Neonatal Alloimmune Thrombocytopenia
Roganović J1*, Kranjcec I2
1 Department of Pediatrics, Division of Hematology and Oncology, University Hospital Centre Rijeka, Croatia.
2 Division of Hematology and Oncology, Children's Hospital Zagreb, Zagreb, Croatia.
*Corresponding Author
Jelena Roganović MD,
Professor of Pediatrics, Pediatric Hematologist and Oncologist,
Department of Pediatrics, Division of Hematology and Oncology,
University Hospital Centre Rijeka, Rijeka, 51000, Croatia.
Tel: +385 51 659 109
Fax: +38551 623126
E-mail: jelena.roganovic1@ri.t-com.hr
Article Type: Case Report
Received: May 15, 2015; Accepted: July 06, 2015; Published: July 08, 2015
Citation: Roganović J, Kranjcec I (2015) Neonatal Alloimmune Thrombocytopenia. Int J Pediat Health Care Adv. 2(1), 4-6. doi: dx.doi.org/10.19070/2572-7354-150002
Copyright: Roganović J© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Neonatal alloimmune thrombocytopenia is the most common cause of immune-mediated thrombocytopenia in the newborn period. The disorder results from placental transfer of maternal alloantibodies directed against paternally inherited antigens carried on fetal platelets. While most cases are mild, some neonates have very low platelet counts associated with serious bleeding in hours to days following birth. The treatment for severely affected neonate is typically transfusion of compatible random donor platelets in addition to intravenous immunoglobulins. The diagnosis is confirmed by genotyping of parental platelet antigens and serological testing for maternal serum antibodies.
We present a newborn with early onset symptomatic thrombocytopenia, in whom early clinical recognition and prompt therapeutic intervention resulted in the complete recovery. The importance of correct diagnosis for future pregnancies is emphasized.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Thrombocytopenia; Newborns; Thrombocytopenia; Neonatal Alloimmune; Antigens; Human Platelet.
Introduction
Neonatal alloimmune thrombocytopenia (NAIT), also referred to as fetomaternal alloimmune thrombocytopenia, is a disorder resulting from placental transfer of maternal alloantibodies directed against paternally inherited antigens present on fetal platelets, but lacking on maternal platelets. The estimated incidence is 1 to 2,000 to 3,000 live births [1]. The most frequently implicated alloantigen in white populations is human platelet antigen (HPA)-1a. Physical findings of the newborn usually reveal skin and mucous membrane bleeding while laboratory evaluation demonstrates isolated thrombocytopenia. The diagnosis is generally based on clinical presentation. The purpose of further testing is to confirm a diagnosis in a suspected case and to guide the management of future pregnancies in affected couple and mothers’ family members [2,3]. Infants born with profound thrombocytopenia and significant bleeding require rapid pharmacological and/or transfusion intervention because of the risk of severe hemorrhage and potentially significant morbidity.
Case Report
A full-term baby boy was delivered by cesarean section at week 38 of gestation due to anticipated fetal distress. He was the third child from the third, uncomplicated pregnancy of a healthy 32-year-old woman. Apart from meconium stained amniotic fluid, delivery was unremarkable. Birth weight, length and head circumference were according to the gestational age (2910 g, 48.5 cm, and 32 cm respectively). A few hours after the delivery a low platelet count was noted (Plt 40x109/μL ), while red and white blood cell counts were within normal limits (Hb 201 g/L, L 29.5x109/L). Chest Xray was normal. Echocardiogram demonstrated patent foramen ovale.
Head ultrasound showed no signs of intracranial hemorrhage. Because of a risk of perinatal infection due to meconium stained amniotic fluid, empirical antibiotic therapy with ampicillin and gentamicin was initiated. A complete blood count of the mother was normal (Plt 376x109/μL). Fifteen hours after birth, the infant presented petechial rash and was transferred to our clinic. Petechiae and bruising on the trunk and extremities were seen, and lower platelet count verified (Plt 31x109/μL).
Examination of the peripheral smear showed sparse large platelets. The patient and both parents had blood type A and Rh factor positive. TORCH screening and blood cultures were negative. Head and heart ultrasound scans were repeated, confirming the former findings. Fundus examination excluded retinal hemorrhages, and fecal occult blood test ruled out gastrointestinal bleeding.
NAIT was suspected, and intravenous immunoglobulin (1/kg/day) for two consecutive days was administered. In the following days, a continuous rise in platelet counts was observed (Figure 1).
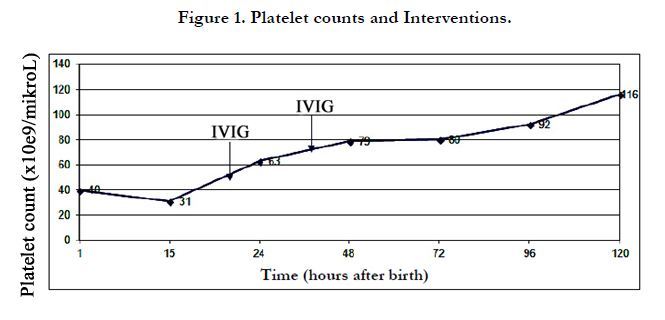
Figure 1. Platelet counts and Interventions.
The baby was discharged from the hospital on the 12th day of life with platelet count 162x109/μL. At the age of 15 days, investigation of anti-platelet antibodies was conducted (Table 1). The father refused testing. Circulating maternal anti-HPA-1a/2a and anti-HPA-2b/3a antibodies were detected, not present in the infant. HPA genotyping was not available at that time. The infant was followed-up for 6 months, and platelet counts remained within normal limits (Plt > 150x109/μL).
