Acute Hemorrhagic Edema of Infancy: A New Observation
H Elmahi*, S Elloudi, H Baybay, S Gallouj, FZ Mernissi
Department of Dermatology, Hospital Center Hassan II, Fez, Morocco.
*Corresponding Author
Halkim Elmahi,
Department of Dermatology, Hospital Center Hassan II, Fez, Morocco.
E-mail: elmahi.hakima@gmail.com
Received: February 09, 2017; Accepted: March 03, 2017; Published: March 04, 2017
Citation: H Elmahi, S Elloudi, H Baybay, S Gallouj, FZ Mernissi (2017) Acute Hemorrhagic Edema of Infancy: A New Observation. Int J Pediat Health Care Adv. 4(2), 29-30. doi: dx.doi.org/10.19070/2572-7354-170009
Copyright: H Elmahi© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Acute Hemorrhagic Edema of Infancy is a is an uncommon benign cutaneous vacuities , It typically affects children between 4 and 24 months of age. It is characterized by large, target-like, and macular to purpuric plaques predominantly affecting the face, ear lobes and extremities. Non-pitting edema of the distal extremities and low-grade fever may also be present. Extracutaneous involvement is very rare. Despite its worrisome presentation, it carries good prognosis. The etiology of AHEI remains unknown. The potential triggers of AHEI include preceding bacterial or viral infections, immunizations, and drugs. The disease often occurs in winter or fall, supporting the link to preceding viral infections. It is a benign and auto-limited disease, with complete resolution within two to three weeks leaving no sequelae in the majority of cases. No recurrences are described. We report a case of a 8 month old girl admitted at our hospital with Acute Hemorrhagic Edema of Infancy.
2.Introduction
3.Case
4.Discussion
5.Conclusion
6.References
Keywords
Acute Hemorrhagic Edema of Infancy; Leucocytoclastic Vasculitis; Cutaenous Lesions.
Introduction
Acute hemorrhagic edema of infancy (AHEI) is a rare benign acute cutaneous vasculitis that occurs in children between 4 and 24 months [1]. The disease is characterized by the acute appearance of skin lesions, edema, and fever, however, it is self-limiting [1, 2]. The cutaneous findings are dramatic, both in appearance and rapidity of onset; histopathology is characterized by leukocytoclas [2]. We report a case of a 8-month old girl referred at our department with AHEI.
Case
An 8-month-old otherwise healthy infant was referred from the pediatric department in view of fever, purpuric rash, and subcutaneous edema of the extremities, appearing 1 day before the visit. Four days before the rash development, the patient had rhinorrhea and mild fever which he was receiving syrup paracetamol. On examination, the child was in good general condition, with normal vital signs, except mild fever. Cutaneous examination showed multiple oval to round ecchymotic patches and plaques over the face, arms, hands, gluteal area, legs and feet varying in size from 0.5 to 5 cm in diameter [Figure 1, 2 and 3]. The oral mucosa showed no alterations. Systemic examination was normal for age. Routine laboratory workup, including urinalysis was within normal reference limits. The cutaneous biopsy was not done and we have defined the diagnosis of AHEI relying only on the clinical course that was strongly suggestive. we treated the baby symptomatically and prescribed topical application of emollient lotion with subsequent follow-up after 7 days. On second followup visit showed complete resolution of skin lesions with mild pigmentary changes.
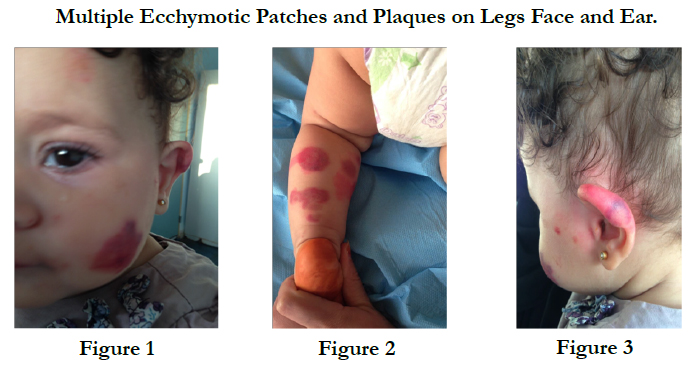

Multiple Ecchymotic Patches and Plaques on Legs Face and Ear.
