To Study the Effect of Silicone Tube Intubation with and without Mitomycin C in Revision of Failed Dacryocystorhinostomy Surgery
Verma S1, Priti G1*
1 Department of Ophthalmology, JNU Institute for Medical Sciences and Research Centre, Jaipur, Rajasthan, India.
*Corresponding Author
Gupta Priti, MS (Ophthalmology),
Department of Ophthalmology, JNU Institute for Medical Sciences and Research Centre,
Jaipur, Rajasthan, India.
E-mail: pritigupta089@gmail.com
Received: November 13, 2017; Accepted: January 09, 2018; Published: January 11, 2018
Citation: Verma S, Priti G. To Study the Effect of Silicone Tube Intubation with and without Mitomycin C in Revision of Failed Dacryocystorhinostomy Surgery. Int J Ophthalmol Eye Res. 2017;6(1):358-362. doi: dx.doi.org/10.19070/2332-290X-1800072
Copyright: Priti G© 2018. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aims: To study the effect of silicone tube intubation with and without mitomycin c in revision of external dacryocystorhinostomy following failed dacryocystorhinostomy (DCR) surgery.
Settings and Design: A Retrospective study.
Materials and Methods: A retrospective review of patients who underwent revision of external DCR between november 2012 and march 2015 at teaching institute. In this study 45 patients of failed DCR were included, 30 of them were endoscopic DCR, and 15 were External DCR. In this study mitomycin c (MMC) was applied in 20/45 patients and silicone tube intubation done in all 45 patients. The tube was removed at 3 months after surgery.
Statistical Analysis: Statistical analysis was carried out using SPSS statistical software package (Version 16.0; SPSS).
Results: At the last examination, 3 patients still had epiphora 6.67%, and their nasolacrimal passage was obstructed. 42 patients had no complaints, and their lacrimal system was patent (93.33%).
Conclusion: We concluded that revision of failed dcr surgery with silicone tube intubation and mitomycin c has good results. Mitomycin c can be used in selective cases in which excessive fibrosis and granulation tissue was found intraoperatively.
2.Introduction
3.Subject and Methods
3.1 Surgical Method
4.Observations and Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
External Dacryocystorhinostomy (DCR); Mitomycin C; Silicone Tube Intubation.
Introduction
Conventional (external approach) dacryocystorhinostomy (DCR) is indicated for obstruction distal to the medial opening of the common canaliculus, and consists of anastomosis of the lacrimal sac to the mucosa of the middle nasal meatus. To increase the success rate of surgery the causes of failure must be find out. The following causes can lead to failure of dcr surgery [1].
• Reclosure of the stoma as the most frequent cause for failure of dacryocystorhinostomy.
Reclosure is due to scarring, adhesions and granulation tissue formation.
• Incorrect position of the anastamosis (high anastamosis).
• Poor surgical procedure.
To increase the success rate of failed dcr application of antimitotic agent like mitimycin C and silicone tube intubation is very usefull [2, 3]. Mitomicin ‘c’ (MMC) is an antibiotic, anti-neoplastic, antifibrotic agent isolated from streptomyces caespitosis. It inhibits RNA, DNA and protein synthesis and usually used in systemic anticancer therapy. The inhibitory action of MMC on fibroblast proliferation has led to its successful application in glaucoma surgery and in addition to pterygium surgery it has been successfully applied in other indications in ocular surface surgery, including ocular surface neoplasia and symblepharon repair for ocular- cicatricial pemphigoid [4]. Mitomycin-C use during external DCR surgery is safe and effective and it results in good outcome of DCR surgery [5, 6]. Races with higher level of melanin in body tissues are more prone to develop tissue fibrosis during wound healing [2]. Silicone tube allows epithelisation around tubes and the nasal opening can remain patent even after the removal of tubing. The two malleable and convenient probes help in easier insertion through the punctum.