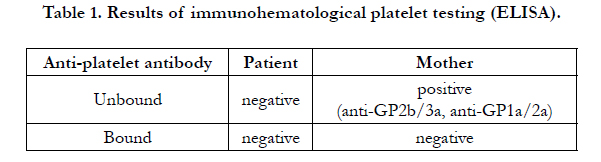

Table 1. Results of immunohematological platelet testing (ELISA).
Discussion
Thrombocytopenia is a common clinical problem in the settings of neonatal intensive care units, developing in up to 35% of all newborns admitted [4]. Early onset thrombocytopenia (<72 hours of age) is mostly due to immune mechanisms, congenital infections and asphyxia, while commonest causes of late onset thrombocytopenia (>72 hours of age) are bacterial sepsis, necrotizing enterocolitis, or both [5]. The most common cause of immune-mediated thrombocytopenia in the newborn period is NAIT, when mother develops alloantibodies against the paternal antigen present on the fetal platelets that the mother lacks. In contrast to Rh(D) hemolytic disease, NAIT may occur during the first pregnancy in half of the cases. The most frequent cause in Caucasians are antibodies to human platelet antigen (HPA)-1a.
The severity of NAIT is related to the following factors: pregnancy order (second being more severely affected than first), outcome of previous pregnancies (prenatal intracranial hemorrhage in previous child increasing the likelihood of hemorrhage in future children), platelet antigen (HPA-1a alloimmunization being more severe), and HLA type (HLA DRB3 0101 being highly predictive of alloimmunization). Common hemorrhagic manifestations include petechiae, bruising and gastrointestinal bleeding, and most affected newborns otherwise look well. The degree of thrombocytopenia may be severe, and patients with NAIT are at increased risk for intracranial hemorrhage, appearing in 10% to 20% of cases. The diagnosis is confirmed by serologic testing. Antigen testing of the mothers’ and fathers’ platelets should be performed, mothers’ serum tested for antiplatelet antibody, and parental platelet antigen genotypes identified if available. However, NAIT is primary a clinical diagnosis, and therapy should be initiated in severe cases as soon as the diagnosis is suspected. Term, healthy infants with no risk factors or with signs of bleeding are transfused if the platelet count is below 30x109/μL. The threshold for transfusion is higher in preterm infants or ill, term infants with risk factors. The treatment of choice for severe NAIT is transfusion of washed, irradiated maternal platelets. Due to medical or practical reasons it is often difficult to implement, and random-donor platelet infusions are mostly applied. Adequate platelet count should be maintained during the first 72 to 96 hours. As a temporary measure of limited benefit, intravenous immunoglobulin (400 mg/kg/day for 3 to 4 days, or 1 g/kg/day for 1 to 3 days) may be administered. Intravenous glucocorticoid (methylprednisolone 1 mg/kg/3 times a day for 1 to 3 days) has been used as an adjunctive therapy. Thrombocytopenia resolves over the first few months of life, and close monitoring of patient and platelet count during this period is strongly recommended.
Since the intracranial hemorrhage is responsible for most of neonatal mortality and significant morbidity, efforts are made to reduce NAIT incidence to a minimum by prenatal maternal management. The detailed counseling should be provided to the family at the time of the first diagnosis, and formal serologic and genotyping testing initiated in the early postpartum period. Standard-risk pregnancies are those with a history of previous child with thrombocytopenia but no intracranial hemorrhage. At 20 weeks of gestation IVIG is initiated (2 g/kg/week), supported by glucocorticoid (prednisone 0.5 mg/kg/day) at 32 weeks, no amniocentesis performed, and pregnancy terminated at 38 to 39 weeks by cesarean section. Pregnancies with a history of previous child with intracranial hemorrhage in the third semester or neonatal period are considered as high-risk. For them IVIG (1 g/kg/ week) is initiated at 12 weeks of gestation, the dose increased at 20 weeks (2 g/kg/week) or glucocorticoid added (prednisone 0.5 mg/kg/day), both continued in mentioned doses from 28 weeks, no amniocenteses performed, and pregnancy terminated at 37 to 38 weeks by cesarean section. Fetal intracranial hemorrhage in the second trimester places the patient in the extremely high-risk group. In these cases IVIG (2 g/kg/week) is introduced at 12 weeks of gestation, glucocorticoid (prednisone 1 mg/kg/day) added at 20 weeks, no amniocentesis performed, and cesarean delivery carried out at 36 to 37 weeks.
Hereby we report a newborn with severe early-onset thrombocytopenia and skin hemorrhage. The mothers’ platelet count was normal. Previous two pregnancies and births were uneventful. The diagnosis of NAIT was based on clinical information. IVIG was an effective treatment, and no antigen-compatible platelet transfusion was needed. Circulating maternal antiplatelet antibodies favored the diagnosis of NAIT.
Conclusion
Severe thrombocytopenia is a potentially lifethreatening condition. Initial management of newborns with active bleeding takes advantage over any diagnostic evaluation. Parental and neonatal testing should be obtained if available, to determine future fetus’ risk of developing NAIT.
References
- Manno CS (2005) Management of bleeding disorders in children. Hematology Am Soc Hematol Educ Program 2005(1):416-422.
- Nugent DJ (2006) Immune thrombocytopenic purpura of childhood. Hematology Am Soc Hematol Educ Program 2006(1):97-103.
- Roberts I, Murray NA (2003) Neonatal thrombocytopenia: causes and management. Arch Dis Child Fetal Neonatal Ed 88(5):F359-F364.
- Sola-Visner M, Sallmon H, Brown R (2009) New insights into mechanisms of non-immune trombocytopenia in neonates. Semin Perinatol 33(1):43-51.
- Roberts IA, Murray NA (2006) Neonatal thrombocytopenia. Curr Hematol Rep 5(1):55-63.





