between the combination of Mifepristone with vaginal Misoprostol with vaginal Misoprostol alone for medical abortion.
Material and Methods
Hospital based Randomized Controlled Trial
Family Planning unit at tertiary care teaching hospital, Government Medical College Hospital, Kottayam.
Women who came for termination of pregnancy up to 63 days to the family planning unit at Government Medical College Hospital, Kottayam over the period of one year ranging from may 2011 to May, 2012 and were selected at random for the study.
Inclusion Criteria
• Women who need termination of pregnancy due to various reasons.
• Primigravida or women with history of normal labour.
• TVS demonstrating a live intra uterine pregnancy up to 63 days gestation with visibility of fetal pole or mass with cardiac activity.
• Estimated Hb level 10 gm% or more.
• Blighted ovum
• Incomplete or missed abortion
• IUCD co-existing with pregnancy
• Scarred uterus
• Anemia
• Medical diseases
• Inherited porphyria
• H/o allergy to drugs in trial
Patients in the Family Planning OP, Government Medical College Hospital, Kottayam, India.
Study Method
Women requesting termination of pregnancy within 9 weeks from the onset of amenorrhea will be recruited for the study. Women who enrolled will be given written informed consent and agreed to have suction evacuation should the pregnancy be viable at the follow-up visit or anytime if heavy bleeding occurs.
The gestational age will be confirmed in all women by Trans vaginal scan examination. Randomized cards based on computer generated random numbers will be stocked in FP unit and patients are allocated accordingly. The patients who receive Mifepristone Misoprostol combination trial are given Mifepristone 200 mg oral from OP and advised to come on next day. Patient in both trial group are admitted in hospital for proper observation on the day of Misoprostol trial. If the patient’s blood type is Rh negative, she will be given Inj anti D intramuscularly. Patients in both groups will be given Misoprostol 400 mcg 4th hrly up to a 5 maximum doses. Patient’s vitals will be monitored soon after the administration of vaginal misoprostol and then at 3rd hr for each dose. The patients are kept under observation until they undergo complete abortion or till the end of the 5th dose which ever is earlier. At the end of the 5th dose the patients are allowed to go home.
Patients will be asked to record the onset of bleeding, timing of passage of products of conception, duration of bleeding, and side effects for the next 14 days. They will also be instructed to come to hospital in case of heavy bleeding (soaking of more than 2 pads per hour for more than 2 hrs or severe pain or any othercomplication. They will be asked to come for a follow-up visit on day 15 when vaginal examination and pelvic ultrasound examination will be carried out. For each woman, the outcome will be classified into one of the following categories.
(I) Complete abortion,
(ii) Incomplete abortion,
(iii) Continuing pregnancy.
In complete abortion the uterine cavity will be empty and the endometrial thickness will be less than 15 mm through the TVS. In incomplete abortion there may be retained products of conception and endometrial thickness will be less than 15 mm. In missed abortion the gestational sac may be present but without any cardiac activity in embryo. In continuation of pregnancy the live fetus is present in the gestational sac. Women with treatment outcomes in the last three categories will be further managed by suction evacuation of the uterus. Success will be defined as complete expulsion of the products of conception with no need for surgical intervention.
The induction abortion interval is defined as the time interval from administration of Mifepristone in Mifepristone Misoprostol combination trial group and from administration of misoprostol in misoprostol only group to the passage of products of conception
Maternal details were entered in the computer [Excel data sheet (Appendix)] and analyzed using SPSS 11.