Need for the study: The most common cause of DCR failure is occlusion of the rhinostomy site by soft tissue, common canalicular obstruction, cicatricial ostium closure, formation of synechiae between the ostium and the middle turbinate or the septum, and granuloma formation at the ostium. To avoid these complications we want to use silicone tube and mitomycin c during revision of failed DCR cases.
Subject and Methods
This experimental study was conducted for a period of November 2012 to february 2015 at teaching institute. 45 patients were selected, who had undergone external DCR for chronic dacryocystitis and complaining of constant epiphora and discharge following previous external DCR surgery of more than six months duration. We made two groups of patients, group A and group B.
Group A (25 patients ) included patients of previously failed DCR surgery, which was managed by revision of DCR surgery with silicone tube intubation. Group B (20 patients) included patients of previously failed DCR surgery, which was managed by revision of DCR surgery with silicone tube intubation with mitomycin-C. Mitomycin c was applied only in patients with excessive fibrosis found during surgery.
Inclusion criteria: Patients between 20 and 70 years of age, who underwent DCR surgery for chronic dacryocystitis and still complaining for constant epiphora and discharge.
Exclusion criteria: Included history of trauma, or nasal and paranasal sinuses pathology, acute dacryocystitis and patients who were not come for regular followup.
Preoperatively, in all patients visual acuity, slit lamp and fundus examination was done. To confirm nasolacrimal duct obstruction, lacrimal sac syringing was done in all 45 patients. All patients were sent to ENT specialist for nasal cavity and paranasal sinus examanination to detect any pathology. Patients having any nasal and paranasal sinus pathology were excluded from our study.
The procedure is usually performed under general anaesthesia. A vertical skin incision is made 10 mm medial to the inner canthus, the medial canthal tendon and lacrimal sac exposed and reflected, and after removal of the intervening bone the sac is incised. A metallic probe was inserted from lower canaliculus after the puncta were dilated. A small incision with the scalpel at the tip of the probe, then H-type incision was made with the scissors on the lacrimal sac. The same H-type incision was also made on the nasal mucosa,then the mucosal flaps were sutured to the flaps of lacrimal sac. Silicone tube intubation was made after the posterior flaps anastomoses. The two ends of the silicone rod were retrieved from the nose and tied then pushed into the nose. In patients with excessive fibrosis was found during surgery, mitomycin- C was applied, a piece of cellulose sponge saturated with 0.02% mg/ml mitomycin-C was placed over the anastomosed posterior flaps and osteotomy site. After 2 minutes of application, the cellulose sponge soaked with MMC was removed through the nostril. Flaps and subcutaneous tissues were sutured with 6-0 absorbable suture and the skin with 6-0 silk suture.
Postoperatively all patients were treated with moxifloxacin 0.5% and tobramycin & fluoromethalone eye drops four times daily for 3 months. The silicone tube was removed at least after 3 months. The patients were followed up at the 1st week and 1, 3, 6 and 12 months. Success of revision of DCR surgery is defined by relief of epiphora, discharge postoperatively and patency of lacrimal passage by lacrimal sac syringing. Informed consent was taken from all patients. The Statistical analysis was carried out using SPSS statistical software package (Version 16.0; SPSS).
Observations and Results
The mean age was in group A 52.65 ± 11.55 and in group B 51.12 ± 12.45 years. There were 15 females and 10 males in group A. 12 females and 8 males in group B. In our study mostly patients were belong to age group 50-70 years. In group A 15 eyes were right and 10 eyes were left and in group B 8 eyes were right and 12 were left. Silicone tube was removed after 3 months in all patients. In our study we were found that in group A 23 patients had no complaints and 2 patients had develop epiphora after removal of silicone tube at 3rd month follow up. In group B 19 patients had no complaints and one patient developed epiphora at 6 month follow up after surgery. Overall success rate was 93.33% and failure rate was 6.67 %. In 4 patients (group A 2 and group B 2) Chronic nasal irritation and congestion was reported.
