Effect of Fentanyl Addition to Local Anesthetic on Peribulbar Block in Keratoplasty Sugery
Bakry MA1, Khalil NM2*, M El H Abdel Ghaffar3
1 Department of Anesthesia, affiliated to SICU and Pain Management, Kasr Al-ainy School of medicine, Cairo University, Egypt.
2 Department of ophthalmology, affiliated to Kasr Al-ainy School of medicine, Cairo University, Egypt.
3 Department of Anesthesia, affiliated to the Research Institute of Ophthalmology, Cairo University, Egypt.
*Corresponding Author
Khalil NM (M.D),
Department of Ophthalmology, Affiliated to Kasr Al-ainy School of medicine,
Cairo University, Egypt.
Tel: +20238384023
E-mail: khalilnoha76@gmail.com
Received: March 31, 2016; Accepted: April 28, 2016; Published: April 30, 2016
Citation: Bakry MA, Khalil NM, M El H Abdel Ghaffar (2016) Effect of Fentanyl Addition to Local Anesthetic on Peribulbar Block in Keratoplasty Sugery. Int J Opthalmol Eye Res,S7:001, 1-5. doi: dx.doi.org/10.19070/2332-290X-SI07001
Copyright: Khalil NM© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Peribulbar block is becoming increasingly popular in ophthalmic practice because it is simple and safer. In this study , the addition of fentanyl to peribulbar anesthesia as regard the duration and intensity of ophthalmic block is evaluated and thus the possibility of performing lengthy surgeries without the need for top-up doses.
Methods: 200 patients undergoing penetrating keratoplasty were randomly classified into Group F which received 12cc peri bulbar block containing 30ug Fentanyl and 0.5% bupivacaine and 75 units Hyalase and group C which received 12cc peribulbar block containing 0.5% bupivacaine and 75 units Hyalase.
Results: Duration of block and surgeon satisfaction were significantly higher in group F compared to group C. There was no difference between the two groups regarding onset of anesthesia or lid akinesia.
Conclusions: Addition of fentanyl to peribulbar block potentiates the intensity of the block and increases its duration.
2.Introduction
3.Methods
3.1.Exclusion criteria
3.2.Data recorded
3.3.Statistical Analysis
4.Results
4.1.Globe Akinesia
4.2.Lid Akinesia
4.3.Perioperative Complications
4.4.Surgeon’s Satisfaction
5.Discussion
6.References
Keywords
Fentanyl; Peribulbar Block; Keratoplasty; 0.5% Bupivacaine; Hyalase.
Introduction
Peribulbar anesthesia is now accepted as a safe locoregional anesthesia to carry out most of the ophthalmic procedures. However, in penetrating keratoplasty (PKP) it carries many risks if the patient becomes restless since PKP is an “open sky” procedure making it totally dependent on the changes in the intra-ocular pressure (IOP). [1] Therefore, the main concern of anesthesia is to limit the risks associated with unexpected increase of IOP , the most hazardous of which would be suprachoroidal hemorrhage. [2]. Advancements in keratoplasty techniques are thus being made constantly to further improve prognosis and minimize the risks. Some of these include deep lamellar techniques and femtosecond laser assisted keratoplasty , the latter of which requires the patient to be transferred from one room, where the recipient’s and donor’s cornea are being cut by the femtosecond laser, to the operating room for graft suturing. Unfortunately, these advancements came at a cost as the procedure became lengthier.
With advancement in keratoplasty surgeries and introduction of femtosecond laser assisted keratoplasty, the use of local ophthalmic block became more and more the standard technique, as it omits the risks of transporting the patient between rooms under general anesthesia (in case of femto keratoplasty) and also avoids postoperative vomiting which may be hazardous to the graft due to increased intra ocular pressure. Therefore, the prolongation of the duration of peribulbar block has long been the ultimate target for both the anesthesiologist and the ophthalmologist. Addition of adjuvant drugs to the local anesthetic mixture might provide a simple way to prolong the duration of the block in case the surgical technique lasted more than the expected time [3].
Opioids have been added to local anesthetics and injected extradurally, intrathecally or in nerve plexuses for a more intense and prolonged analgesia by acting on opioid receptors present on the nerve terminals [4-7]. Fentanyl (N-phenyl-N-(1-Phenethyl-4-piperi-dinyl) propanamide) is an opioid analgesic with potency eighty times that of morphine. However, fentanyl has some side effects as vomiting, pruritus and respiratory depression. To our knowledge, few studies discussed the effect of adding fentanyl to peribulbar block in ophthalmic practice [8, 9] and this is the first study to investigate its addition to the peribulabar block in keratoplasty.