Discussion
Acute hemorrhagic edema of infancy (AHEI) was originally described by Snow in the USA in 1913 [2]. Finkelstein gave a detailed description in Europe in 1938 and since then it has been recognized in the European literature under various terms: Finkelstein disease [3], Seidlmayer syndrome [1], infantile postinfectious iris-like purpura and edema, purpura en cocarde avec edema. Approximately 122 cases of AHEI have been reported in the literature so far, but the incidence could be underestimated because of the difficulty in recognizing this disease. The etiology of AHEI remains unknown [1, 4]. The potential triggers of AHEI include preceding bacterial or viral infections, immunizations, and drugs. The disease often occurs in winter or fall, supporting the link to preceding viral infections [1]. Males are more susceptible than females [2]. AHEI usually presents in children aged younger than 24 months [5]. The cutaneous lesions are erythematous, annular, rosette, or targetoid patches that cluster and often coalesce. There is a predilection for the face and extremities, but lesions can be found on any cutaneous surface except the mucosal membranes [5]. These self-limiting lesions can appear very suddenly, and many resolve into ecchymotic purpuric patches. The defining characteristic that differentiates AHEI from other entities is the accompanying edema of the hands, feet, face, or extremities [5, 6]. Beside the characteristic skin lesions and a low-grade fever, the patient's history and physical examination are benign, supporting the absence of any visceral involvement. Krause et al., [7] proposed the following criteria for diagnosing AHEI:
• Age b2 years;
• Purpuric or ecchymotic target-like skin lesion with edema on the head and face, with or without mucosal involvement;
• Lack of systemic disease or visceral involvement; and
• Spontaneous recovery within few days or weeks.
The debate over this disease is still open; some authors consider it purely cutaneous variant of Henoch-Schönlein purpura (HSP), whereas some others prefer to regard it as a separate clinical entity within the group of cutaneous small vessel vasculitis of childhood [6]. Both illnesses share a rapid onset of hemorrhagic rashes but in HSP, the face is usually spared and the skin lesions are more polymorphic. Moreover, there is difference in age of onset and in the duration of attacks (which is shorter in AHEI). In contrast to HSP, in AHEI renal, gastrointestinal and joint involvement is uncommon. Other diseases should be considered as differential diagnosis, including purpura fulminans, erythema multiforme, Kawasaki disease, drug eruption, necrotizing fasciitis, batteredchild syndrome, and meningococcal infection [6]. No laboratory findings are specific for AHEI [1, 6].
There is no effective treatment for AHEI and symptomatic care has been advocated (2). Treatment is usually supportive and proper counselling of parents about benign course and good prognosis of the disease is important. Spontaneous recovery usually occurs within 2-3 weeks [8].
Conclusion
To conclude it can be said that AHIE is a disease with apparently alarming symptoms and signs; but its course is benign and outcome is favorable.
References
- Ceci M, Conrieri M, Raffaldi I, Pagliardini V, Urbino AF (2016) Acute Hemorrhagic Edema of Infancy: Still a Challenge for the Pediatrician. Pediatr Emerg Care.
- Roy KP, Madke B, Kar S, Yadav N (2015) Acute Hemorrhagic Edema of Infancy. Indian J Dermatol. 60(6): 624-5.
- Long D, Helm KF (1998) Acute hemorrhagic edema of infancy: Finkelstein's disease. Cutis. 61(5): 283-4.
- Michael DJ (2006) Acute hemorrhagic edema of infancy. Dermatol Online J. 12(5): 10.
- Homme JL, Block JM (2016) Acute hemorrhagic edema of infancy and common mimics. Am J Emerg Med. 34(5): 936.e3-6.
- Serra E Moura Garcia C, Sokolova A, Torre ML, Amaro C (2016) Acute Hemorrhagic Edema of Infancy. Eur Ann Allergy Clin Immunol. 48(1): 22-6.
- Krause I, Lazarov A, Rachmel A, Grunwald MM, Metzker A, et al., (1996) Acute haemorrhagic oedema of infancy, a benign variant of leucocytoclastic vasculitis. Acta Paediatr. 85(1): 114–7.
- Avhad G, Ghuge P, Jerajani H (2014) Acute hemorrhagic edema of infancy. Indian Dermatol Online J. 5(3): 356-7.





