Seborrheic Dermatitis
Alexander K. C. Leung1*, Barankin B2
1 Clinical Professor of Pediatrics, University of Calgary, Pediatric Consultant, Alberta Children's Hospital, Canada.
2 Dermatologist, Medical Director and Founder, Toronto Dermatology Centre, Canada.
*Corresponding Author
Alexander K. C. Leung MBBS, FRCPC, FRCP(UK & Irel), FRCPCH,FAAP,
Clinical Professor of Pediatrics,
University of Calgary, Pediatric Consultant,
Alberta Children's Hospital,
#200, 233 – 16th Avenue NW Calgary,
Alberta, Canada T2M 0H5, Canada.
Fax: (403) 230-3322
E-mail: aleung@ucalgary.ca
Article Type : Review Article
Received: June 01, 2015; Accepted: July 22, 2015; Published: July 24, 2015
Citation: Alexander K. C. Leung, Barankin B (2015) Seborrheic Dermatitis. Int J Pediat Health Care Adv. 2(1), 7-9. doi: dx.doi.org/10.19070/2572-7354-150003
Copyright: Alexander K. C. Leung© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Seborrheic dermatitis is a common chronic inflammatory skin disease characterized by erythema and greasy scales affecting areas rich in sebaceous glands. Seborrheic dermatitis has two incidence peaks, the first in the first three months of life and the second beginning at puberty, reaching its apex at 30 to 40 years of age. Infants with seborrheic dermatitis often present with focal or diffuse scaling and crusting of the scalp. Erythematous or salmon-colored sharply demarcated patches with yellow-white scales may involve the face, postauricular areas, trunk, and intertriginous and flexural areas of the body. In the diaper area, infantile seborrheic dermatitis presents as a sharply demarcated, erythematous, scaly eruption with a tendency to coalesce, resulting in the formation of a large confluent lesion. Pruritus is characteristically absent. In adolescence and beyond, seborrheic dermatitis usually presents as greasy scaling of the scalp. It may also present as ill-defined erythematous patches with yellow-white, greasy scales affecting the nasolabial folds, eyelids, eyebrows, glabella, postauricular area, anterior chest, and less commonly the upper back. Mild periodic pruritus is common in adolescent seborrheic dermatitis. Scalp lesions in infantile seborrheic dermatitis usually respond to simple daily shampooing alone or in combination with non-prescription mild shampoos specific for seborrheic dermatitis. For infantile scalp seborrheic dermatitis that does not respond to the above measures, for seborrheic dermatitis lesions elsewhere, and for adolescent or adult seborrheic dermatitis, the use of topical antifungals, calcineurin inhibitors, and low to mid potency corticosteroids should be considered. A compounded mixture of these ingredients is also often employed.
2.Introduction
3.Epidemiology
4.Etiology
5.Histopathology
6.Clinical Manifestations
7.Diagnosis
8.Differential Diagnosis
9.Complications
10.Prognosis
11.Management
12.References
Keywords
Erythema; Greasy Scales; Cradle Cap; Diaper Rash; Topical Antifungals.
Introduction
Seborrheic dermatitis is a common chronic inflammatory skin disease characterized by erythema and greasy scales [1]. The condition typically affects areas rich in sebaceous glands such as the scalp, eyebrows, glabella, nasolabial folds, postauricular area, and intertriginous areas [2, 3]. In general, scaling tends to predominate on the scalp whereas erythema tends to predominate in the flexural folds and intertriginous areas [4].
Epidemiology
Seborrheic dermatitis has two incidence peaks, the first in the first three months of life and the second beginning at puberty, reaching its apex at 30 to 40 years of age [5-7]. The condition affects up to 70% of infants in the first 3 months of life [3, 5] and 3 to 5% of young adults [7-9]. Seborrheic dermatitis is more common in males than females, presumably because androgens stimulate sebum production [6, 8].
Etiology
Seborrheic dermatitis might result from excessive sebaceous gland activity with sebum overproduction as the dermatitis usually develop in areas with the highest density of these glands [1]. The high prevalence of infantile seborrheic dermatitis in early infancy can be explained by a transient surge of gonadotropins with a resulting rise in testosterone levels which peaks at 1 to 3 months of age. It is believed that the sebum permits growth and proliferation of commensal yeasts of the Malassezia (formerly known as Pityrosporum) family which, through the action of lipases, degrade lipids on the skin surface with production of unsaturated and saturated fatty acids [7, 9]. The inflammation which causes hyperproliferation of stratum corneum (scaling) results from nonimmunogenic irritation due to unsaturated fatty acids and the cellular immune response to these yeasts [2, 7, 9]. There is a genetic predisposition; there is an increase in the frequency of HLA-A32, HLA-AW30, HLA-AW31, HLA-B12, and HLA-B18 in patients with seborrheic dermatitis [7, 9].
