Climatic Keratopathy in Snow Laden Hilly Areas
Sood T1*, Sharma RL2, Mandeep T3, Sood S4, Sharma A5
1 Eye Surgeon, Civil Hospital Sarkaghat, Himachal Pardesh, India.
2 Associate Professor, Department Of Ophthalmology, IGMC Shimla, Himachal Pardesh, India.
3 Registrar, Department of Ophthalmology, IGMC Shimla, Himachal Pardesh, India.
4 JP Eye Hospital, Mohali, Chandigarh, India.
5 Dermatology, Zonal Hospital ,Bilaspur, Himachal Pardesh, India.
*Corresponding Author
Dr. Tarun Sood Mbbs, M.s.ophthalmology (Igmc Shimla)
Eye Surgeon, Civil Hospital Sarkaghat, Himachal Pardesh, India.
Tel: 9418644853
E-mail: tarunsood_86@yahoo.co.in
Received: April 26, 2016; Accepted: June 06, 2016; Published: June 08, 2016
Citation: Sood T, Sharma RL, Mandeep T, Sood S, Sharma A (2016) Climatic Keratopathy in Snow Laden Hilly Areas. Int J Ophthalmol Eye Res. 4(5), 212-214.DOI : dx.doi.org/10.19070/2332-290X-1500043
Copyright : Sood T© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Spheroidal degeneration, reported as a rare entity in western literature is a common ocular morbidity in some parts of India. It is commonly seen in persons who are exposed to intense sun light (excess UV radiation) reflected off the surface of the sea, snow and sand. The State of Himachal Pradesh lies in the northern part of India. Himachal Pradesh occupies an area of 55,673 sq km. It forms a key and central part of the Indian Himalayan region (IHR). The IHR region covers vast areas, with about 17 percent of the region being under permanent snow cover and glaciers and about 30-40 percent under seasonal snow cover, forming a unique water reservoir. High level of UV radiation reflected from snow have been implicated in pathology of spheroidal degeneration which may be one of reasons that prevalence of spheroidal degeneration is more in snowy areas of himachal. The author tends to report a case series of few cases of spheroidal degeneration.
2.Conclusion
3.References
Introduction
Spheroidal degeneration of cornea has been classified into Primary and Secondary forms. Primary spheroidal degeneration occurs as an aging process in an otherwise normal eye. Secondary spheroidal degeneration occurs in eyes with other ocular pathology such as phthisis bulbi, absolute glaucoma, corneal scars, chronic uveitis etc.,[1].
Clinically, spherules appear either in the form of smooth, fine gelatinous dew drops or yellowish or amber coloured raised globules with irregular surface [2]. The globular deposits are amorphous and predominantly acidophilic in nature and vary considerably in size (1µ - 100 µ) [3].
Depending on the size and depth of the spherules, spheroidal degeneration can be classified into 4 grades [4].
Tiny, microscopic oil droplet like lesions in the interpalpebral area, nasally and temporally near limbus, best seen by retro illuminaton.
Fine granular lesions in the interpalpebral area. Cornea appears ground glass. Lesions extend up to Bowman’s membrane. Lesions are seen with corneal loupe.
Amber coloured spherical nodules, raised above the surface of the cornea, occupying the peripheral or central cornea. Confluent lesions in the central part causes diminution of vision.
Spherules are associated with thinning and opacification of the superficial cornea. Gross visual deterioration occurs in this stage. Such patients are liable to get indolent corneal ulcers [4].
Chemical composition of the spherules is not exactly known. It could be hyaline, colloid, a protein high in tyrosine, lipids elastin or keratin in incomplete form [5].
First described in 1955 by Bietti as Bietti nodular hyaline band shaped keratopathy. Basing on the clinical appearance or the geographical location or population groups in which the cases were identified, different authors have given different names to this condition i.e Climatic droplet keratopathy, Spheroidal droplet degeneration (Fraunfelder and associates), Fisherman’s keratopathy (Dr. R.Suryaprasada rao 1961), Labrador keratopathy (Freedmann and Rodger-1965), Nama keratopathy from South Africa (Freedman), Eskimo’s keratopathy etc., but Spheroidal degeneration (Fraunfelder and Hanna) is the most commonly used term to describe all the related lesions [6].
Clinically, it is characterised by the presence of amber coloured spherules on the cornea giving rise to intense foreign body sensation, pain, redness, watering, photophobia and decreased visual acuity. Because of the poor ocular surface they are not suitable for certain other ocular procedures like refractive status assessment, cataract surgery etc thus decreasing their quality of life [7]. All these in turn result in gross decrease in the Quality of life of the patient. Intense sunshine, excess UV radiation, microtrauma due to wind borne particles, extremes of high or low temperature, aridity, malnutrition and genetic factors are incriminated as the etiological factors for the development of spheroidal degeneration.
The Author Tends to Report Few Cases of Spheroidal Degeneration Reported at Eye OPD.
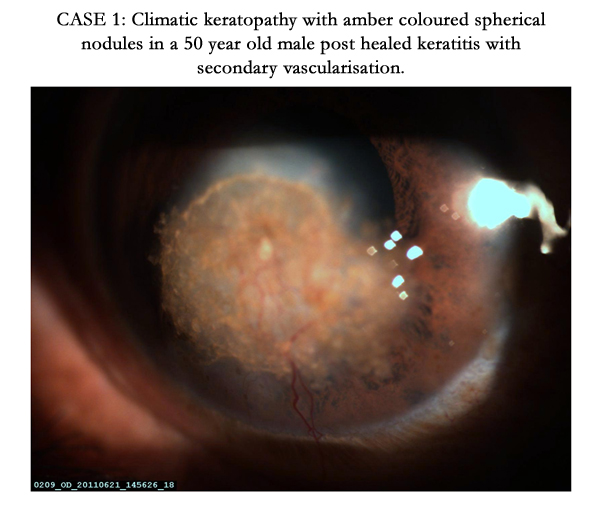
CASE 1: Climatic keratopathy with amber coloured spherical nodules in a 50 year old male post healed keratitis with secondary vascularisation.
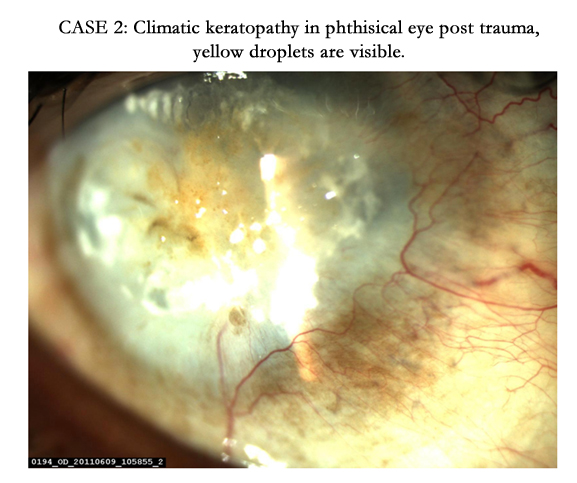

