Clinical Versus Echographic Estimation of Fetal Weight at Term in A Selected Caucasian Milieu: A Comparative Analysis of The Kongnyuy – Mbu’s Clinical Estimation
Ronbinson Enow Mbu1*, Izaac Mboh Eyong2, William Ako Takang3, Eugene Kornyuy4, Cyril Faraquet5, Souhaide Antoine5, Eric Louis5, Vincente Liliann5, Gilles Body5, Robert Joseph – Ivo Leke6
1 Department of Obstetrics and Gynecology, Faculty of Medicine and Biomedical Sciences, University of Yaounde 1, Cameroon.
2 Department of Obstetrics and Gynecology, Yaounde Military Hospital, Cameroon and Regional Hospital Centre, Chatre, France.
3 Department of Obstetrics and Gynecology, University of Bamenda, Cameroon.
4 The United Nations Population Fund, Democtratic Republic of Congo.
5 Regional Hospital Centre, Chartres, France.
6 Professor Emeritus, Department of Obstetrics and Gynecology, Faculty of Medicine and Biomedical Sciences, University of Yaounde 1, Cameroon.
*Corresponding Author
Robinson Enow Mbu,
Department of Obstetrics and Gynecology, Faculty of Medicine and Biomedical Sciences,
University of Yaounde 1, Cameroon.
Tel: (237) 77 57 51 31/99 93 44 56/33 66 96 15
E-mail: rembu2000@yahoo.com; rembu@pepfardfh.org
Article Type: Research Article;
Accepted: April 26, 2014; Published: April 28, 2014
Citation: Robinson Enow Mbu (2014) Clinical Versus Echographic Estimation of Fetal Weight at Term in A Selected Caucasian Milieu: A Comparative Analysis of The Kongnyuy – Mbu’s Clinical Estimation. Int J Reprod Fertil Sex Health 1(1), 1-6. doi: dx.doi.org/10.19070/2377-1887-140001
Copyright: © 2014 Robinson Enow Mbu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Estimation of fetal weight is essential in contemporary obstetrics. Clinical estimations using maternal and fetal characteristics and ultrasound methods exist. We compared a simple clinical estimation that is in use in low resourced facilities in Cameroon and ultrasound in a completely Caucasian environment.
Methodology: In this cross –sectional study, consented pregnant women with singleton pregnancies were carefully selected and enrolled. Those with adjuvant pathologies that increased uterine volumes were eliminated. We measured fundal heights and applied the Kornyuy – Mbu’s formula for birth weights and compared these with echographic estimations and actual birth weights. We calculated the percentage error between estimated birth weights (EBW) and actual birth weights (ABW) for accuracy and the ratio by percentage of estimation within 10% of actual birth weights.
Results: The average birth weight was 3,529 + 0.35g. We did not have any baby who weighed <2500g, 89.6% weighed between 2,500 - <4000g, and 10.4% had BW > 4,000g. The mean maternal age was 29, 2 + 4 years. The median gravidity and parity were 2 and1 respectively. The mean gestational age at delivery was 40.8 + 0.6 weeks. Clinical method underestimated and echographic method overestimated birth weights slightly but with no significance difference (P=0.130). Clinical method was able to estimate birth-weights within 10% of actual birth weight in all the subjects as against only 50% of the subjects with ultrasound.
Conclusion: Clinical estimation of birth weight as described by Kornyuy and Mbu is as accurate as routine echographic estimation in cases that are well selected.
2.Introduction
3.Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
8.Acknowledgement
9.Competing interest
10.Authors’ contribution
11.References
Keywords
Echography; Clinical Estimation; Fetal Weight; Error; Accuracy
Introduction
Fetal weight estimation is an important consideration when making decisions in obstetrics [1]. Accuracy in estimation remains a challenge to obstetricians especially in breech presentation, previous scar, fetal macrosomia, and previous dystocia [2-4]. Various methods of fetal weight estimation with different conditions and having varying degrees of accuracy and limitations have been reported. Accuracy varies depending on the time, the method and formula used [1]. Clinical estimations based on abdominal palpations and fundal height measurements with errors of 251g, 224g and 310 – 338g have been reported by some authors [5-8], [13].
Although ultrasound has its limitations, only few health facilities in developing countries have ultrasound equipments and when available, not all clients can afford for them. Clinical estimation, however, could be as accurate as routine ultrasound estimation, except in low birth-weight babies [9].
