Prospective Study on the Effect of Selective Laser Trabeculoplasty in Normal Tension Glaucoma
De Keyser M1*, De Belder M2, De Groot V1,3
1 Department of Medicine, University of Antwerp, Universiteitsplein 1, Antwerp, Belgium.
2 Department of Experimental Psychology, Ghent University, Henri Dunantlaan 2, Belgium.
3 Department of Ophthalmology, Antwerp University Hospital, Wilrijkstraat 10, Antwerp, Belgium.
*Corresponding Author
Myrjam De Keyser, MD,
Department of Medicine, University of Antwerp,
Universiteitsplein 1, B-2610 Antwerp, Belgium.
Tel: 0032/473893001
E-mail: Myrjam@bijzonder.be
Received: August 22, 2016; Accepted: September 15, 2016;Published: September 19, 2016
Citation: De Keyser M, De Belder M, De Groot V (2016) Prospective Study on the Effect of Selective Laser Trabeculoplasty in Normal Tension Glaucoma. Int J Opthalmol Eye Res, S1:008, 36-41. doi: dx.doi.org/10.19070/2332-290X-SI01008
Copyright: De Keyser M© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribu tion and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: Compare the effect of selective laser trabeculoplasty (SLT) in normal tension glaucoma (NTG) patients with its effect in primary open angle and ocular hypertension patients (POAG/OHT), considering both evolution of intraocular pressure (IOP) and mean number of medication.
Method: Prospective trial of 130 patients on glaucoma medication. Patients were offered SLT as a means to diminish medication use. Both eyes of the patient underwent SLT. Laser was performed over 360°, 100 spots, 3nsec, 400 μm. IOP and medication were recorded at 1 hour, 1 week, 1, 3, 6, 12 and 18 months. Results were compared with a control group of patients that remained on medication.
Results: IOP changed little after SLT, as the groups were controlled under medication. Nevertheless, SLT was able to achieve additional IOP reduction: 9% and 6% respectively after 12 and 18 months in the NTG group and 19% and 2% respectively in the POAG/OHT group.
The use of medication lowered significantly: from a mean of 1.20 in the NTG group to 0.19 and from 1.71 to 0.31 in the POAG/OHT group. This was a significant change compared to the control groups. Mean reduction of medication after SLT was comparable between the NTG and the POAG/OHT group at 1 week, 1 month, 3,6 and 12 months.
Conclusions: The efficacy of SLT is not inferior in NTG patients compared to POAG or OHT patients.
2.Introduction
3.Materials and Methods
3.1 Study design and subjects
3.2 Baseline examinations
3.3 Laser technique
3.4 Postoperative management
3.5 Statistical methods
4.Results
4.1 Population
4.2 Laser technique
4.3 Evolution of IOP
4.4 Evolution of medication
5.Discussion
6.Conclusions
7.References
KeyWords
Selective Laser Trabeculoplasty; Normal Tension Glaucoma; Open Angle Glaucoma; Ocular Hypertension.
Introduction
Normal tension glaucoma (NTG) is a type of progressive optic neuropathy where intra ocular pressure (IOP) is within the statistically normal range (≤ 21 mmHg), but where optic nerve damage and visual field loss appear like in patients with primary open angle glaucoma (POAG) related to an elevated IOP [1-3].
Pathogenesis of NTG seems to involve both IOP dependent and IOP independent mechanisms that work individually or in combination. Increased IOP can distort the lamina cribrosa and interfere with axoplasmatic flow or create hypo-perfusion of the optic nerve head. On the other hand a high incidence of vascular insufficiency has been demonstrated in NTG patients, leading to perfusion deficits of the optic nerve head, the retina, the choroid and the retro-bulbar vessels [2, 4-6].
For many years it was unclear whether lowering IOP in NTG patients from somewhere within the normal range to a lower value was useful. The Collaborative Normal Tension Glaucoma Study however showed that there was a slower progression of visual field loss in NTG patients with 30% or more lowering of their IOP [1].
