Axenfeld Riger Syndrome with Dental Anomalies - Rare Developmental Anomaly
Vardhan N1*, Shivanjli B2, Sharma A3
1 Ophthalmology IGMC Shimla, Governmentt Hospital, Jubbal District, Shimla (H.P.), India.
2 GDC Shimla, India.
3 General Physician, Government Hospital, Jubbal District, Shimla (H.P.), India.
*Corresponding Author
Nishant vardhan MS,
Ophthalmology IGMC Shimla, Government Hospital,
Jubbal District, Shimla (H.P.), India.
Tel: 9418723653
E-mail: wardhan8@gmail.com
Received: December 11, 2016; Accepted: February 27, 2017; Published: February 28, 2017
Citation: Vardhan N, Shivanjli B, Sharma A (2017) Axenfeld Riger Syndrome with Dental Anomalies - Rare Developmental Anomaly. Int J Ophthalmol Eye Res. 5(2), 280-282. doi: dx.doi.org/10.19070/2332-290X-1700060
Copyright: Vardhan N© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This article reports an rare case of Axenfeld Rieger Syndrome (ARS) associated with dental anomalies. A 10 year old boy with ARS revealed interesting dental anomalies.
2.Introduction
3.Case Report
4.References
Keywords
Axenfeld Rieger Syndrome, Iris Hypoplasia; Dental Anomalies.
Introduction
Axenfeld–Rieger Syndrome (ARS) is an autosomal dominant genetic disorder and the incidence of ARS is estimated at 1 in 200,000 [1]. Sixty percent of cases have been linked to mutations in the transcription factors PITX2 (4q25), FOXc1 (6p25) and unidentified genes on 13q14, 16q24 and chromosome 11 [2]. Although cases with ARS show a wide spectrum of developmental defects, including ocular, umbilical, auricular, dental and craniofacial abnormalities; the ocular and craniofacial features are primary presentations of this syndrome [3]. Cardiovascular and endocrinological anomalies may also be seen.
ARS manifests with varying degrees of ocular anterior segment dysgenesis including heterochromia, aniridia, coloboma of the iris and persistent papillary membrane, corneal opacities [1, 4]. Craniofacial malformations include midface hypoplasia, hypertelorism, telecanthus, mandibular prognatism, hypodontia and microdontia. Cleft palate may also be found [1]. In this case report, a brief description of ARS with dental anomalies was presented.
Case Report
A 10 year old child presented with gradual painless diminution of vision right eye with intermittent headache. Ophthalmic evaluation showed visual acuity of 6/24 right and 6/6 left eye. On slit lamp examination iris hypoplasia detected in both eyes (Figure 1, 2). Schwalbe’s line was anteriorly displaced Figure 2). Intraocular pressures was 28 mmHg in the right eye and 16 mmHg in left eye. There was deep vertical cupping right eye with corresponding visual field defect (Figure 4, 5). OCT was done (Figure 6). Routine investigations including ECG an routine blood test were normal. Dental examination revealed hypodontia, oligodontia and anterior cross bite (Figure 7, 8). Based upon iris pattern, angle anomalies,- disc changes and dental anomalies provisional diagnosis of Axenfeld Rieger Syndrome (ARS) with secondary glaucoma was made. Patient was started antiglaucoma medication and called for follow up. On next visit patients IOP reduced to 16 mmHg both eyes. IOP was recorded weekly for a month and found to maintain at 14 mm Hg. The patient is now on monthly follow up.
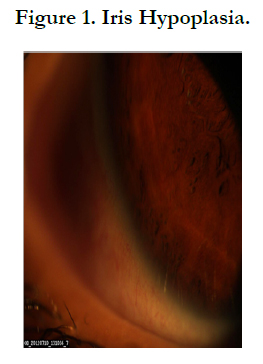