In daily obstetric practice, no standard clinical formula has been adopted in estimating fetal weight in Cameroon and this led to the development and testing of the Kongnyuy – Mbu’s method. This method uses only fundal height (FH) to estimate fetal weight (FW) in grams [Estimated FW = 3(FH)2]. The two authors working in the biggest maternity in Cameroon discovered that the abdominal circumference (AC) of a pregnant Cameroonian woman at term is thrice the fundal height and they derived the formula from the FH x AC used routinely to estimate fetal weights in the service. The authors explained that AC is influenced by the body mass index (BMI) while fundal height is not. The inexpensive and easy availability of the non-elastic tape makes it attractive for use in fetal weight estimation in developing countries [10-12]. This study was carried out to compare this method and routine echography in relation to actual birth weights at term.
Methods
We carried out a cross – sectional study that lasted twelve months (15th June 2011 – 14th June 2012) at the Regional Hospital Centre Chartres, France. This is a referral hospital quoted as level 2B in France and is a centre for the training of French and foreign interns. We received authorization to test and compare this formula with ultrasound estimations of fetal weights from the authors of this formula and ethical clearance from the hospital.
We recruited women with singleton pregnancies who were seen at the out-patient consultation or referred and who were to undergo either abdominal or vaginal deliveries at term (37-42 completed weeks of gestation) and who consented. We excluded those with uterine fibroids, multiple gestations, polyhydramnios, oligohydramnios, fetal anomalies or demise, unsure dates, abnormal lie or presentation, ante partum hemorrhage and eclampsia. We also excluded women whose body mass indices were at least 30.
Women who consented were enrolled and we took measurements from the highest point on the uterine fundus to the midpoint of the upper border of the symphysis pubis with the women in supine position and with voided bladders. We used the inelastic flexible tape for measurements. All measurements were taken thrice to the nearest centimeter by the same person and the mean of these readings was then taken as the absolute measurement. Demographic data were completed in the questionnaire and each woman was thereafter sent for ultrasound estimation of fetal weight by an expert in obstetrical ultrasonography using the highly performant VOLUSON 730 apparatus and applying the Hadlock-3 formula. The ultrasound printout was attached to the study questionnaire of each woman. Clinical estimation applying the Kongnyuy-Mbu’s formula was then made.
Completion of the questionnaire was done at delivery and the actual fetal weight was recorded. The midwives who weighed the new borns were not aware of the fetal weight estimates.
All data were analyzed using the SPSS, the 17.0 version.
Statistical Analysis
Accuracy of birth-weight was determined by calculating the percentage error between the estimated birth weight (EBW) and the actual birth weight (ABW), that is, EBW-ABW ×100/ABW and the ratio by percentage of estimation within 10% of actual birthweight. Each of these error terms was averaged for each method of estimation in the entire study group and in the strata of birth weights. The mean error represented the sum of positive (overestimations) and negative (underestimations) from actual birth weights approximating zero in a method with very low or no systemic error.
The difference between the two methods in the mean percentage error (i.e. the size of systemic error) in each method was assured by the Paired t-test. The mean absolute percentage error was the sum of the absolute deviations (regardless of their direction) reflecting the size of the overall predictive error in terms of actual birth-weight.
Since the absolute errors are not normally distributed, Wilcoxon Signed-rank test (non-parametric) was used for testing the differences between the estimates. The difference in proportion of estimates within 10% of actual birth-weight was assessed by the chisquare test. P<0.05 was considered statistically significant. Each outcome measure was assessed for overall foetal weight and for three categories of weights: <2.500g, 2.500<4000g and ≥4000g. The overall correlation coefficients of ultrasound and the Kongnyuy- Mbu’s estimates were compared.
Results
Ninety six women were recruited. The mean actual birth weight was 3,529 + 0.35 (range: 2,715 – 4,380) g. There were no birth weights <2500g, 89.6% had birth weights between 2,500 - < 4000g, and 10.4% had birth weights >4,000g. The mean maternal age was 29, 2 + 4.8 (range: 16-41) years. The median gravidity and parity were 2 (range: 1 – 8) and 1(range: 0-7). Thirty – three percent (33%) were nulliparous, and 65% were multiparous while 02% were grand multiparous. The mean gestational age was 40.8 + 0.6 (range 39-42) weeks.
Table 1 shows the accuracy and statistical differences between clinical and ultrasonic-estimated fetal weights.