Laser trabeculoplasty has demonstrated its efficacy in lowering IOP in POAG [7, 8]. Studies on its use for NTG patients are scarcer. The incidence of NTG in different populations is not the same. In the western world, 30 to 40 percent of people with glaucomatous visual field defect have normal IOPs [9, 10]. A much higher incidence of NTG has been reported in Asian populations, with NTG accounting for as many as 77 to 92% of the primary open angle glaucoma (POAG) patients in respectively Korea and Japan [2, 3]. Several Asian studies report on the use of SLT in NTG patients [3, 11-13] and one study in the USA [14]. Information on SLT and NTG in a European setting is rare.
We aimed to examine the efficiency of SLT in NTG patients in a prospective study, assessing evolution of IOP and medication use after SLT.
Materials and Methods
A prospective, randomized clinical trial including 145 patients of the glaucoma consultation at ZNA Jan Palfijn Hospital, Merksem. The trial was registered as NTR5417.
Approval of the ethics committee of the clinic was obtained (4313 MEC).
Inclusion criteria concerned patients with primary open angle glaucoma (POAG), normal tension glaucoma (NTG) and ocular hypertension (OHT), controlled with medical therapy. Only patients with recording of all data at minimal time points were included. Patients had to agree to sign an informed consent form. Exclusion criteria were other types of glaucoma than open angle glaucoma and previous trabeculectomy or SLT. Patients with a corneal disease that inhibited good visualization of the trabecular meshwork (TM) and those taking systemic steroids were also excluded from the study.
POAG was defined as IOP above 21 mmHg on several separate occasions and different hours, open angle on gonioscopy and either glaucomatous visual field defects on Humphrey visual field analyzer, optic disc changes on funduscopy and/or loss of retinal nerve fiber layer on Optical Coherence Tomography (OCT). OHT was set as a mean IOP higher than 21 mmHg in the absence of field or disc changes or defects in retinal nerve fiber layer.
NTG was defined as analogue changes in visual field, optic disc and/or retinal nerve fiber layer but with a Goldman napplanation measured IOP always ≤ 21 mmHg 134.
Randomization was performed with a computer-generated allocation schedule; only after introduction of patient data, the allocated group became clear. Both eyes received SLT. Primary outcome measure: IOP and/or medication lowering effect of SLT.
At baseline a full ophthalmologic examination of both eyes was conducted, including best corrected visual acuity, IOP measurement by Goldmann applanation tonometry (two measurements were taken and the mean calculated), slit lamp examination of the anterior segment (conjunctival injection, cornea, iris, lens appearance), corneal thickness measurement, gonioscopy, dilated fundus examination, visual field examination by computerized perimetry (program 24-2, Humphrey Field Analyzer 745i, Zeiss, Jena, Germany) and Optical Coherence Tomography (OCT) of the optic nerve head. All OCT scans were performed with the spectraldomain OCT RTVue (Optovue, Fremont, USA). IOP at start was calculated as the mean of the last three measurements made prior to SLT on different days and hours.
Immediately before the laser procedure a drop op pilocarpine 1% and apraclonidine 0,5% were instilled into the operative eye. A frequency doubled, Q-switched Nd:YAG laser was used, emitting at 532 nm, with a pulse duration of 3 nsec, a spot size of 400 μm and pulse energies ranging from 0, 2 to 1, 7 mJ, coupled to a slit lamp delivery system.
Using the 400 μm spot size, the entire width of the trabecular meshwork was irradiated with each pulse. The laser energy was initially set at 0, 9 mJ and a single laser pulse was delivered at the 12 O’clock position. If a cavitation bubble appeared, the laser energy was reduced by 0, 1 mJ increments until minimal bubble formation was observed. Treatment was then continued at this energy level [15]. If no cavitation bubble was observed, the pulse energy was increased by steps of 0, 1 mJ until bubble formation.
Immediately before the laser procedure a drop of pilocarpine 1% and apraclonidine 0.5% were instilled into the treated eye. After the laser treatment, patients received indomethacin 0.1% or dexamethasone 0.1% three times a day for one week or no anti-inflammatory drops, following study protocol. The observation that post-laser treatment did not make a difference in IOP or medication lowering effect of SLT was published previously [16].