Discussion
From this study of medical abortion in <63 days ‘gestation', the success rate of complete abortion with mifepristone 200 mcg followed by vaginal misoprostol was 94%, compared to success rate of 86% for vaginal misoprostol used alone in repeated doses. Surgical evacuation was needed in 10 cases; seven for cases of incomplete abortion -three in group a (6%) and four in group B (8%) and the other three evacuations were performed for pregnancy continuation in group B (6%)
In total more favourable outcome were observerd with the combination of mifepristone and misprostol giving a complete abortion rate that is equal to or slightly less then other studies carried out in pregnancy of≤ 63 days. Almost all of these studies achieving success rates of 95% have invariably incorporated a large number of subject ranging from 800-1200. 2,4,5-7,14,18 One such study ‘ Low dose mifepristone 200 mcg and vaginal misoprostol for abortion’ conducted by Schaff E.A ,Essenger S.H, and Stadalius L.S at Dept of family medicine , Rochester University of Medicine ,Newyork in 933 women showed complete abortion rate of 97%. Nevertheless, there are some studies that have been tried in small number of women 12,17,19,23 Another study ‘Mifepristone plus vaginal misoprostol vs vaginal misoprostol alone for medical abortion in first trimester conducted by Rashmi Chawdhary,Ashma Rana and Neelam Pradhan in Thribhuvan University , Kathmandu among 194 women showed a complete abortion rate of 95% in the combination group.
A large multi centric Cochrane data base analysis conducted by WHO on Medical methods of first trimester abortion reviewed 58 trials out of which 5 trials compared the efficacy of prostaglandin alone to combination regimen of prostaglandin and mifepristone. All these trials showed higher effectiveness with combination trial.
Regarding gravidity, with the exception of two incomplete abortions which occurred in group A, the rest of the Primigravida (90.4%) aborted completely. This was almost equal to the complete abortion rate in multigravida (89.8%). Incomplete abortion (9.5%) in Primigravida, however was more frequent than multigravida (6.3%) but without any significant differences, while pregnancy continuation occurred only in multigravida (3.8%) and all of them belong to Group B. In group B, pregnancy continuation (three) and incomplete abortion (four) occurred in multigravida (seven). In group A, incomplete were seen more in Primigravida (two) than multigravida(one).
Gestational age is one of the parameters for the success of the medical abortion. Medical abortion with misoprostol failed in three women in group B when their gestational age in days was <56 days (35,36,53 days). Further, in the case of incomplete abortion, the gestational age was 51,62 and 63 days (Group A) or 39,56 and 63 days (Group B). Yet the mifepristone and misoprostol regime resulted in a 100% complete abortion rate when the duration of amenorrhea was <49 days. This is an impressive finding compared to the research conducted for confirming the safety and efficacy in pregnancy <49 days which gave success rate below 100% 19,21. Efficacy, however decreased significantly when the duration of pregnancy was more than 49-63 days of amenorrhea.
A study worth mentioning is ‘ Misoprostol for abortion up to 9 wks gestation in adolescents’ by Velazco A, Valera L et al compared 800μg vaginal misoprostol in its normal form without wetting or using the water- wet form inserted on days 1, 3 and 5 resulting in a complete abortion rate of 85% Further, the success rate was stretched up to 88% in 150 adolescents with a similar dosing interval and dosage of vaginal misoprostol in normal forms. However the success rate of vaginal misopristol alone was only 85-88% in comparison to its combination with mifepristone, which gave a success rate of above 92%. On the basic of the lower success rate, there are contradicting views as to whether it is appropriate or not to use misoprostol for pregnancy termination.
Misoprostol is usually associated with more side effects such as nausea vomiting, diarrhea, fever and shivering, and with the exception of one study , mifepristone has appeared to have fewer side effect 5,14,15,22,23. One of the main disadvantages that could reduce the acceptability of medical abortion is its longer duration of bleeding, which was also observational finding in this study.
The percentage of complete abortion after first dose of misoprostole in group A was 23% and after each subsequent dose of the drug was 59%,86%,92% and 94%, while in group B it was 18%,42%,69%,83%,86%.
One the whole, this experimental study has shown safety, tolerability and a better success rate when the combination regime of oral mifepristone and vaginal misoprostol is used, congruous to other study findings 4,5,14,. Probably success rate could have improved had we implicated the insertion used a different dosing interval schedule of 4-8 or 5 days.
There are a number of limitations that should be noted, as this preliminary study with a small sample size was not really big enough to measure differences. Even with a complete abortion judged by ultrasound in six cases, the second treatment with misoprostol repeated on day 3 could have reduced the duration and amount of bleeding. Efficacy rates could have been improved with a longer window period than just 24hrs.