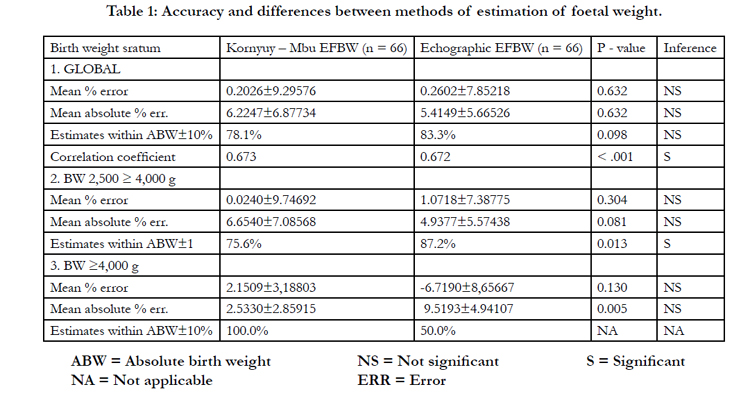

Table 1: Accuracy and differences between methods of estimation of foetal weight.
Figures 1a and 1b show the scatter diagrams of actual birth weights by method of estimation. Figures 2(a/ b) and 3 (a / b) show the overall distribution of the error terms for the two methods.
.JPG)
.JPG)
Figure 1a: Scatter diagram of actual birth-weight with respect to clinical estimation by the Kongnyuy-Mbu’s method.
.JPG)
.JPG)
Figure 1b: Scatter diagram of actual birth-weight with respect to echographic method.
.JPG)
.JPG)
Figure 2a: Overall distribution of percentage error terms by the Kongnyuy-Mbu’s clinical estimation.
Standard deviation = 9.29576; Mean = -0.2026; N=96
.JPG)
.JPG)
Figure 2b: Overall distribution of percentage error by echographic estimation.
Standard deviation = 7.85218; Mean = -0.2602; N=96
.JPG)
.JPG)
Figure 3a: Overall distribution of absolute percentage error terms by the Kongnyuy-Mbu’s clinical.
Standard deviation = 6.87734; Mean = -6.2247; N=96
.JPG)
.JPG)
Figure 3b: Overall distribution of absolute percentage error terms by echographic estimation.
Standard deviation = 5.66526; Mean = -5.4149; N=96
Echographic estimates were within 10% of the actual birth weight in 87.2% of weights between 2500 – 4000 g as against 76.5% for clinical estimation (p = 0.098). The clinical method overerestimated and echographic method underestimated fetal weight. Clinical method estimated all birth weights within 10% of actual birth weights as against 50% for echographic estimations for babies weighing at least 4000g.
Discussion
In this study, the clinical method (Kongnyuy-Mbu’s) generally under estimated while echographic method over estimated birth weights. However the difference between the two methods was not statistically significant (P = 0.632). The mean absolute percentage error was greater (6.22% vs 5.41%) for the clinical estimation,although the difference was not statistically significant (P=0.632) figs. 3a/3b
Estimates within 10% of actual birth weight were better with echography (87.2% vs 75.6%) for foetal weights ranging between 2,500 – 4,000g, but the difference was not statistically significant (P=0.098). The accuracy of clinical estimation obtained was highest in the birth weights range between 2,500-4000g. It was also best when birth weights were >4000g. We did not have any cases in the group with birth weights <2500g. In the high birthweight (>4000g) group, however, the clinical method systematically overestimated birth-weight, while the echographic method underestimated it, but the difference between these methods was not statistically significant (P=0.130). Clinical method was able to estimate birth-weights within 10% of actual birth weights in all (100%) of the subjects with birth weights > 4000g; meanwhile this was possible in only 50% with the echographic method. Bothmethods generally overestimated foetal weight by 300 g and 450 g for echographic and clinical method respectively.
Accurate prediction of fetal weight has been of great interest in obstetrics. Identification of intrauterine growth restriction after 37 weeks’ gestation is an indication for delivery in order to reduce the chances of foetal mortality [23]. Similarly, diagnosis of macrosomiafrequently leads to delivery by means of caesarean section to reduce risk of failed vaginal delivery and shoulder dystocia [16],[17],[23].
As fetal weight cannot be measured directly, it must be estimatedfrom fetal and maternal anatomical characteristics. Many researchers have used different methods to achieve this and the most commonly used are clinical and echographic but a few studies have compared the two methods [9], [14-20], [24,26,28], [30-42].
The correlation coefficient for the clinical and ultrasonic methods, compared to actual birth-weight, were +0.673 and + 0.672 respectively (Table 1), and results of statistical analysis showed these coefficients were statistically significant (P=0.000). These coefficients are comparable with those reported in similar studies(0.67 vs 0.74) [9].