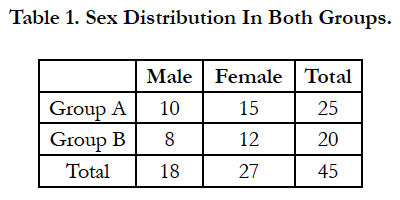

Table 1. Sex Distribution In Both Groups.
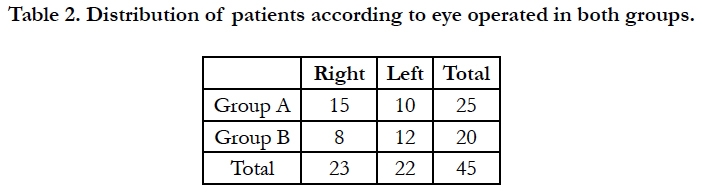
Table 2. Distribution of patients according to eye operated in both groups.
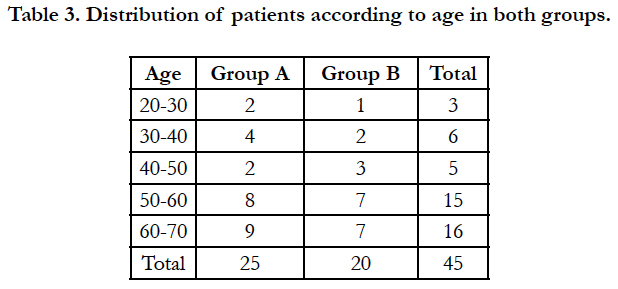
Table 3. Distribution of patients according to age in both groups.
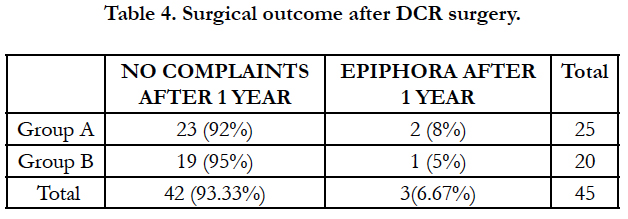
Table 4. Surgical outcome after DCR surgery.
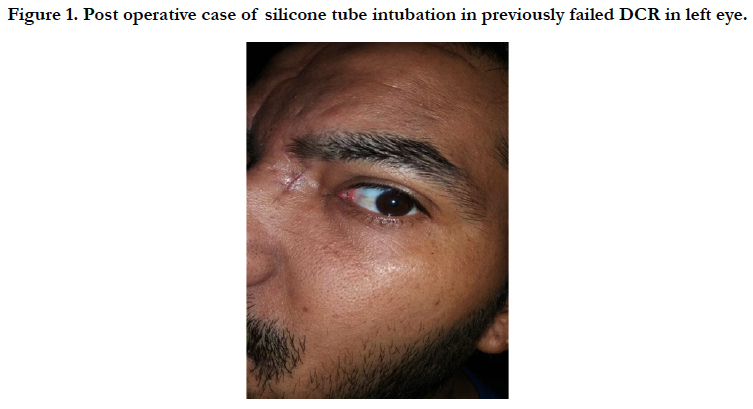

Figure 1. Post operative case of silicone tube intubation in previously failed DCR in left eye.
Discussion
In our study we have included 45 patients of failed DCR and divided into 2 groups: Group A and Group B. In group A patients were operated and silicone tube intubation was done. In group B patients were operated and silicone tube intubation was done along with mitomycin c application. In our study the total success rate was 93.33% . Failure rate was 6.67%.