Observations
A total of 100 women were included in the study group which comprises 50 women from Mifepristone + Misoprostol [GROUP A] and 50 women from Misoprostol alone [GROUP B] after satisfying the inclusion and exclusion criteria. Various findings of the study are presented and tabulated as follows .
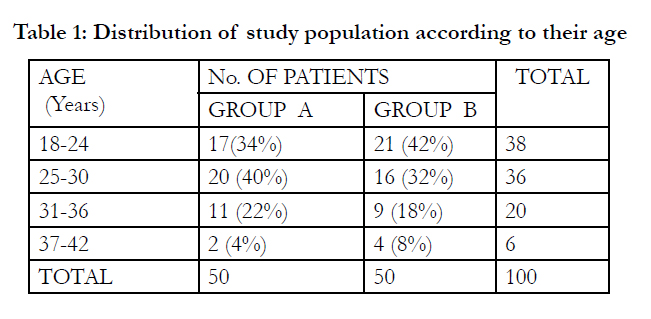

Table 1: Distribution of study population according to their age.
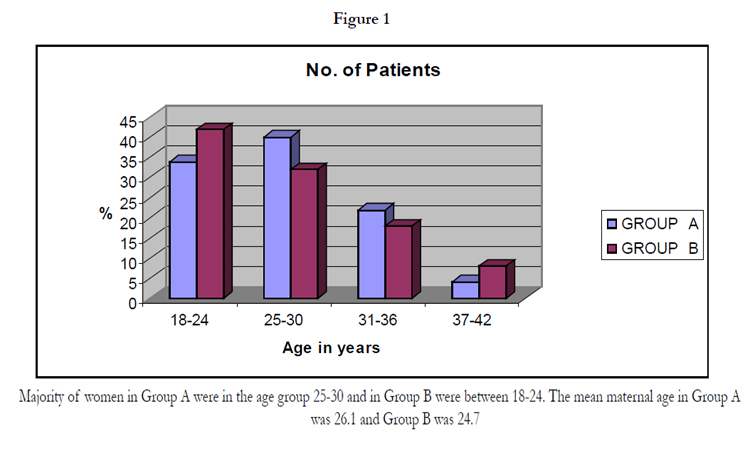
Figure 1.
Majority of women in Group A were in the age group 25-30 and in Group B were between 18-24. The mean maternal age in Group A was 26.1 and Group B was 24.7
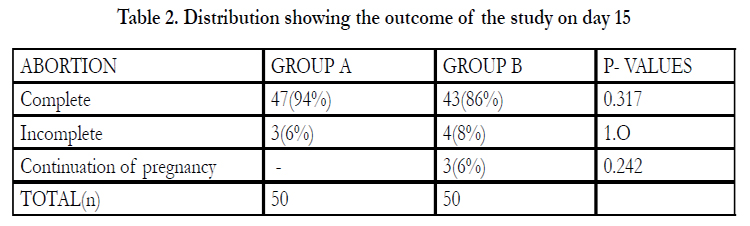
Table 2. Distribution showing the outcome of the study on day 15.
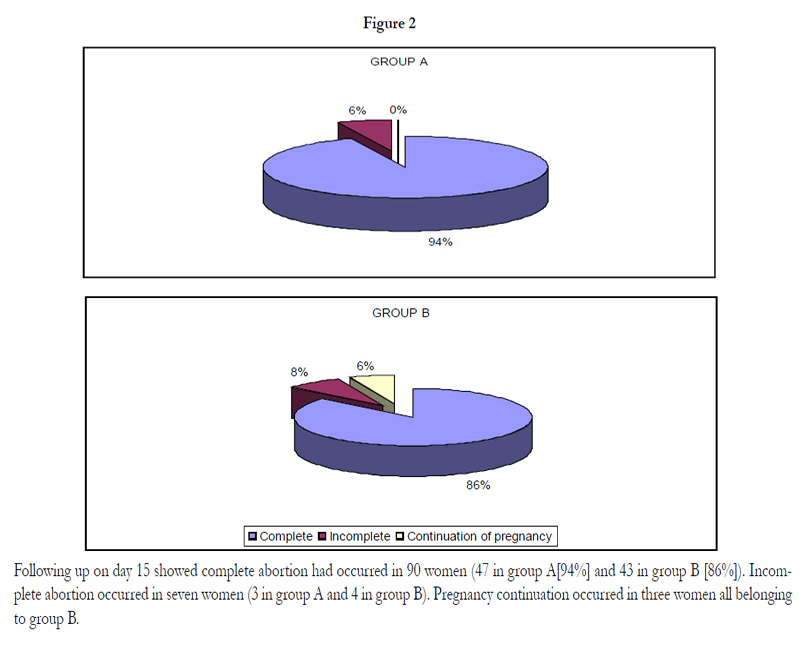
Figure 2.