With respect to echographic estimation, our results are in consonance with what has been reported that the mean absolute percentage error of predicted birth weights varies between 6% and 12% of actual birth weights, and 40-75% of the estimates arewithin 10% of actual birth weights [23,27,38]. This was higher(90%) in our study and could be explained by the strength of the echography machine (VOLUSON 730) used and its manipulators. Also, our wide range of exclusion criteria in patient selection could have contributed to this relatively high accuracy with respect to results reported by others.
In previous studies, no standardized method was used for clinical estimation, making it subjective, poorly defined and non-reproducible. Sonographic methods are used because they are objective, reproducible and involve well-defined measurement procedures. In this study, we used a standardized method of clinical estimation that had been found previously to correlate well with birth-weight thus making it a unit protocol [25]. The Hadlock-3 formula present in the ultrasound machine found in the service was used for echographic estimation since authors who have compared the accuracy of conventionally used formulae suggestthat no single formula estimates birth weight more accurately toa significant degree than any other formulae, thus eliminating the bias that only Hadlock-3 formula was used [14].
Two measures of accuracy were used in our statistical analysis in the estimates within + 10% of actual birth weight. They were the mean percentage error, and the mean absolute percentage error. Interestingly, the mean percentage error can be misleading because it is the sum of positive and negative deviations from actual birth weight, thus artificially reducing the difference between actual birth weight and estimated birth weight. It is a measure of systematic error in each method and not variation from birth weight. By contrast, the mean absolute percentage error reflects the variability noted regardless of their direction and as such, is a much more accurate mediator of differences from actual birth weight. Hence, for practical clinical purposes, the variation between predicted birth weight and actual birth weight is best expressed in the forms of mean absolute percentage error [23].
The major strength of this study is that clinical estimation of fetal birth weight using the Kongnyuy-Mbu’s formula is as accurate as the echographic method but while the clinical method slightly under estimated foetal weight, the echographic method over estimated it. These findings are similar to those reported in previous studies that have had similar designs and sample sizes where no statistically significant differences in estimates + 10% of actual birth weights have been found in birth weights that range from 2,500 – 4,000g [9,18,19]. Some other studies reported that echographic estimations are more accurate only when there is low birth-weight. In these reports, both methods both clinical and echographic methods underestimated birth weights by 400g [14,30]. In recent publications, no significant differences have been reported between the two methods even at extremes of birth weights at term and no advantages of echographic estimation over clinical estimation have been found [20,28,29,32].
In this study, we found out that both methods generally overestimated birth weights by 300g and 450g for echographic and clinical estimations respectively. This was marked in (foetuses) of birth weights >2,500 to <4000g. When the Kongnyuy-Mbu’s formula was applied under a purely African setting, they found an overestimation with respect to the actual birth weights of 251g [13].
In their comparism of accuracy of the two methods, some researchers observed no benefit in obtaining a sonographic estimation because its accuracy is not better than that of clinical estimation, except when there is low birth-weight (<2,500g). In such cases, ultrasound yields a better prediction. These authors concluded that estimation of birth weight is associated with a wide range of actual birth weight variations making obstetrics decision based on such predictions to be likely associated with unnecessary interventions [15].
The above findings have important implications for developing countries like ours (Cameroon) where there are limited technologically-advanced ultrasound machines capable of carrying out fetal weight estimations and coupled with the near absence of experienced radiologists or experts in obstetrical ultrasonography.
Conclusion
The Kongnyuy-Mbu’s clinical estimation of birth weight is also good when compared with routine echographic estimation in carefully selected cases irrespective of race. This simple, user friendly and available method is a useful alternative to ultrasonography in birth weight estimation at term when fetus weighs >2500g. Also,in settings where there is no availability or accessibility of ultrasound, especially where some women may present in emergency situations, this simple method can be used in decision making. If the present results are validated by future studies, the method holds a great promise for use in poor resource settings.
Acknowledgement
We acknowledge Mrs Françoise Debray, the Assistant Director in charge of personnel at the Regional Hospital Centre, Chartres, France for authorizing this study and Dr Michel Frech, Dr Camille Barral, Dr Olivier Guilbaud, Dr Seridi Ismah, Dr Dathevy Tete, Ms Sanaz, Mrs Agathe Bourgeoise all at the same hospital for encouragement and moral support. Our sincere gratitude to Dr Tumasang Florence, Pr Nana Philip, Dr Tonye Rebecca and Dr Ako Simon, obstetricians and gynecologists at the central hospital Yaounde for valorizing the Kongnyuy – Mbu’s clinical method in their daily practice. We are indebted to Mr Martin Mbu for statistical input.