In adolescence and beyond, predisposing factors include HIV infection, stress, medications (haloperidol, chlorpromazine, buspirone, lithium), trisomy 21, and familial amyloidosis with polyneuropathy [3, 5, 6].
Histopathology
Histological findings in the acute stage include spongiosis, focal parakeratosis, plugged follicular ostia, and superficial perivascular and interstitial lymphocytic infiltration [2, 7]. In the chronic stage, changes include in addition to the aforementioned findings, irregular acanthosis, a poorly formed or absent granular layer, and psoriasiform hyperplasia with dilatation of the capillaries and venules of the superficial plexus [7].
Clinical Manifestations
Infantile seborrheic dermatitis usually develops within the first month of life [10]. Infants with seborrheic dermatitis often present with focal or diffuse, white or yellow, greasy scaling and crusting of the scalp (Figure 1) [1, 2]. The lesion may become so thickened that it forms a cap, meriting its description as cradle cap [1]. Cradle cap is usually the initial and at times the only manifestation of infantile seborrheic dermatitis [10]. Not uncommonly, erythematous or salmon-colored sharply demarcated patches with yellow-white scales may involve the face, external ear, postauricular folds, trunk, and intertriginous and flexural areas of the body [1]. In the diaper area, infantile seborrheic dermatitis presents as a sharply demarcated, erythematous, greasy, scaly eruption with a tendency to coalesce, resulting in the formation of a large confluent lesion; it may be mistaken for candidal dermatitis [1]. In infantile seborrheic dermatitis, oozing, weeping and pruritus are characteristically absent [11].
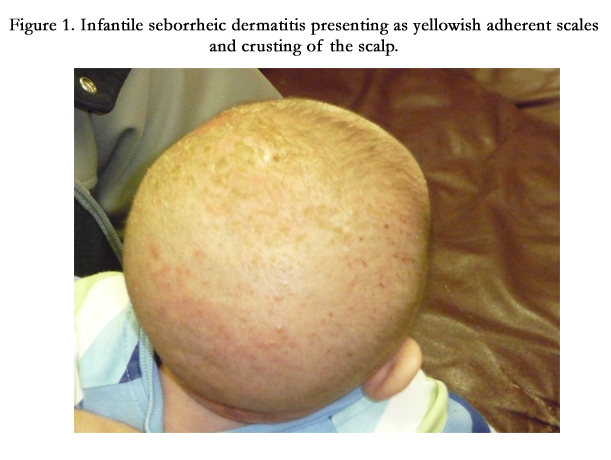

Figure 1. Infantile seborrheic dermatitis presenting as yellowish adherent scales and crusting of the scalp.
In adolescence and beyond, seborrheic dermatitis usually presents as greasy scaling of the scalp (dandruff). It may also present as ill-defined erythematous patches with yellow-white, greasy scales on the nasolabial folds, eyelids, eyebrows, glabella (Figure 2), postauricular area, anterior chest, and less commonly the upper back [11, 12]. In contrast to infantile seborrheic dermatitis, pruritus is common in adolescent seborrheic dermatitis, especially with scalp involvement [6]. Involvement of the eyelids may lead to blepharitis with erythematous eyelids and potential destruction of eyelid follicles [7, 8]. The upper chest and back are less commonly affected [12]. Generalized seborrheic dermatitis is uncommon which, if present, should lead to the suspicion of an underlying immunodeficiency disorder.
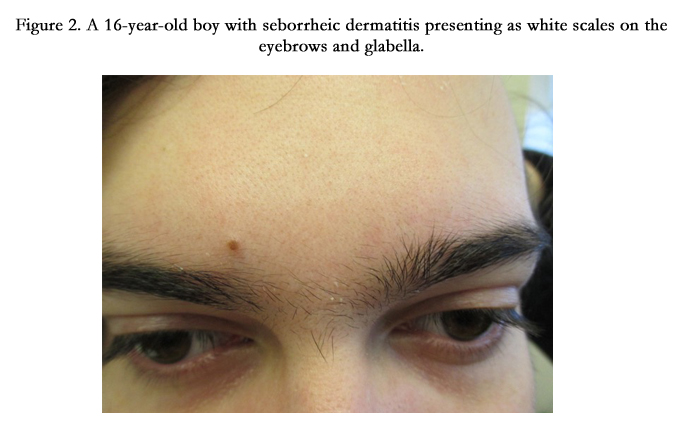

Figure 2. A 16-year-old boy with seborrheic dermatitis presenting as white scales on the eyebrows and glabella.