Syed Ali Raza Rizvi et al., (2011) were included 50 patients of traumatic dacryocystitis and failed dacryocystorhinostomy in there study and concluded that Silicone Intubation is one of the most effective modality in dealing with such cases [7]. Imtiyaz A. Lone et al., (2004) were included forty patients of failed dcr and concluded DCR with silicone tube intubation has been accepted as a highly successful procedure in patients with history of epiphora and discharge following chronic dacryocystitis [8]. Shagufta Rather, Tejit Singh (2013) were included 200 patients in there study and concluded that use of silicone tube intubation in primary DCR surgery ,leads to high success rate [9]. Nam Ju Kim, MD et al., ( 2007) were included 13 patients who had persistent epiphora after an anatomically successful primary external DCR and concluded that Lacrimal silicone tube intubation is a simple safe and effective procedure for patients with epiphora even after anatomically successful DCR [10]. Praveen Subudhi et al., (2015) Were included 40 patients of failed DCR in there study and they performed dcr surgery with silicone tube intubation and concluded that Re DCR has high risk of osteotomy closure, hence this modified technique can be considered as an alternative to standard intubation technique with optimum results [11]. Emine Akcay et al (2016) were included 41 patients of failed DCR surgery in the study and concluded that the repeat external DCR procedure has high success rates for failed DCR surgeries, whichever procedure was performed [12]. Ji Sun Baek et al., (2017) were included 61 patients of failed endonasal DCR surgery and concluded that lacrimal silicone tube intubation is an effective treatment procedure for patients with functional epiphora [13].
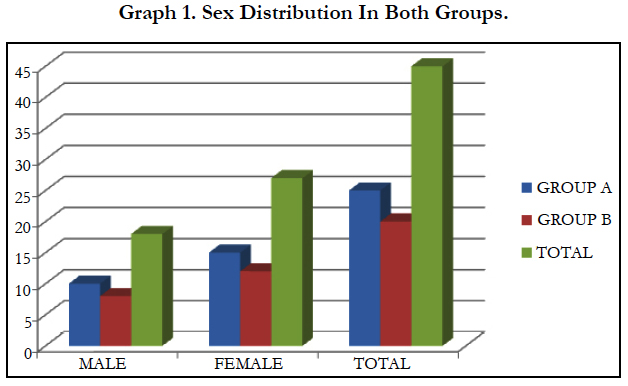
Graph 1. Sex Distribution In Both Groups.
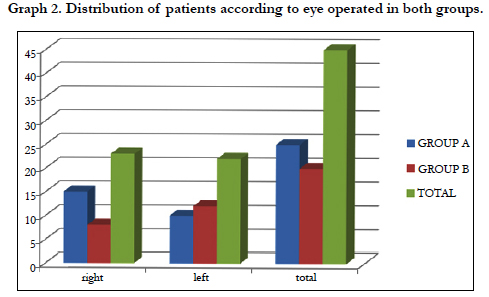
Graph 2. Distribution of patients according to eye operated in both groups.
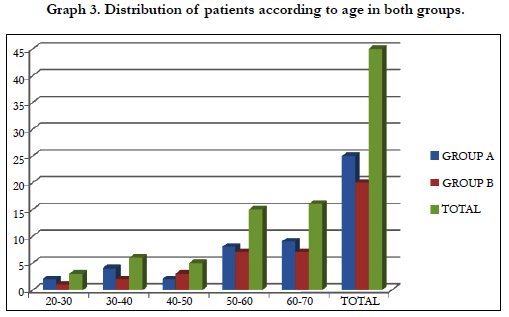
Graph 3. Distribution of patients according to age in both groups.
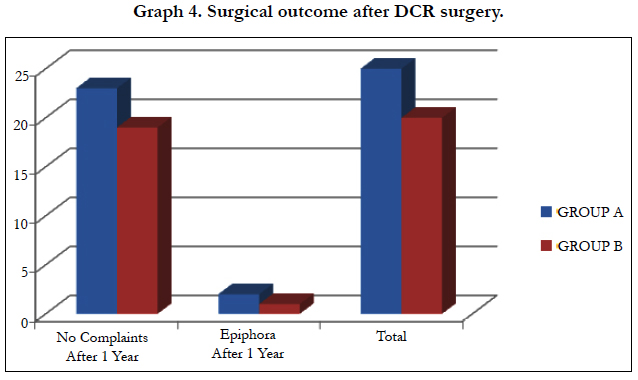
Graph 4. Surgical outcome after DCR surgery.