Competing interest
The authors declare that they have no competing interest.
Authors’ contribution
Robinson Enow Mbu and Eugene Korinyuy participated in the design and testing of the clinical method and authorized it to be compared elsewhere. Isaac Mboh Eyong and William Ako Takang developed the protocol, designed and tested the questionnaire, carried out clinical measurements and estimated birth weights. Cyril Faraguet heads the obstetrics and gynecology unit at the Rgional Hospital Centre, Chartres, France. He gave openings to the various compartments of the service. Souhaide Antoune and Eric Louis performed echographic measurements. Vincent Liliann and her team measured the actual birth weights. Gilles Body Robert Joseph – Ivo Leke read the final manuscript.
References
- Ebrahimzadeh ZS, Golmakani N, Saadatjoo SA, Jalalian M (2010) Comparison of clinical estimations of fetal weight at the beginning and end of labor. AMJ 3(10): 672-677.
- Studd J (1982) Progress in Obstetrics and Gynaecology. ( 4th edition) Edinburgh, Churchill Livingstone.
- Philpott RH (1982) Obstructed labor. Clin Obstet Gynaecol 9: 625-640.
- Anderson ABM (1981) Second thoughts on stopping labour. In: Studd J (Ed.), Progress in Obstetrics and Gynaecology, Edinburgh, Churchill Livingstone 1:139-148.
- Ghaemmaghami F, Jamal A, Soleimani MR, Mohammadian H (2002) parturient fundal height and birth weight estimation. Arch Iranian Med 5 (2): 80-83.
- Prechapanich J, Thitadilok W (2004) Comparison of Fetal Weight Estimation Using Clinical and Sonographic Methods. J Med Assoc Thai 87: 1-7.
- Bhandary AA, Pinto P J, Shetty A P (2004) Comparative study of various methods of fetal weight estimation at term pregnancy. J Obstet Gynecol Ind 54(4):336-339.
- Numprasert W (2004) A study in Johnson’s: Fundal Height Measurement for Estimation of Birth Weight. AU JT 8(1): 15-20.
- Akinola SS, Oluwafemi K, Ernest O, Orji R (2007) Clinical versus Sonographic Estimation of Foetal Weight in Southwest Nigeria. J Hth Pop Nutri 25(1): 14-23.
- Egwuatu VE, Osefo NJ (1988) Symphysis-fundal height and abdominal circumference measurements: fetal age relationships in Nigerian women. W Afr J Med 7: 77-82.
- Leke RJI, Nasah BT, Martin GE, Amin ME (1982) Correlation between the fundal height abdominal girth and the fetal weight at birth in pregnant women in Cameroon . Trop J Obstet Gynaecol 3: 13-34
- Abramson JH, Gahlinger M (1999) Computer Programme for Epidemiologist (PEPI) (3rd edition), Llanidloes, Brixton Books.
- Kongnyuy EJ, Mbu ER (2006) Estimation of Foetal Weight at term using maternal characteristics: The Kongnyuy-Mbu’s Formula. Eur J Obstet, Gynaecol Reprod Biol (128):231-235.
- Sherman DJ, Arieli S, Tovbin J, Siegek G, Caspi E, et al. ( 1998) A comparison of clinical and ultra-sound estimation of fetal weight. Obstet Gynaecol 91: 212 -7
- Chauhan SP, Hendrix NW, Magann EF, Morrison JC, Jenney SP, et al (1998) Limitations of clinical and sonographic estimates of birth weight: experience with 1034 parturient. Obstet Gynecol 91:72-7.
- Nzeh DA, Oyawoye O, Adetoro OO (2000) Ultrasound estimation of birth weight in late pregnancy among African women. West Africa J Ultrasound 1:9-14.
- Hanretty KP, Neison JP, Fleming EE (1990) Re-evaluation of clinical estimation of fetal weight: a comparison with ultrasound. J Obstet Gynaecol 10: 199-201.
- Hendrix NW, Grady CS, Chauhan SP (2000) Clinical versus sonographic estimates of birth weight in term of parturients , A randomized clinical trail . J Reprod Med 45: 317-22.
- Raman S, Urquhart R, Yusof M (1992) Clinical versus ultrasound estimation of fetal weight. Aust N Z J Obstet Gynaecol 32: 196-9.