Following up on day 15 showed complete abortion had occurred in 90 women (47 in group A[94%] and 43 in group B [86%]). Incomplete abortion occurred in seven women (3 in group A and 4 in group B). Pregnancy continuation occurred in three women all belonging to group B.
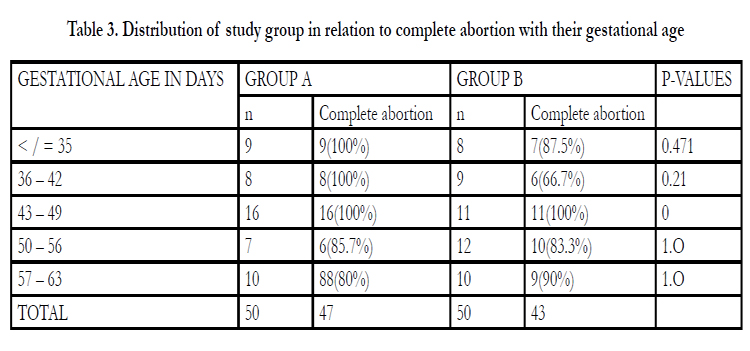
Table 3. Distribution of study group in relation to complete abortion with their gestational age.
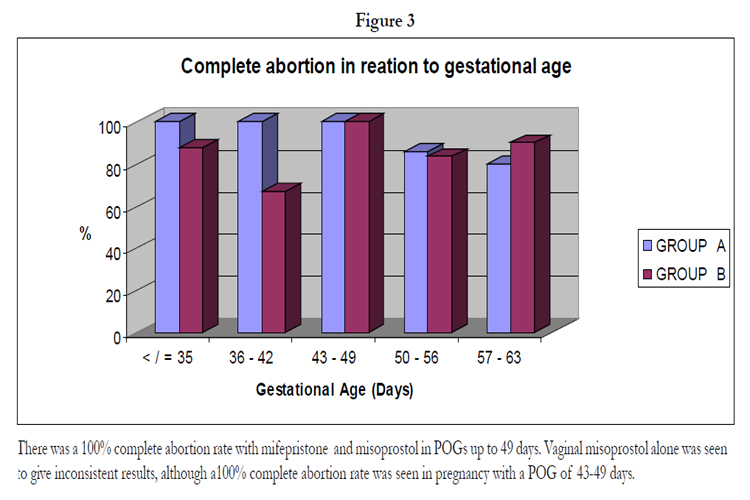
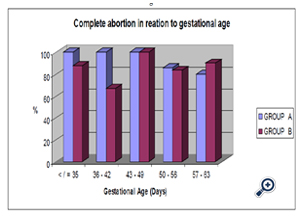
Figure 3.
There was a 100% complete abortion rate with mifepristone and misoprostol in POGs up to 49 days. Vaginal misoprostol alone was seen to give inconsistent results, although a100% complete abortion rate was seen in pregnancy with a POG of 43-49 days.