Conclusion
We concluded that revision of failed dcr surgery with silicone tube intubation and mitomycin c has good results. Mitomycin c can be used in selective cases in which excessive fibrosis and granulation tissue was found intraoperatively.
Acknowledgments
The completion of this study could not have been possible without the expertise of dr ankita shrivastav. We would also like to thanks dr. dimple shakeet for sitting on our panel and taking the time to read our article. Last but not the least, we would like to thank our parents our teachers and almighty god.
References
- Selig YK, Biesman BS, Rebeiz EE. Topical application of mitomycin-C in endoscopic dacryocystorhinostomy. Am J Rhinol. 2000 May-Jun;14(3):205-7. PubMed PMID: 10887629.
- Yildrim C , Yayali V, EsmeA, Ozden C. Long term result of adjunctive use of mitomycin C in external dacryocystorhinostomy. 2007 Feb;27(1):31-5. PubMed PMID: 17377748.
- DeAngelis D, Hurwitz J, Shinoff M. Lacrimal drainage system stenting with silicone tubing. Ophthal Plast Reconstr Surg. 2000 Jul;16(4):305-6. Pub- Med PMID: 10923981.
- Ajit Kulkarni ,S.Dadeya.Antimetabolites in pterygium surgery .March,2005 DOS Times – Vol. 10, No. 9
- Rahman A , Channa S, Niazi JH, Memon MS. Dacryocystorhinostomy without intubation with intraoperative mitomycin-C. J Coll Physicians Surg Pak. 2006 Jul;16(7):476-8. PubMed PMID: 16827960.
- Kao SC, Liao CL, Tseng JH, Chen MS, Hou PK. Dacryocystorhinostomy with intraoperative mitomycin-C. Ophthalmology. 1997 Jan;104(1):86-91. PubMed PMID: 9022109.
- Rizvi SA, Sharma SC, Tripathy S, Sharma S. Management of traumatic dacryocystitis and failed dacryocystorhinostomy using silicone lacrimal intubation set. Indian J Otolaryngol Head Neck Surg. 2011 Jul; 63(3): 264–268. PubMed Central PMCID: PMC3138957. doi: 10.1007/s12070-011-0230-x.
- Lone IA, Wahab A, Ahmad SS, Untoo RA. Repeat DCR with silicone tube intubation: A prospective study.
- Rather S, Singh T. External Dacryocystorhinostomy with & without Silicon Tube Intubation in Chronic Dacryocystitis with Nasolacrimal Duct Block.
- Kim NJ, Kim JH, Hwang SW, Choung HK, Lee YJ, Khwarg SI. Lacrimal Siicone Intubation for Anatomically Successful but Functionally Failed External Dacryocystorhinostomy . Korean J Ophthalmol. 2007 Jun;21(2):70-3. PubMed PMID: 17592235. PubMed Central PMCID: PMC2629706.
- Subudhi P, Datta D, Namperumalsamy P. External Repeat Dacryocystorhinostomy with Modified Silicone Intubation for Failed DCR: Analysis of Efficacy and Patient Tolerability. The Official Scientific Journal of Delhi Ophthalmological Society. 2015 Apr 13;25(4):242-5.
- Akcay E, Yuksel N, Ozen U. Revision External Dacryocystorhinostomy Results After a Failed Dacryocystorhinostomy Surgery. Ophthalmol Ther. 2016 Jun; 5(1): 75–80. PubMed Central PMCID: PMC4909675. doi:10.1007/s40123-016-00484.
- Baek JS, Jeong SH, Lee JH, Choi HS, Kim SJ, Jang JW.Cause and Management of patients With Failed Endonasal Dacryocystorhinostomy . Clin Exp Otorhinolaryngol. 2017 Mar;10(1):85-90. PubMed PMID: 27384034. PubMed Central PMCID: PMC5327589.