- Watson WJ, Soisson AP, Harlass FE (1988) Estimated weight of the term fetus, Accuracy of ultrasound vs clinical examination. J Reprod Med 33: 369-71.
- Diejomaoh FME (1988) Perinatal and maternal mortality, Textbook of obstetrics and gynaecology for medical student v. 2. Logos: University Services Educational Publishers 304-14.
- Airede AI (1995) Birth weight of Nigerian newborn infants –a review. West Afr J Med 14: 116-20.
- Nahum G (2002) Estimation of fetal weight http://www.emedicin.com.
- Mehdizadeh A, Alaghehbandan R, Horsan H (2000) Comparison of clinical versus ultrasound estimation of fetal weight. Am J Perinatol 17: 233-6.
- Wilcox AG, Skjaerven R (1992) birth weight and prenatal morality: the effect of gestational age. Am J Public Health 82: 378-82.
- Chauhan SP, Lutton PM, Bailey KJ, Guerrieri JP, Morrison JC (1992) Intrapartum clinical, sonographic and parous patients estimates of newborn birth weight. Obstete Gynaecol 79: 956-8.
- Ratanasiri T, Jirapomkul S, Sombooporn W, Seejom K, Patumnakul P (2002) Comparison of the accuracy of ultrasonic fetal weight estimation by using the various equations . J Med Assoc Thai 85: 962-7.
- Baum JD, Gussman D, Stone P (2002) Clinical and patient estimation of fetal weight vs ultrasound estimation. J Reprod Med 47: 194-8.
- Nhum GG, Stanislaw H, Huffakar BJ (1999) Accurate prediction of term birth weight from prospectively measurable maternal characteristics. J Reprod Med 44: 705-12.
- Titapant V, Chawanpaiboon S, Mingmitpatanakul K (2001) A comparison of clinical and ultrasound estimation of fetal weight. J Med Assoc Thai 84: 1251-7.
- Shamley KT, London MB (1994) Accuracy and modifying factors for ultrasonographic determination of fetal weight at term. Obstet gynaecol 84: 926-30.
- Shamley KT, London MB (1994) Accuracy and modifying factors for ultrasonographic determination of fetal weight at term. Obstet Gynaecol 84: 926-30.
- Johnstone FD, Prescott RJ, Steel JM, Mao JH, Chambers S, et al (1996) Clinical and ultrasound prediction of macrosomia in diabetic pregnancy. Br J Obstet Gynaecol 103: 747-54.
- Campbells M, Wilkin D (1975) Ultrasonic measurement of foetal abdominal circumference in the estimation fetal weight. Br J Obstet Gynaecol 82: 689-97.
- Combs C.A, Jackle RK, Rosenn B, Pope M, Miodovnik M, et al (1993) Sonographic estimation of fetal weight based on a model of fetal volume. Obstet Gynaecol 82: 365-70.
- Ott WJ, Doyle S, Wittman J (1986) Accurate ultrasonic estimation of fetal weight: Prospective analysis of new ultrasonic formulas. Am J Perinatol 3: 307-10.
- Waesof SL, Wolf P, Coulehan J, Queenan JT (1986) Comparison of fetal weight estimation formulas with and without head measurements. Obstet Gynaecol 67: 569-73.
- Shepard MJ, Richards VA, Berkowitz RL, Warsof SL, Hobbins JC (1982) An evaluation of two equations for predicting fetal weight by ultrasound. Am J Obstet Gynaecol 142: 47-54.
- Deter RL, Hadlock FP (1985) Use of ultrasound in the detection of macrosomia: a review. JClin Ultrasound 13:519.
- Richards M, Hardy R, Kuh D, Wadsworth ME (2001) Birth weight and cognitive function in the British 1946 birth cohort: longitudinal population based study. BMJ 322: 199-203.
- Susuki K, Minei LJ, Schintzer LE (1974) Ultrasonographic measurement of foetal heart volume for estimation of birth weight. Obstet Gynaecol 43: 867-71.
- Poulos PP, Langstadt JR (1953) The volume of the uterus during labour and its correlation with birth weight: L A method for the prediction of birth weight. Am J Obstet Gynaecol 65: 233-44.
- Wickstorm I, Bergstrom R, Bakketaig L (1993) Prediction of birth weight from internal characteristics: symphysio-fundal height and ultrasound biometry. Gynaecol Obstet Invest 35: 27-33.
- Orji EO (2002) Analysis of obstructed labour at Ife State Hospital. Sahel Med J 5: 143-8