The aim of the current study was to investigate whether the addition of fentanyl to peribulbar anesthesia prolongs the duration of the block in lengthy keratoplasty operations without the need for top-up doses which might carry many risks jebradizing the results of surgery.
Methods
Two hundred adult patients of ASA physical status I and II, of both sexes and scheduled for elective keratoplasty surgery in Alrowad eye hospital ( a private hospital affiliated to cairo university), were consecutively recruited between August 2012 to November 2015. Informed written consent was obtained from all the patients who participated in the study. Data collection conformed to all local laws and was compliant with the principles of the Declaration of Helsinki.
Each patient underwent a full ophthalmological examination by an ophthalmologist and A-scan ultrasonography was performed using the E-Z Scan™ AB5500+ device (SONOMED INC., USA). to measure the axial length and to do biometry if it was needed.
(1) any associated disorders, (2) refusal of local anesthesia, (3) single eyed patients , (4) high myopes (axial length >28 mm), (5) glaucoma , (6) impaired orbital sensation, (7) coagulopathy, (8) impaired consciousness, (9) mental retardation, (10) recent myocardial infarction and (11)uncontrolled hypertension.
Preoperative investigations in the form of electrocardiograpgy (ECG) , chest X-ray, complete blood picture, coagulation profile, liver function tests and kidney function tests were carried out. Patients were randomly divided into two groups: Group F received 12cc peribulbar block containing 30ug Fentanyl and 0.5% bupivacaine and 75units Hyalase. Group C received 12cc peribulbar block containing 0.5% bupivacaine and 75units Hyalase.
In all patients an intravenous (IV) line was inserted, basic monitors were applied (ECG, pulse oximeter, NIBP). Patients received Metoclopramide 10mg and 2mg dormicum I.V. as premedications. Peribulbar block was performed in the operating room while patients were in supine position. After sterilization, a 12 cc solution was injected into the following sites: medial canthus and inferotemporal peribulbar areas. Injection was done by the use of a 22-gauge short bevel needle. Ocular compression was performed by the application of Honan intraocular pressure reducer to aid in the diffusion of anesthetic mixture to achieve extraocular muscle paralysis and lid akinesia and also to reduce intra ocular pressure prior to surgery.
age, sex
measured at 3,5 and 10 mins after the administration of the block,
• Globe Akinesia was recorded using Globe Akinesia score (Ozdemir et al, 2004):
The time between onset and full effect,
Full movement 3
Moderate movement 2
Flicker 1
No movement 0
• Lid Akinesia was recorded using Lid Akinesia Score (Ozdemir et al, 2004):
The time between onset and full effect,
Full movement 2
Flicker 1
No movement 0
Duration till full recovery and duration of analgesia; indicted by full return of ocular movement and discomfort sensation.
Surgeon satisfaction was evaluated by the requirement of top up doses given intra-operatively due to regaining of kinesia or due to patient discomfort.
Occurrence of complictions eg. Bleeding, nausea, and vomiting.
The data is expressed as mean (±), standard deviation (SD), median (range), or actual number (%) as appropriate. Continuous data (e.g. age) were compared using the unpaired Student's t-test. Categorical data were compared using the Χ² test. ANOVA test was used to detect significant differences between the different groups. Tukey- Kramer multiple comparison test was used. If the value of Q was greater than 3.688 then p value was <0.05. In case of perioperative complications, Kruskial-Wallies (non parametric test for abnormally distributed data) was used. For all tests, a p value < 0.05 was considered significant.
Statistical calculations were performed using MedCalc software for windows, version 10.0.2.0, (Frank schoonjans).
Results
There was no statistically significant difference between the two studied groups as regard the age and the sex. There was also no statistically significant difference between the groups regarding duration of surgery as shown in the following Table1.
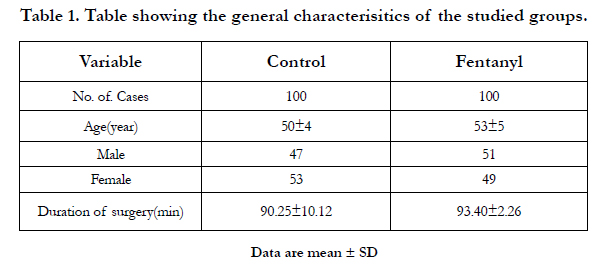

Table 1. Table showing the general characterisitics of the studied groups.