Patients were examined at 1 hour, 1 week, 1, 3, 6, 12 and 18 months after SLT. At 6 months the same parameters as at baseline were assessed. Glaucoma drops were continued until IOP was more than 2 mmHg below target pressure, at which point they were stopped. Fixed combinations were considered to be two medications and were stopped one by one. At least three months of wash out period passed before a second medication was stopped.
An independent-samples t-test was performed to compare baseline differences between the groups for continuous variables (i.e. age, IOP at baseline, best corrected visual acuity, central corneal thickness, cup disc ratio, visual field mean deficit and pattern standard deviation, OCT focal loss of volume, IOP before treatment, number of medications at baseline). A Chi-squared analysis was performed to compare sex and type of glaucoma.
A second independent-samples t-test was executed to investigate the difference in evolution of mean IOP for both groups at all time points. The same analysis was run to investigate the time evolution in number of used medications.
Results of statistical analysis with p-values < 0.05 were considered to be significant.
Results
72 patients were appointed to the SLT group; 69 of them completed a minimum six months of follow up, giving a total of 135 eyes. Among these were 56 NTG eyes and 79 eyes with POAG or OHT. 73 patients were assigned to the control group; 61 appeared at the scheduled appointments; 116 eyes were retained. 36 had NTG, 80 had POAG or OHT. The mean follow up was 12.76 ± 5.97 months. Demographic and baseline characteristics are shown in Table 1. No significant differences were present between the SLT and the control group in terms of mean age, sex, type of glaucoma, best corrected visual acuity, central corneal thickness (CCT), visual field, OCT, IOP before start of medication and mean medication taken at baseline.
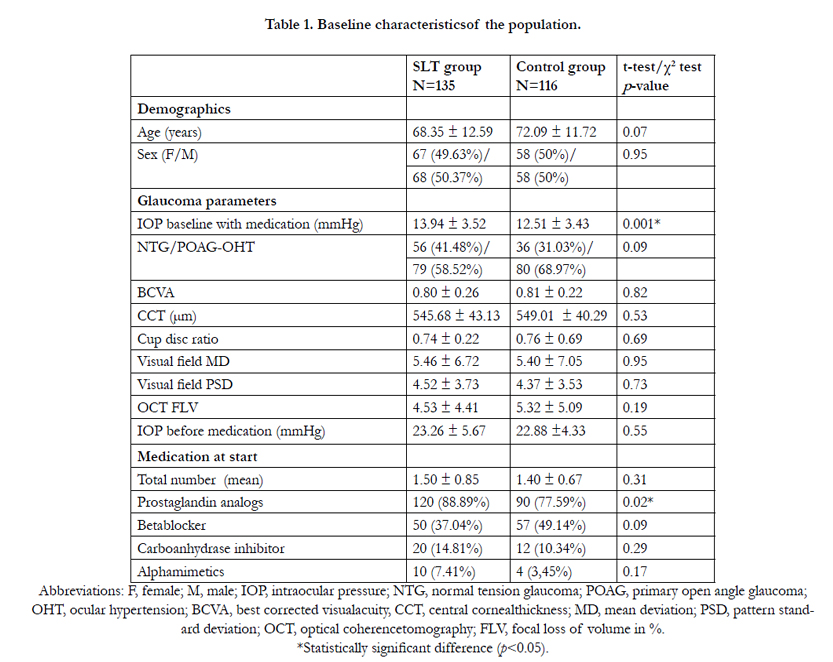

Table 1. Baseline characteristicsof the population.
There was a significant difference in IOP at baseline, with a higher mean IOP in the SLT group; 13.94 compared to 12.51 mmHg in the control group. A larger percentage of patients in the SLT group took prostaglandins at baseline. However, pre-laser use of prostaglandins has proven to have no influence on the efficiency of SLT [17].
We used a Lumenis Selecta II laser (Lumenis, Dreieich, Germany). Mean energy used was 1.09 ± 0.31 mJ. Patients received a mean of 102.37 ± 9.34 spots over 360° of the TM. The same experienced surgeon (MDK) applied all treatments.
The health coaching intervention offered support for behavior change to help improve eye health and general health. Benefits of the health coaching were seen in eye health and general health. With regards to eye health, participants developed specific strategies to improve adherence as well as enhanced self-awareness about their vision and disease. With regards to general health, the benefits included weight loss and diet changes, more exercise, adjustments to work-life balance with more family time, and reconnection to primary care.