Figure 1. Iris Hypoplasia.
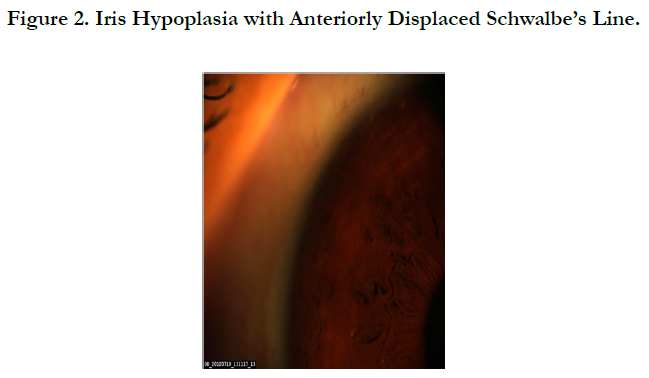

Figure 2. Iris Hypoplasia with Anteriorly Displaced Schwalbe’s Line.
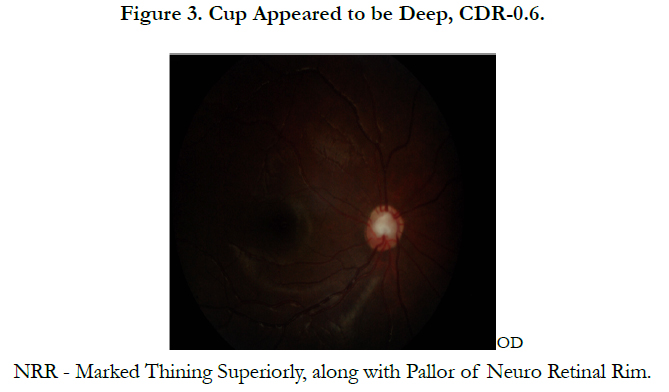
Figure 3. Cup Appeared to be Deep, CDR-0.6 NRR - Marked Thining Superiorly, along with Pallor of Neuro Retinal Rim.
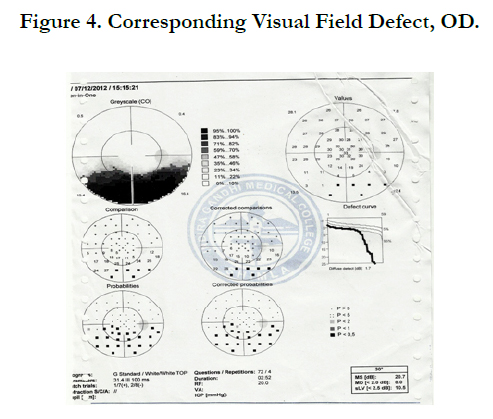

Figure 4. Corresponding Visual Field Defect, OD.
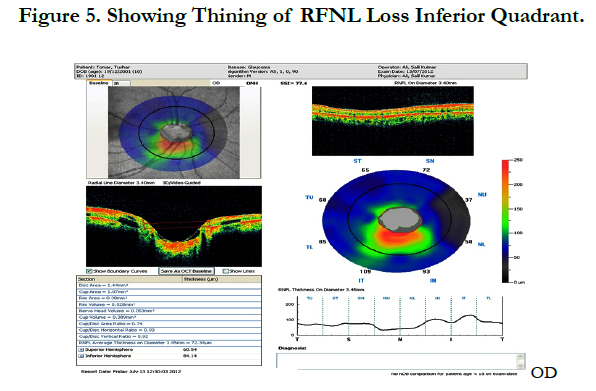
Figure 5. Showing Thining of RFNL Loss Inferior Quadrant.
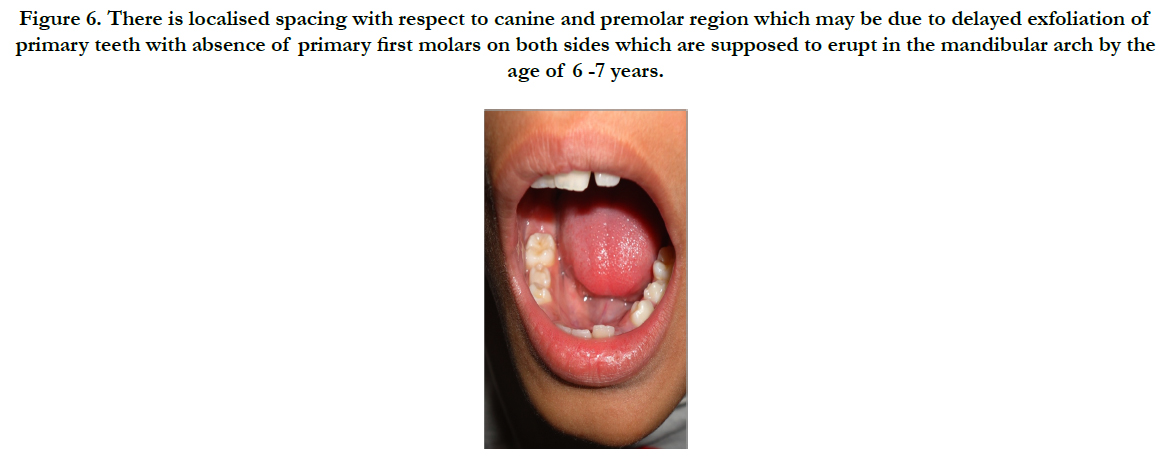