Diagnosis
The diagnosis is mainly clinical, based on the characteristic clinical morphology of scaling and erythema in typical sebum-rich areas. If necessary, the diagnosis can be aided by dermoscopy which shows atypical red vessels, arborizing vessels, and structureless red areas [13]. If tinea capitis is suspected, a potassium hydroxide wet-mount examination of scalp scrapings may help in the diagnosis. Referral to a dermatologist should be considered if the diagnosis is in doubt.
Differential Diagnosis
Seborrheic dermatitis should be differentiated from atopic dermatitis, irritant diaper dermatitis, tinea capitis, psoriasis, rosacea, Langerhans cell histiocytosis X, and immunodeficiency [11]. Infantile seborrheic dermatitis is distinguished from atopic dermatitis by its earlier age of onset, involvement of the scalp, diaper area, and flexural rather than extensor surfaces, well-defined lesions with dry fine scaling, absence of oozing or weeping, and absence of pruritus [10].
Typically, irritant contact dermatitis presents as confluent erythema and maceration on the convex skin surfaces in contact with the diaper. The skin has a shiny, glazed appearance. In contrast to infantile seborrheic dermatitis, the intertriginous folds are usually spared.
Tinea capitis typically presents as fine scaling with patches of circular alopecia; diffuse or patchy, fine, white, adherent scaling of the scalp resembling generalized dandruff; or patches of well-demarcated areas of alopecia with fine scales, studded with brokenoff, swollen hair stubs, resulting in a “black dot” appearance.
In infants and young children, psoriasis often present as sharply demarcated erythematous plaques in the diaper and intertriginous areas. The classic silvery scales are usually absent. Compared to infantile seborrheic dermatitis, the response to topical corticosteroid is much slower, and there is no response to topical antifungals.
Rosacea is characterized by telangiectasia, persistent erythema of the central face, small, dome-shaped erythematous papules, and/ or tiny pustules on the central aspects of the face. The perioral and periocular areas are typically spared. Facial flushing, dryness, scaling, edema, or burning/stinging (“sensitive skin”) sensation may be present.
Langerhans cell histiocytosis X is a multisystem disease that can be distinguished by the presence of 1 to 3 mm discrete yellowish to red-brown crusted papules, purpuric lesions, lymphadenopathy, and hepatosplenomegaly. The cutaneous lesions are resistant to topical corticosteroid [10].
Various immunodeficiency states may present with an intractable seborrhea-like dermatitis. Immunodeficiency should be suspected if there are constitutional findings such as fever, anemia, diarrhea, and failure to thrive.
Complications
Although scalp hair loss is not usually associated with seborrheic dermatitis, alopecia may result if the scalp involvement is chronic and severe [14]. Infantile seborrheic dermatitis may be complicated by superimposed infection with Candida species. Postinflammatory pigmentary changes may occur, particularly in more pigmented individuals [1]. Blepharoconjunctivitis may also occur [3]. In adolescence, the condition can be socially embarrassing and may have a substantial adverse effect on the quality of life [3, 8].
Prognosis
Infantile seborrheic dermatitis is usually self-limiting, resolving within several weeks to several months [11]. The majority of cases clear by 12 months of age [11, 12]. In adolescent and adult seborrheic dermatitis, the disease runs a chronic course with relapses and remissions [12].
Management
Treatment should be individualized, taking into consideration the age of the patient, location of the lesion, response to previous treatment, preference of the patient, and adverse effect of the medication. Scalp lesions in infantile seborrheic dermatitis usually respond to more regular shampooing alone or in combination with the non-prescription mild shampoos specifically labelled for seborrheic dermatitis. For infantile scalp seborrheic dermatitis that does not respond to the above measures, for seborrheic dermatitis lesions elsewhere, and for adolescent or adult seborrheic dermatitis, the use of topical antifungals (ketoconazole, ciclopirox), calcineurin inhibitors (tacrolimus and pimecrolimus), and low to mid potency corticosteroids should be considered, alone or in combination [2, 15-19]. Topical antifungal agents (ketoconazole, ciclopirox, sertaconazole) which are available in different formulations such as creams and shampoos are the mainstay of treatment [2, 5, 6]. Shampoos with different active ingredients (e.g. zinc pyrithione, ketoconazole, selenium sulphide, tar, salicylic acid) have been used with success [20, 21]. In this regard, zinc pyrithione-based shampoos are effective, affordable, and have excellent cosmetic and hair conditioning effects; all of which will encourage long-term compliance. More frequent shampooing is often helpful [21].
Oral antifungals (itraconazole, ketoconazole, terbinafine, fluconazole) or isotretinoin are rarely indicated but may be considered in selected cases of extensive and severe lesions resistant to topical treatment [8, 22].