IOP did not change significantly over time in both SLT and control groups, as was expected in this medically controlled population. There was no significant IOP difference between NTG patients that received SLT and those that remained on medication. At baseline, there was a higher IPO in the group of POAG/OHT patients that had SLT compared to their control group. This difference remained after SLT. See Table 2.
Although IOP was controlled under medication, SLT was able to produce an additional IOP reduction of 9% and 6% respectively after 12 and 18 months in the NTG group and 19% and 2% respectively in the POAG/OHT group.
The percentage of IOP reduction after SLT was comparable between the NTG and the POAG/OHT group at most time points. At 18 months after SLT, the reduction in IOP was significantly less in the POAG/OHT group. See Table 3.
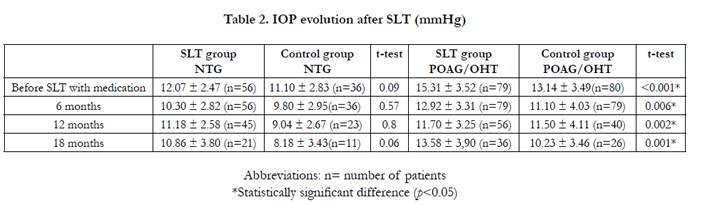
Table 2. IOP evolution after SLT (mmHg)
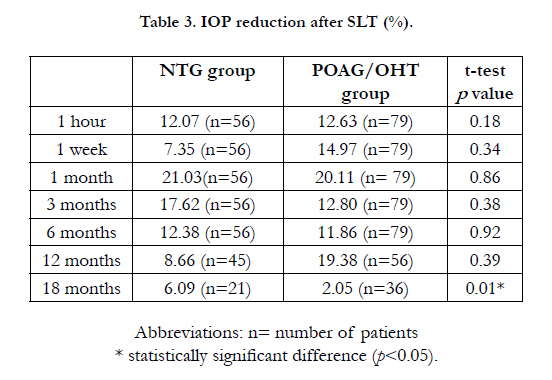
Table 3. IOP reduction after SLT (%).
Compared to their control groups, the use of medication lowered significantly both in the NTG and the POAG/OHT group. From 1.2 to 0.19 medications in the NTG group and from 1.71 to 0.31 in the POAG/OHT group. See Table 4.
The mean reduction of medication after SLT was comparable in the NTG and the POAG/OHT group at all time points. See table 5.
In the NTG group, 76% of the medication could be stopped after 18 months, in the POAG/OHT even 90%.
In the control group, mean medication use remained the same.
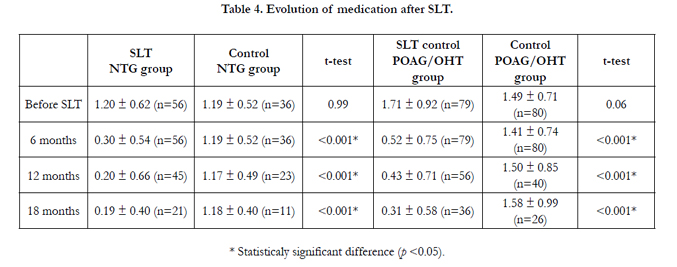
Table 4. Evolution of medication after SLT.
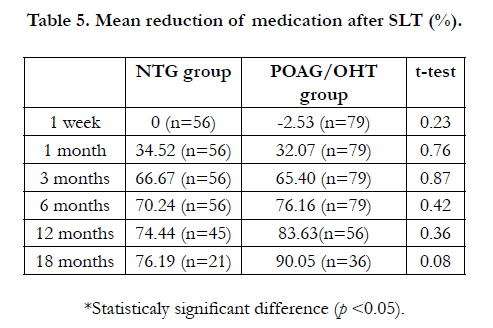
Table 5. Mean reduction of medication after SLT (%).
Discussion
IOP reduction remains the most important modifiable risk factor to slow down the progression of NTG. This can be achieved with medication, laser or surgery. Since its launch in 1997 by Latina et al., [15], SLT has proven to be efficient [7, 8] and to bypass the inconveniences [18, 19], costs [20] and side effects [21, 22] of medication. High pre-laser IOP has proven to be predictive of better IOP lowering results after SLT [23-26]. This may make it less applicable for NTG patients.