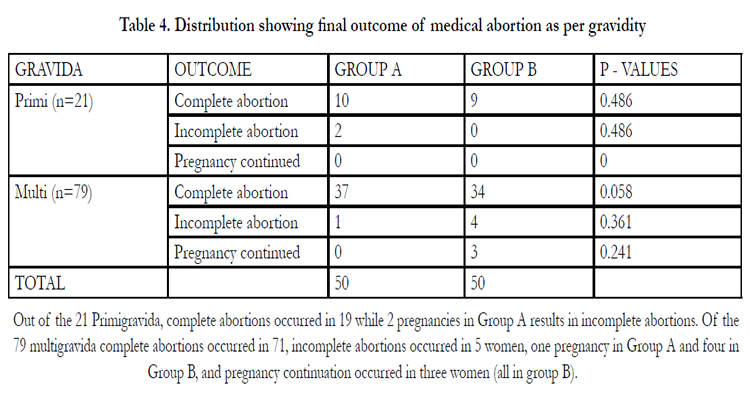
Table 4. Distribution showing final outcome of medical abortion as per gravidity.
Out of the 21 Primigravida, complete abortions occurred in 19 while 2 pregnancies in Group A results in incomplete abortions. Of the 79 multigravida complete abortions occurred in 71, incomplete abortions occurred in 5 women, one pregnancy in Group A and four in Group B, and pregnancy continuation occurred in three women (all in group B).
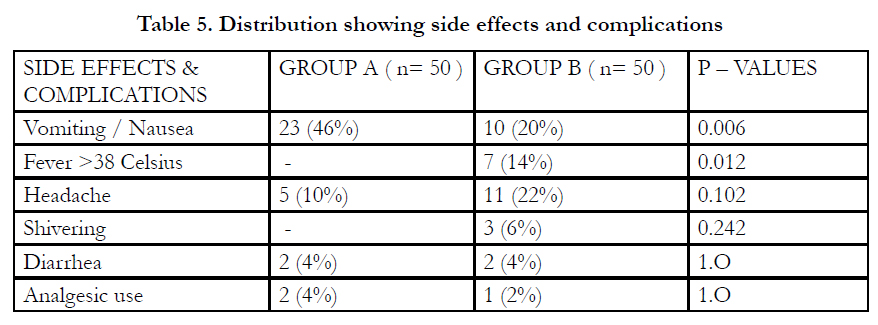
Table 5. Distribution showing side effects and complications.
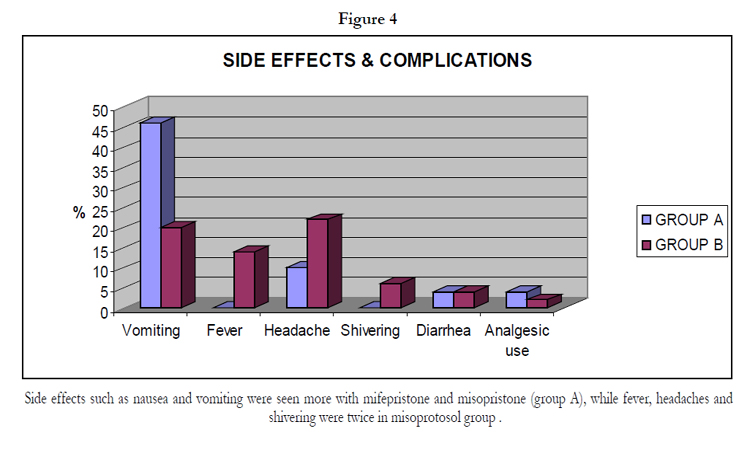
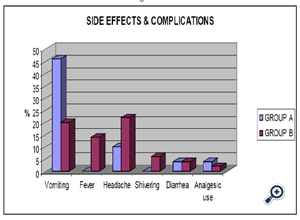
Figure 4.
Side effects such as nausea and vomiting were seen more with mifepristone and misopristone (group A), while fever, headaches and shivering were twice in misoprotosol group .