Figure 6. There is localised spacing with respect to canine and premolar region which may be due to delayed exfoliation of primary teeth with absence of primary first molars on both sides which are supposed to erupt in the mandibular arch by the age of 6 -7 years.
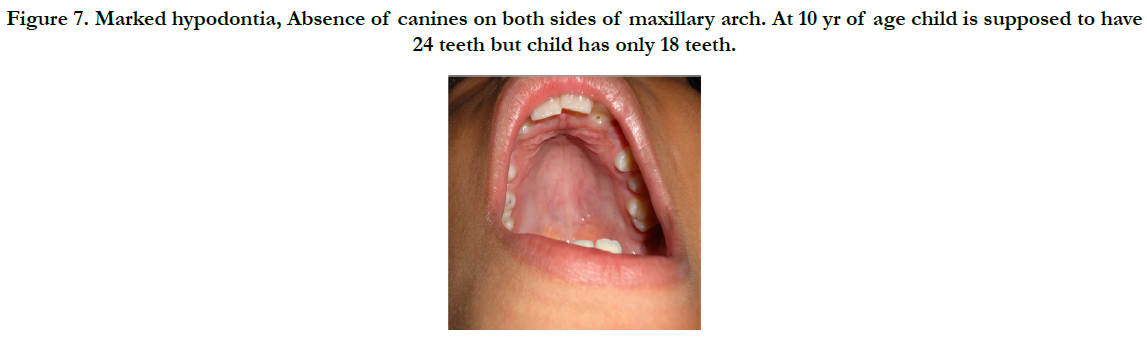

Figure 7. Marked hypodontia,Absence of canines on both sides of maxillary arch. At 10 yr of age child is supposed to have 24 teeth but child has only 18 teeth.
ARS is one of the ocular anterior segment dysgenesis syndromes [5, 7]. The pathogenesis is believed to be the impaired neural crest cell and ectodermal migration and differentiation during embryonic development [1, 8]. The ocular and systemic features of ARS including craniofacial, dental, abdominal abnormalities are well described in literature and multiple additional abnormalities have been reported in association with ARS, including sensorineural hearing loss and cardiac abnormalities [7]. As visual function can be preserved with early diagnosis, the knowledge of this presentation is important for the ARS patients. ARS is a multisystem disorder and a team approach including specialists in ophthalmology, oral surgery, cardiology and molecular genetics is necessary.
References
- Waldron JM, McNamara C, Hewson AR, McNamara CM (2010) Axenfeld Rieger syndrome (ARS): A review and case report. Spec Care Dentist. 30(5):218 22.
- Lines MA, Kozlowski K, Walter MA (2002) Molecular genetics of Axenfeld-Rieger malformations. Hum Mol Genet. 11(10): 1177-84.
- Li X, Venugopalan SR, Cao H, Pinho FO, Paine ML, et al., (2014) A model for the molecular underpinnings of tooth defects in Axenfeld Rieger syndrome. Hum Mol Genet. 23(1): 194 208.
- Chang TC, Summers CG, Schimmenti LA, Grajewski AL (2012) Axenfeld Rieger syndrome: New perspectives. Br J Ophthalmol. 96(3): 318 22.
- Dhir L, Frimpong Ansah K, Habib NE (2008) Missed case of Axenfeld Rieger syndrome: A case report. Cases J. 1: 299.
- Alward WL (2003) Axenfeld Rieger syndrome in the age of molecular genetics. Am J Ophthalmol. 130(1): 107 15.
- Gripp KW, Hopkins E, Jenny K, Thacker D, Salvin J (2013) Cardiac anomalies in Axenfeld Rieger syndrome due to a novel FOXC1 mutation. Am J Med Genet A. 161A(1): 114 9.
- Ma J, Zhong Y, Zhao C, Zhang X, Sui R, et al., (2011) Axenfeld Rieger syndrome in monozygotic twins. J Glaucoma. 20(9): 584 6.