There was no statistically significant difference between the two groups regarding the time until full effect was obtained (Table 2).
Globe akinesia expressed as median (range).
Time till onset of full effect expressed as median (range)±standard deviation.
Time till full motor recovery expressed as mean (range)±standard deviation.
Kremel test showed that the duration of globe akinesia was significantly higher in group F compared to group C (Table 2 and 3).
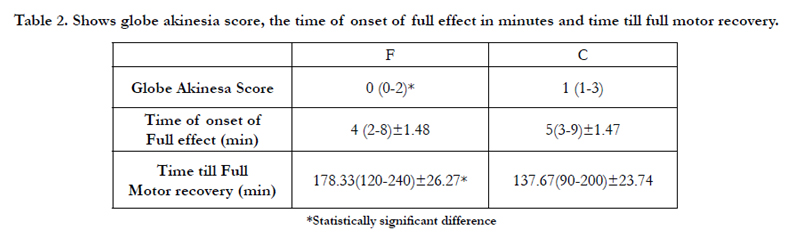
Table 2. Shows globe akinesia score, the time of onset of full effect in minutes and time till full motor recovery.
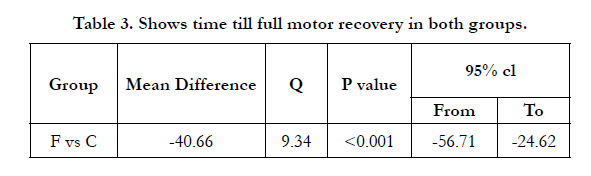
Table 3. Shows time till full motor recovery in both groups.
There was also no significant difference between the two groups in the lid akinesa score (Table 4).
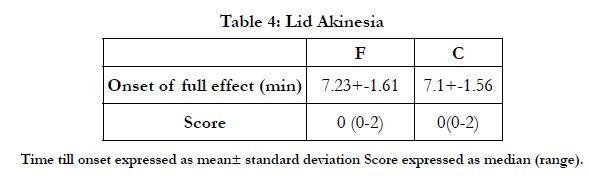
Table 4: Lid Akinesia
Comparison was made between the two groups and no significant difference was found between them (Table 5).
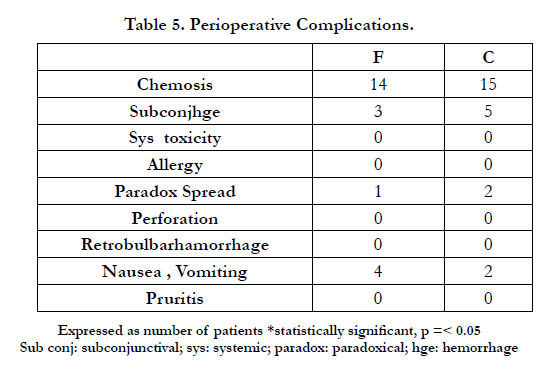
Table 5. Perioperative Complications.
Surgeon’s satisfaction was significantly higher in Group F compared to Group C (Table 6).
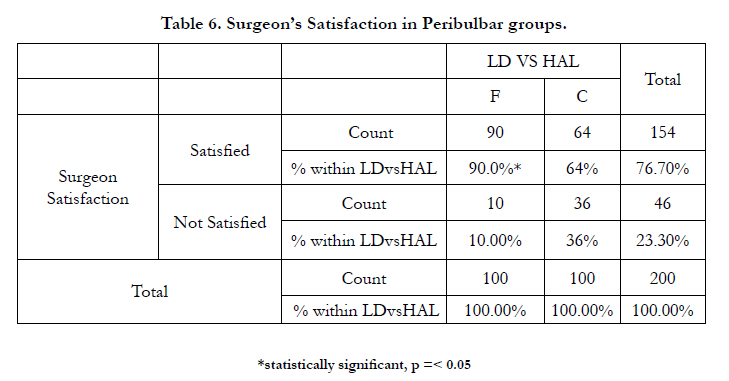
Table 6. Surgeon’s Satisfaction in Peribulbar groups.
Discussion
The use of local anesthesia during keratoplasty has the advantage of being safer for the patient as it carries a lower risk of postoperative vomiting and allows for safe transfer of the patient between rooms during femto keratoplasty. A major challenge for anesthetists is to maintain the effect of local anesthesia during the procedure without the need to switch to general anesthesia or provide top up doses. Many mixtures have been used especially the addition of epinephrine in order to prolong the effect of local anesthesia , however it is not preferred to be used in keratoplasty due to its mydriatic effect which renders the procedure very difficult and carries risks of lens injury f cataract extraction was not planned.