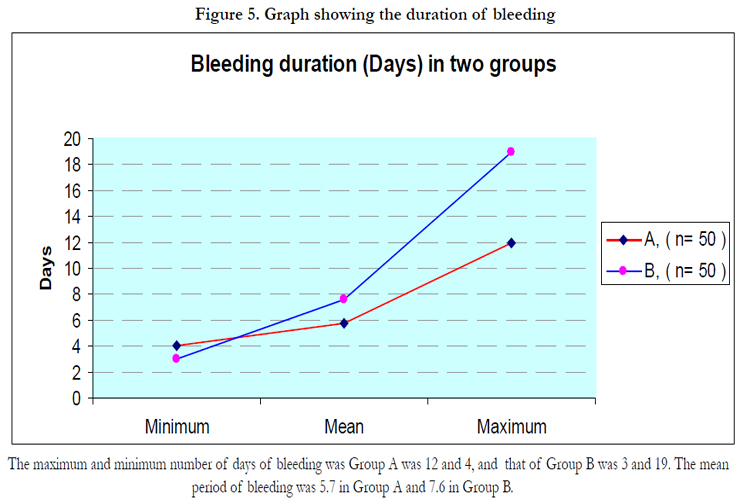
Figure 5.
The maximum and minimum number of days of bleeding was Group A was 12 and 4, and that of Group B was 3 and 19. The mean period of bleeding was 5.7 in Group A and 7.6 in Group B.
References
- Hou SP, Fang AH, Chen QF, Huang YM, Chen OJ, et al. (2011 ) Termination of second-trimester pregnancy by mifepristone combined with misoprostol versus intra-amniotic injection of ethacridine lactate (Rivanol®): a systematic review of Chinese trials .Contraception 84(3):214-23.
- Cheng L, Gülmezoglu AM, Oel CJ, Piaggio G, Ezcurra E,et al. (2008) Interventions for emergency contraception. Cochrane Database Syst Rev (2).
- Kulier R, Fekih A, Hofmeyr GJ, Campana A (2001) Surgical methods for first trimester termination of pregnancy .Cochrane Database Syst Rev (4).
- Ngoc NT, Blum J, Raghavan S, Nga NT, Dabash R, et al. (2011) Comparing two early medical abortion regimens: mifepristone+misoprostol vs. misoprostol alone. Contraception 83(5):410-7.
- Kulier R, Gülmezoglu AM, Hofmeyr GJ, Cheng LN, Campana A (2004) Medical methods for first trimester abortion. Cochrane Database Syst Rev(2).
- Say L, Kulier R, Gülmezoglu M, Campana A (2005) Medical versus surgical methods for first trimester termination of pregnancy. Cochrane Database Syst Rev 25(1).
- Lohr PA, Hayes JL, Gemzell-Danielsson K (2008) Surgical versus medical methods for second trimester induced abortion. Cochrane Database Syst Rev 23(1).
- Tang OS, Mok KH, Ho PC (2004) A randomized study comparing the use of sublingual to vaginal misoprostol for pre-operative cervical priming prior to surgical termination of pregnancy in the first trimester . Hum Reprod 19(5): 1101-1105.
- Aronsson A, Bygdeman M, Gemzell-Danielsson K (2004) Effects of misoprostol on uterine contractility following different routes of administration .Hum Reprod 19(1): 81-84.
- Wong CY, Ng EH, Ngai SW, Ho PC (2002) A randomized, double blind, placebo-controlled study to investigate the use of conscious sedation in conjunction with paracervical block for reducing pain in termination of first trimester pregnancy by suction evacuation. Hum Reprod 17(5): 1222-1225.
- Tang OS, Schweer H, Seyberth HW, Lee SW, Ho PC (2002) Pharmacokinetics of different routes of administration of misoprostol . Hum Reprod 17(2).
- Ngai SW, Chan YM, Ho PC (2001) The use of misoprostol prior to hysteroscopy in postmenopausal women. Hum Reprod 16(7): 1486-1489.
- Guest J, Chien PF, Thomson MA, Kosseim ML (2007) Randomised controlled trial comparing the efficacy of same-day administration of mifepristone and misoprostol for termination of pregnancy with the standard 36 to 48 hour protocol. BJOG 114(2):207-15.
- Creinin MD, Schwartz JL, Pymar HC, Fink W (2001) Efficacy of mifepristone followed on the same day by misoprostol for early termination of pregnancy: report of a randomised trial. BJOG 108(5):469-73.
