Is Glaucoma an Optic Neuropathy?
Syed S. Hasnain*
* General Ophthalmology 560 W. Putnam Ave. Suite #6 Porterville, CA 93257, USA.
*Corresponding Author
Syed S. Hasnain,
General Ophthalmology, 560 W. Putnam Ave. Suite #6,Porterville,
CA 93257, USA.
Tel: 559.781.7482
Fax: 559.781.8446
Email: hasnain40@sbcglobal.net
Received: April 26, 2016; Accepted: August 17, 2016; Published: August 19, 2016
Citation: Syed S. Hasnain (2016) Is Glaucoma an Optic Neuropathy?. Int J Opthalmol Eye Res, S3:002, 8-11. doi: dx.doi.org/10.19070/2332-290X-SI03002
Copyright: Syed S. Hasnain© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Glaucoma is defined as an optic neuropathy implying that nerve fibers are being atrophied in glaucoma.
However, there are many distinctive morphological and histological features between the glaucomatous disc and nonglaucomatous optic atrophies. In glaucoma, there is always the orderly loss of nerve fibers starting with the peripheral fibers and ending with the central. In contrast, the nerve fibers loss in non-glaucomatous optic atrophies is always non-orderly. Furthermore, in glaucomatous discs there is development of disc excavation whereas no such excavation occurs in nonglaucomatous optic atrophies. This article will discuss the various distinctive features between glaucomatous disc and nonglaucomatous optic atrophies and conclude that the nerve fibers are being severed, not atrophied in glaucoma. Therefore, glaucoma may not be an optic neuropathy but an optic axotomy.
1.1 Why is excavation occurring in glaucomatous disc?
1.2 Why are the nerve fibers being severed in Glaucomatous Disc?
1.3 Do we have Evidence of Sinking LC and Severance of Nerve Fibers ?
1.4 Why Are the Nerve Fibers Being Destroyed in an Orderly Fashion?
2.Conclusion
3.References
Discussion
Excavation or formation of empty spaces is a unique feature of glaucomatous disc (GD). Excavation is also described as pathological cupping which is not an appropriate term since the term ‘cupping’ is being used to describe physiological cupping [1,2]. The use of the term ‘cupping’ describing both physiological as well as pathological cupping is creating unnecessary confusion in glaucoma diagnosis. There is no excavation occurring in nonglaucomatous optic atrophies (NGA) which are morphologically flat disc atrophies. The development of excavation in the GD implies that nerve fibers are disappearing permanently by some mechanism. The histology of end-stage glaucomatous disc (ESGD) reveals total disappearance of nerve fibers in contrast to the histology of NGA in which the nerve fibers though atrophied and shrunken, are still present.
It is hypothesized that in GD, the nerve fibers are being broken (severed), not being atrophied. The severance of the nerve fibers can explain the development of excavation and progressive thinning of nerve fibers as observed in GDs. Splinter hemorrhages in the GDs are due to severance of vasculature as they are meeting the fate of nerve fibers.
The Lamina Cribrosa (LC) is firmly kept in place by the border tissue of Elschnig (BT), lying between the scleral edge and the LC [3]. It is hypothesized that BT atrophies both in high-tension (HTG) and normal-tension glaucoma (NTG). Systemic circulatory pressure supplying the BT and IOP are opposing forces. Normally, the circulatory pressure supplying the BT should be higher than the IOP for the proper perfusion and healthy maintenance of the BT.
However, if this delicate situation is reversed, either due to raised IOP or if the systemic pressure supplying the BT becomes lower than the IOP due to systemic problems such as chronic hypotension, even normal range IOP can take the upper hand. In this scenario, the IOP will begin compressing the circulation of the BT thereby inducing chronic ischemia and its atrophy, thus NTG will ensue. Therefore, it is the IOP whether above or within normal range which is the cause of glaucoma in both HTG and NTG (Figure 1).
Due to atrophy of the BT, the LC will begin sinking resulting in stretching and ultimately severance of the prelaminar nerve fibers since one end is attached to the soma of the RGC and the other end anchored in the pores of the LC.