SLT works on a cellular [27] and a biochemical level [28], enhancing the outflow capacity of the trabecular meshwork with minimal tissue damage [29]. The pathogenesis of NTG however, seems to be different from the mechanisms active in POAG and OHT. Changes in the lamina cribrosa and axoplasmatic flow and a high incidence of vascular insufficiency have been demonstrated in NTG patients [2, 4-6]. It is therefore not inconceivable that eyes with NTG may react differently to SLT than POAG or OHT eyes.
Lee et al., published prospective studies [3, 30] on the use of SLT in NTG patients, proving the value of SLT. A single session of SLT achieved an additional 15% IOP reduction while using 27% less medication at one year [3]. Their patients were Asian; in this population, the prevalence of NTG varies from 77 to 92% [2, 3]. In our European population, only 30 to 40 percent of people with glaucomatous visual field defect have normal IOPs [9, 10].
Our study confirms the usefulness of SLT in European NTG patients. We started out with a group of patients, controlled under medication. SLT was able to keep the IOP low in the NTG and the POAG/OHT group to a comparable degree. Although IOP was controlled under medication, SLT was able to produce an additional IOP reduction of 9% and 6% respectively after 12 and 18 months in the NTG group and 19% and 2% respectively in the POAG/OHT group.
Laser also lowered the amount of medication needed to the same amount in both groups; a 76% reduction of medication in the NTG group and a 90% reduction in the POAG/OHT group after SLT. The difference was not significant. We were able to compare these groups to control groups that stayed on their medication and the medication changes were significant at all time points.
Our study has its limitations; IOP measurement before SLT was performed between 8 am and 4 pm. Diurnal changes in IOP were not evaluated further. The three measurements before baseline were taken with an interval of 4 to 6 months between examinations. We recognize the consistency of the baseline IOP values may be limited.
Conclusions
The efficacy of SLT is not inferior in NTG patients compared to POAG or OHT patients.
References
- Anderson DR, Normal Tension Glaucoma Study (2003) Collaborative normal tension glaucoma study. Curr Opin Ophthalmol. 14(2): 86–90.
- Xue-Song Mi X, Yuan T-F, So K-F (2014) The current research status of normal tension glaucoma. Clin Interv Aging. 9: 1563-1571.
- Lee JWY, Gangwani RA, Chan JCH, Lai JSM (2015) Prospective Study on the Efficacy of Treating Normal Tension Glaucoma With a Single Session of Selective Laser Trabeculoplasty. J Glaucoma. 24(1): 77–80.
- Babar TF et al., (2006) Normal Tension Glaucoma. Pak J Ophth. 22(2): 60-67.
- Tsai (2006) Current Concepts in Normal Tension Glaucoma. 6:1–5.
- Mroczkowska S, Benavente-Perez A, Negi A, Sung V, Patel SR, Gherghel D (2013) Primary Open-Angle Glaucoma vs Normal-Tension Glaucoma.JAMA Ophthalmol. 131(1): 36-43.
- Wong MO, Lee JW, Choy BN, et al., (2015) Systematic review and metaanalysis on the efficacy of selective laser trabeculoplasty in open-angle glaucoma. Surv Ophthalmol. 60(1): 36–50.
- Li X, Wang W, Zhang X (2015) Meta-analysis of selective laser trabeculoplasty versus topical medication in the treatment of open-angle glaucoma.BMC Ophthalmol. 15:1–9.
- Klein BE, Klein R, Sponsel WE, et al., (1992) Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology. 99(10): 1499–1504.
- Dielemans I, Vingerling JR, Wolfs RC, Hofman A, Grobbee DE, de Jong PT (1994) The prevalence of primary open-angle glaucoma in a population- based study in The Netherlands. The Rotterdam Study. Ophthalmology.101(11): 1851–1855.
- Tojo N, Oka M, Miyakoshi A, Ozaki H, Hayashi A (2014) Comparison of Fluctuations of Intraocular Pressure Before and After Selective Laser Trabeculoplasty in Normal-tension Glaucoma Patients. J Glaucoma. 23(8):e138–e143.