Opioids have been long used in conjunction with local anesthetics to consolidate the block intrathecally and in peripheral nerve blocks [4-7]. In our study we explored the effect of adding Fentanyl 30ug to the peribulbar block composed of 0.5% bupivacaine and 75ug Hyalase.
Our study showed that adding fentanyl significantly increased the duration of the block. In addition, surgeon’s satisfaction also increased denoting less need for top-up doses and less patient discomfort. There was no difference between the groups regarding onset of anesthesia or lid akinesia.
Similar findings were reported in a study investigating the effect of adding fentanyl to local anesthesia in vitrectomy surgeries, where not only the duration of the block was increased but also the onset of the block was also accelerated in the fentanyl group. [8] This difference could be explained by their smaller sample size as they only included 40 patients in their study as well as the anesthetic drugs used in the peribulbar block they used as they not only used fentanyl and bupivacaine 0.5% but they also used mepivacaine 3% which is a short and intermediate acting local anaesthetic which could explain the accelerated onset of the block . In another study conducted on the effect of the addition of fentanyl alone to local anesthetic solution compared to that of the addition of fentanyl and clonidine to peribulbar block during cataract surgery, it was found that the addition of both clonidine and fentanyl to local anesthetic solution prolonged the duration of the block for up to 3 hours. [9] Therefore, this offered the most satisfactory block for surgical conditions lasting up to 3h duration . However, the optimum dose of clonidine is still not exactly known (in this study they used a dose of 1 ug/kg) and with doses between 30 and 300 ug, it was evident that clonidine prolonged the duration of sensory and motor block but also increased the likelihood of hypotension, orthostatic hypotension, sedation and fainting . In addition, a lack of evidence of dose responsiveness for beneficial and harmful effects of clonidine was also noted rendering its use as an adjuvant to peribulbar block hazardous [10].
To our knowledge, few studies in literature discussed the effect of fentanyl on peri bulbar block and most of them discussed it in other ophthalmic surgeries than keratoplasty such as vitrectomy and cataract extraction. To our knowledge, this is the first study which highlights its effect on keratoplasty which might carry poor prognosis resulting from anesthetic complications.
Finally, this study demonstrated that the addition of fentanyl significantly potentiates the intensity of the peribulbar block and increases its duration rendering it very useful in peri bulbar blocks used in lengthy keratoplastic procedures thus rendering them safer with better prognosis after ruling out the possible anesthetic complications.
References
- M Muraine, E Calenda, L Watt, N Proust, A Cardon, et al. (1999) Peribulbar anesthesia during keratoplasty: a prospective study of 100 cases. Br J Ophthalmol 83(1): 104-109.
- Jorge L Alio (2013) Femtosecond laser assisted keratoplasty. (1stedn) Jaypee brothers medical publishers (P) Ltd,New Delhi,London, Philadelphia ,Panama.
- Alhassan MB, Kyari F, Ejere HO (2008) Peribulbar versus retrobulbar anaesthesia for cataract surgery. Anesth Analg 16(3): 1-30.
- Gunja N, Varshney K (2006) Brainstem anaesthesia after retrobulbar block: a rare cause of coma presenting to the emergency department. Emerg Med Australas 18(1): 83-85.
- Eghbal MH, et al. (2010) The effect of addition of low dose atracurium to local anesthetic in retrobulbar block for cataract surgery. Middle East J Anesthesiol 20(4): 535-538.
- Gaitini LA, et al. (2000) Does the addition of fentanyl to bupivacaine in caudal epidural block have an effect on the plasma level of catecholamines in children? Anesth Analg 90(5): 1029-1033.
- Palmer CM, et al. (1999) Bupivacaine augments intrathecal fentanyl for labor analgesia. Anesthesiology 91(1): 84-89.
- Abo El Enin MA, Amin IE, Abdelazeez AS, Mahdy MM, Moatafa MM (2009) Effect of Fentanyl Addition to Local Anaesthetic in Peribulbar Block. Indian J Anaesth. 53(1): 57–63.
- Fahmy NG, Fahmy AM, Kamal KY (2011) Effect of adding fentanyl and or clonidine to local anesthetic on prolongation of the peribulbar block in cataract surgery. Ain Shams J of Anesthiol 4(3): 41-47.
- Nael J, Rathmell JP (2013) Complications in regional anesthesia and pain medicine( 2nd edition) Wolters Kluwer,Lippincott Williams & Wilkins,Rhiladelphia, USA.