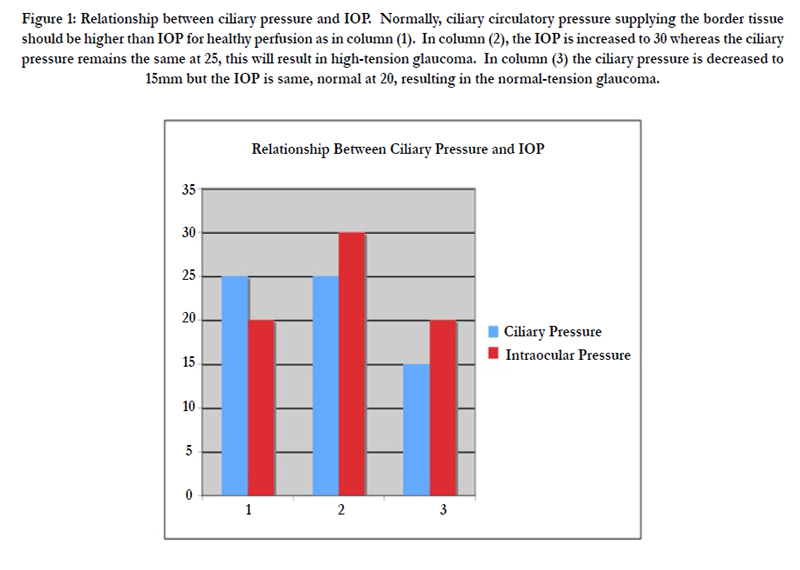
Figure 1: Relationship between ciliary pressure and IOP. Normally, ciliary circulatory pressure supplying the border tissue should be higher than IOP for healthy perfusion as in column (1). In column (2), the IOP is increased to 30 whereas the ciliary pressure remains the same at 25, this will result in high-tension glaucoma. In column (3) the ciliary pressure is decreased to 15mm but the IOP is same, normal at 20, resulting in the normal-tension glaucoma.
Sloping and kinking of the blood vessels at disc margin in GDs prior to any change in the contour of the physiological cup suggests the LC is sinking in the scleral canal. The blood vessels at the disc margin start turning inward in the pursuit of sinking LC. Since no sinking of LC is occurring in NGAs, there is no sloping/ kinking of blood vessels in such cases.
The posterior migration of LC from early stages of glaucoma has been documented in several studies [4,5]. Progressive thinning of the RNFL in GDs can only be explained due to severance of nerve fibers as it is not occurring in non-glaucomatous optic atrophies. The wedge shaped retinal spaces in glaucoma are due to severance and depletion of arcuate nerve fibers and notching due to their depletion at the site of entry in the disc. Notching at the poles of the disc is the initial excavation in the disc and a confirmatory sign of glaucoma.
It is proposed that all the 360 degrees of retinal fibers are being severed simultaneously, however the arcuate fibers being fewer in number compared to the rest are depleted earlier resulting in arcuate field defects, not due to their increased vulnerability or sensitivity. The histology of the end-stage glaucomatous disc is not a 100% cupped LC, but an empty crater left over after severance and phagocytosis of severed nerve fibers. In contrast, the histology of the non-glaucomatous optic atrophy reveals presence of nerve fibers though atrophied and shrunken [6].
Before we discuss the orderly destruction of nerve fibers in glaucoma it is imperative to mention the arrangement of the nerve fibers in the retina/optic disc [7].
About one million or so nerve fibers originating from the RGC’s leave the eyeball through meshwork of the Lamina Cribrosa (LC) and form the optic disc. There are two main aspects in which the nerve fibers are arranged in the retina and optic disc. First, the nerve fibers in the retina are arranged in layers superficial to deep. The fibers originating closest to the disc lie most superficial (closest to vitreous) and exit from the most central part of the disc whereas nerve fibers originating from most peripheral retina lie deepest (closest to sclera) and exit closest to the edge of the scleral opening. Second, the nerve fibers originating from the nasal retina proceed directly to the nasal part of the disc and much of the macular fibers proceed horizontally to the temporal part of disc. However, the fibers originating from the temporal macular area and temporal peripheral retina arch above and below the macular fibers to reach the disc, hence known as arcuate fibers.
On one aspect in glaucoma where we all have consensus: the one million or so densely packed nerve fibers in glaucoma are always being destroyed in an orderly sequence from peripheral to central, never randomly. If this was not true, then the role of perimetry in glaucoma would be meaningless. If the nerve fibers are being destroyed in an orderly sequence in glaucoma then we should expect the mechanism for their destruction to be an orderly one as well.
The concept of atrophy of the nerve fibers has failed to explain the orderly destruction of nerve fibers occurring in glaucoma. For any glaucoma theory to prevail, it must explain the orderly destruction of nerve fibers otherwise it will be of no value. In light of the orderly destruction of nerve fibers all the prevailing glaucoma theories such as the direct role of raised IOP, apoptosis, neurodegeneration, increased sensitivity of the disc to IOP, posterior bowing of the lamina cribrosa or cupping become invalid. These theories can’t explain the orderly destruction of nerve fibers in glaucoma.
The sinking of the LC and severance of the nerve fibers can explain their orderly destruction in glaucoma. As the LC sinks, the peripheral nerve fibers being closest to the scleral edge are stretched and broken first, As a result, the next central fiber will move towards the periphery to occupy the space vacated by the preceding severed fiber and thus also get stretched and severed at the scleral edge (Figure 2).