- Nitta K, Sugiyama K, Mawatari Y, Tanahashi T (2013) [Results of selective laser trabeculoplasty (SLT) as initial treatment for normal tension glaucoma]. Nippon Ganka Gakkai Zasshi. 117(4): 335–343.
- Lee JW, Ho WL, Chan JC, Lai JS (2015) Efficacy of selective laser trabeculoplasty for normal tension glaucoma: 1 year results. BMC Ophth. 15(1):1–6.
- Mallah El MK, Walsh MM, Stinnett SS, Asrani SG (2010) Selective laser trabeculoplasty reduces mean IOP and IOP variation in normal tension glaucoma patients. Clin Opthamol. 4: 889–893.
- Latina MA, Sibayan SA, Shin DH, Noecker RJ, Marcellino G (1998) Qswitched 532-nm Nd:YAG laser trabeculoplasty (selective laser trabeculoplasty) - A multicenter, pilot, clinical study. Ophthalmology. 105(11): 2082-2088.
- De Keyser M, De Belder M, De Groot V (2016) Randomised prospective study of the use if anti-inflammatory drops after selective laser trabeculoplasty. J Glauc.
- Singh D, Coote MA, Hare FOA, et al., (2009) Topical prostaglandin analogues do not affect selective laser trabeculoplasty outcomes. Eye. 23(12): 2194–2199.
- Pisella PJ, Pouliquen P, Baudouin C (2002) Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 86(4): 418–423.
- Nordmann J-P, Auzanneau N, Ricard S, Berdeaux G (2003) Vision related quality of life and topical glaucoma treatment side effects. Health Qual Life Outcomes. 1:75.
- Cantor LB, Katz LJ, Cheng JW, Chen E, Tong KB, Peabody JW (2008) Economic evaluation of medication, laser trabeculoplasty and filtering surgeries in treating patients with glaucoma in the US. Curr Med Res Opin. 24(10): 2905–2918.
- Terai, Müller-Holz, Spoerl E, Pillunat LE (2011) Short-term effect of topical antiglaucoma medication on tear-film stability, tear secretion, and corneal sensitivity in healthy subjects. Clin Ophthalmol. 5: 517-525.
- Baudouin C (2008) Detrimental effect of preservatives in eyedrops: implications for the treatment of glaucoma. Acta Ophthalmol. 86(7): 716–726.
- Ayala M, Chen E (2011) Predictive factors of success in selective laser trabeculoplasty (SLT) treatment. Clin Ophth. 5:573-576.
- Bruen R, Lesk MR, Harasymowycz P (2012) Baseline Factors Predictive of SLT Response: A Prospective Study. Journal of Ophthalmology. 11:1–5.
- Hodge WG et al., (2005) Baseline IOP predicts selective laser trabeculoplasty success at 1 year post-treatment: results from a randomised clinical trial. Br J Ophthalmol. 89(9):1157–1160.
- Lee JY, Lee YK, Moon JI et al., (2014) Long-Term Outcomes and Predictive Factors for Success of Selective Laser Trabeculoplasty. J Kor Ophth Soc. 55(9): 1347-1354.
- Bylsma SS, Samples JR, Acott TS, Van Buskirk EM (1988) Trabecular cell division after argon laser trabeculoplasty. Arch Ophthalmol. 106(4): 544– 547.
- Bradley JM, Anderssohn AM, Colvis CM, et al., (2000) Mediation of laser trabeculoplasty-induced matrix metalloproteinase expression by IL-1beta and TNFalpha. Invest Ophthalmol Vis Sci. 41(2): 422–430.
- Cvenkel B, Hvala A, Drnov ek-Olup B, Gale N (2003) Acute ultrastructural changes of the trabecular meshwork after selective laser trabeculoplasty and low power argon laser trabeculoplasty. Lasers Surg Med. 33(3): 204–208.
- Lee JWY, Shum JJW, Chan JCH, Lai JSM (2015) Two-Year Clinical Results After Selective Laser Trabeculoplasty for Normal Tension Glaucoma. Medicine. 94(24):e984.