References
- Leung AK (2011) Infantile seborrheic dermatitis. In Common Problems in Ambulatory Pediatrics: Specific Clinical Problems. Nova Science Publishers, Inc., New York. 2: 291-295.
- Clark GW, Pope SM, Jaboori KA (2015) Diagnosis and treatment of seborrheic dermatitis. Am Fam Physician 91(3): 185-190.
- Naldi L, Rebora A (2009) Clinical practice. Seborrheic dermatitis. N Engl J Med 360(4): 387-396.
- O’Connor NR, McLaughlin MR, Ham P (2008) Newborn skin: Part 1. Common rashes. Am Fam Physician 77(1): 47-52.
- Berk T, Scheinfeld N (2010) Seborrheic dermatitis. Pharmacy and Therapeutics 35(6): 348-352.
- Mokos ZB, Kralj M, Juzbacic AB, Jukic IL (2012) Seborrheic dermatitis: an update. Acta Dermatovenerol Croat 20(2): 98-104.
- Sampaio AL, Vargas TJ, Nunes AP, Mameri AC, Silva MR, et al. (2011) Seborrheic dermatitis. An Bras Dermatol 86(6): 1061-1074.
- Dessinioti C, Katsambas A (2013) Seborrheic dermatitis: etiology, risk factors, and treatments: facts and controversies. Clin Dermatol 31(4): 343-351.
- Ramos-e-Silva M, Sampaio AL, Carneiro S (2014) Red face revisited: endogenous dermatitis in the form of atopic dermatitis and seborrheic dermatitis. Clin Dermatol 32(1): 109-115.
- Elish D, Silverberg NB (2006) Infantile seborrheic dermatitis. Cutis 77(5): 297-300.
- Schwartz RA, Janusz CA, Janniger CK (2006) Seborrheic dermatitis: an overview. Am Fam Physician 74(1): 125-130.
- Poindexter GB, Burkhart CN, Morrell DS (2009) Therapies for pediatric seborrheic dermatitis. Pediatr Ann 38(6): 333-338.
- Kibar M, Aktan S, Bilgin M (2015) Dermoscopic findings in scalp psoriasis and seborrheic dermatitis; two new signs; signet ring vessel and hidden hair. Indian J Dermatol 60(1): 41-45.
- Pitney L, Weedon D, Pitney M (2015) Is seborrheic dermatitis associated with a diffuse low-grade folliculitis and progressive cicatricial alopecia? Australas J Dermatol doi: 10.1111/ajd.12289.
- Okokon EO, Verbeek JH, Ruotsalainen JH, Ojo OA, Bakhoya VN (2015) Topical antifungals for seborrheic dermatitis. Cochrane Database Syst Rev (4): 1-229.
- Draelos ZD, Feldman SR, Butners V, Alió Saenz AB (2013) Long-term safety of ketoconazole foam, 2% in the treatment of seborrheic dermatitis: results of a phase IV, open-label study. J Drug Dermatol 12(1): e1-e6.
- Goldust M, Rezaee E, Raghifar R, Hemayat S (2013) Treatment of seborrheic dermatitis: the efficiency of sertaconazole 2% cream vs tacrolimus 0.03% cream. Ann Parasitol 59(2): 73-77.
- Lebwohl M, Plott T (2004) Safety and efficacy of ciclopirox 1% shampoo for the treatment of seborrheic dermatitis of the scalp in the US population: results of a double-blind, vehicle-controlled trial. Int J Dermatol 43(Suppl 1): 17-20.
- Shuster S, Meynadier J, Kerl H, Nolting S (2005) Treatment and prophylaxis of seborrheic dermatitis of the scalp with antipityrosporal 1% ciclopirox shampoo. Arch Dermatol 141(1): 47-52.
- Schmidt-Rose T, Braren S, Folster H, Hillemann T, Oltrogge B, et al. (2011) Efficacy of a piroctone olamine/climbazol shampoo in comparison with a zinc pyrithione shampoo in subjects with moderate to severe dandruff. Int J Cosmet Sci 33(3): 276-282.
- Schwartz JR, Bacon RA, Shah R, Mizoguchi H, Tosti A (2013) Therapeutic efficacy of ant-dandruff shampoos: a randomized clinical trial comparing products based on potentiated zinc pyrithione and zinc pyrithione/climbazole. Int J Cosmet Sci 35(4): 381-387.
- Gupta AK, Richardson M, Paquet M (2014) Systemic review of oral treatments of seborrheic dermatitis. J Eur Acad Dermatol Venereol 28(1): 16-26.