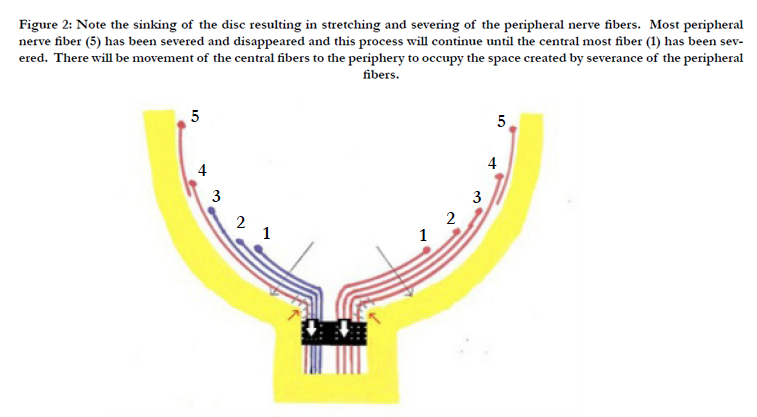
Figure 2: Note the sinking of the disc resulting in stretching and severing of the peripheral nerve fibers. Most peripheral nerve fiber (5) has been severed and disappeared and this process will continue until the central most fiber (1) has been severed. There will be movement of the central fibers to the periphery to occupy the space created by severance of the peripheral fibers.
In addition to the border tissue, the 360 degrees of nerve fibers also anchor the LC as roots anchor a tree. Thus, the severance of nerve fibers leads to further disc sinking.
The cascade of severance of the nerve fibers and sinking disc would become self-propagated and will continue until all the nerve fibers have moved in an orderly tandem fashion to the scleral edge and get severed. This may explain the unstoppable nature of glaucoma despite maximum lowering of IOP. The severed segments undergo phagocytosis and thus will create empty spaces or excavation that we may be interpreting as cupping of the disc. Only the prelaminar nerve fibers can be destroyed in an orderly tandem fashion since they are still loose and have not yet fastened in bundles in the pores of the LC [8, 9].
Once the nerve fibers are anchored in bundles in the pores of the LC, the nerve fibers can’t be separated individually and thus their orderly tandem destruction is not possible. Therefore, the LC may not be the site of injury in glaucoma as commonly believed. Sinking of the disc and severing of the nerve fibers will become self-propagated and will continue until all the nerve fibers are severed beginning with the peripheral and ending with central fibers in an orderly fashion and this is what’s revealed by glaucomatous field defects. Wedge-shaped defects in the retina pertaining to the area of the arcuate fibers location are due to the severance of nerve fibers, not due to their atrophy. Such retinal defects do not occur in NGA. Nasal shifting of the central retinal vessels can be explained by loss of anchorage resulting from the severance of temporal nerve fibers.
Conclusion
The sloping/kinking of the blood vessels at disc margin, prior to any change in the contour of the physiological cup, suggests that the optic disc may be sinking in glaucoma. The development of excavation, wedge retinal defects, arcuate field defects, progressive thinning of the RNFL suggests that the nerve fibers are being severed in glaucoma as such events cannot occur if nerve fibers are being atrophied. Hemorrhages at the disc margin may be due to severance of the smaller vessels. Histology of ESGD – a totally empty bean-pot, supports the fact that the nerve fibers have disappeared after their severance in glaucoma. Most importantly, the orderly destruction of nerve fibers in glaucoma can only be achieved due to a mechanical affect (sinking disc) and not as a result of any biological phenomenon. In summary, glaucoma may not be an optic neuropathy but an optic axotomy.
References
- Hasnain SS (2006) Scleral edge, not optic disc or retina is the primary site of injury in chronic glaucoma. Med Hypotheses 67(6) : 1320-1325.
- Hasnain SS (2012) Pathogenesis of Arcuate Field Defects. Highlights of Ophthalmology. Panama 40(6): 1-6.
- Wolff E (1968) Anatomy of the eye and orbit. (6th edn), H.K. Lewis & Co, London. 326.
- Yang H, Williams G, Downs JC, Sigal IA, Roberts MD, et al., (2011) Posterior (outward) migration of the Lamina Cribrosa and early cupping in monkey experimental glaucoma. Invest Ophthalmol Vis Sci 52(10): 7109-7121.
- Yang H, G Williams, J Downs, I Sigal, M Roberts,et al., (2010) Optic Nerve Head (ONH) Lamina Cribrosa Insertion Migration and Pialization in Early Non-Human Primate Experimental Glaucoma. Poster Presentation ARVO Annual Meeting 51(13): 1631.
- Yanoff M, Fine BS (1975) Ocular pathology: A Text and Atlas. Harper & Row Publishers, Philadelphia 496-615.
- Shields MB (1992) Textbook of Glaucoma. (3rd edn), Williams & Wilkens, Baltimore. 515-516.
- Hasnain SS (2016) The Missing Piece in Glaucoma? Open Journal Of Ophthalmology 6(1): 56-62. doi: 10.4236/ojoph.2016.61008.
- Zeried FM, Osuagwu UL (2013) Changes in retinal nerve fiber layer and optic disc algorithms by optical coherence tomography in glaucomatous Arab subjects. Clini Ophthalmol 7: 1941–1949.