- Schaff EA, Eisinger SH, Stadalius LS, Franks P, Gore BZ,et al. (1999) Lowdose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception. 59(1):1-6.
- Kulier R, Gülmezoglu AM, Hofmeyr GJ, Cheng LN, Campana A (2004) Medical methods for first trimester abortion. Cochrane Database Syst Rev (1).
- World Health Organization Task Force on Post-Ovulatory Methods for Fertility Regulation. Termination of pregnancy with reduced doses of mifepristone (1993). BMJ 307:532-8.
- McKinley C, Thong KJ, Baird DT (1993) The effect of dose of mifepristone and gestation on the efficacy of medical abortion with mifepristone and misoprostol. Hum Reprod 8:1502-5.
- World Health Organization Task Force on Post-Ovulatory Methods for Fertility Regulation. Comparison of two doses of mifepristone in combination with misoprostol for early medical abortion: a randomized trial (2000). BJOG 107:524-30.
- Schaff EA, Fielding SL, Westhoff C (2001) Randomized trial of oral versus vaginal misoprostol at one day after mifepristone for early medical abortion. Contraception 64:81-5.
- Von Hertzen H, Honkanen H, Piaggio G, Bartfai G, Erdenetungalag R,et al. (2003) WHO multinational study of three misoprostol regimens after mifepristone for early medical abortion. I: efficacy. BJOG 110:808-18.
- Honkanen H, Piaggio G Hertzen, H, Bartfai G, Erdenetungalag R, Gemzell- Danielsson K, et al. (2004) WHO multinational study of three misoprostol regimens after mifepristone for early medical abortion. BJOG 111:715-25.
- Middleton T, Schaff E, Fielding SL, Scahill M, Shannon C,et al. (2005) Randomized trial of mifepristone and buccal or vaginal misoprostol for abortion through 56 days of last menstrual period. Contraception 72:328-32.
- Hamoda H, Ashok PW, Dow J, Flett GM, Templeton A (2003) A pilot study of mifepristone in combination with sublingual or vaginal misoprostol for medical termination of pregnancy up to 63 days gestation. Contraception 68:335-8.
- Hamoda H, Ashok PW, Flett GM, Templeton A (2005) A randomised controlled trial of mifepristone in combination with misoprostol administered sublingually or vaginally for medical abortion up to 13 weeks of gestation. BJOG 112:1102-8.
- Creinin MD, Schwartz JL, Pymar HC, Fink W (2001) Efficacy of mifepristone followed on the same day by misoprostol for early termination of pregnancy: report of a randomised trial. BJOG 108:469-73.
- Creinin MD, Fox MC, Teal S, Chen A, Schaff EA, et al. (2004) A randomized comparison of misoprostol 6 to 8 hours versus 24 hours after mifepristone for abortion. Obstet Gynecol 103:851-9.
- Spitz IM, Bardin CW, Benton L, Robbins A (1998) Early pregnancy termination with mifepristone and misoprostol in the United States. N Engl J Med 338:1241-7.
- Schaff EA, Eisinger SH, Stadalius LS, Franks P, Gore BZ, et al. (1999) Lowdose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception 59:1-6.
- Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD (1997)Absorption kinetics of misoprostol with oral or vaginal administration. Obstet Gynecol 90(1):88-92.
- Pymar HC, Creinin MD, Schwartz JL (2001) Mifepristone followed on the same day by vaginal misoprostol for early abortion. Contraception 64:87-92.
- Fox MC, Creinin MD, Harwood B (2002) Mifepristone and vaginal misoprostol on the same day for abortion from 50 to 63 days' gestation. Contraception 66:225-9.
- Honkanen H, Piaggio G, Hertzen H, Bártfai G, Erdenetungalag R, et al. (2004) WHO multinational study of three misoprostol regimens after mifepristone for early medical abortion.BJOG 111:715-725.
- Ashok PW, Penny GC, Flette GM (2001) An effective regimen for early medical abortion: A report of 2000 consecutive cases. Hum Reprod 16:2962-2965.