CASE 2: Climatic keratopathy in phthisical eye post trauma, yellow droplets are visible.
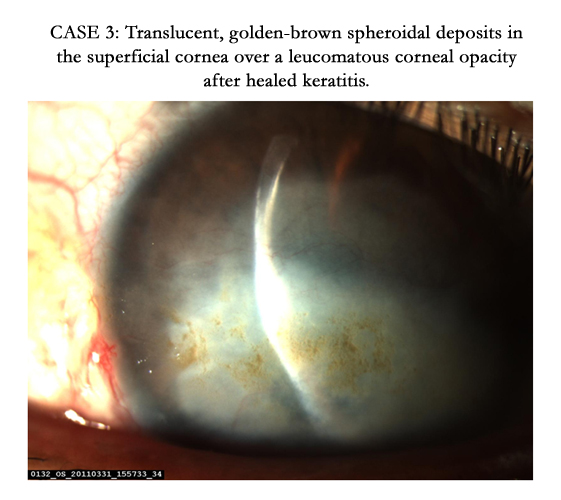

CASE 3: Translucent, golden-brown spheroidal deposits in the superficial cornea over a leucomatous corneal opacity after healed keratitis.
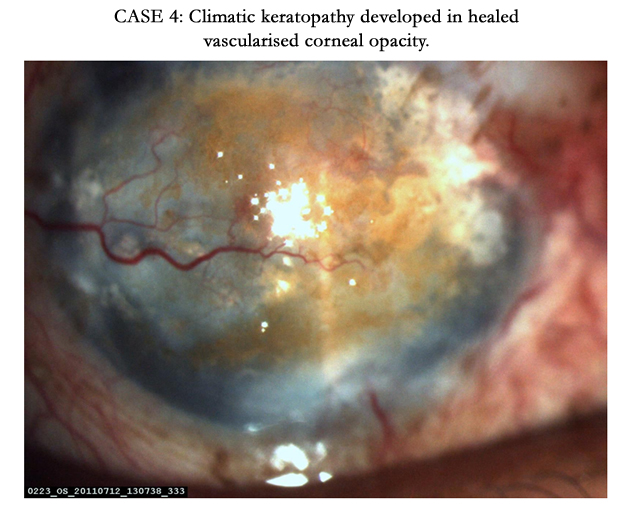

CASE 4: Climatic keratopathy developed in healed vascularised corneal opacity.
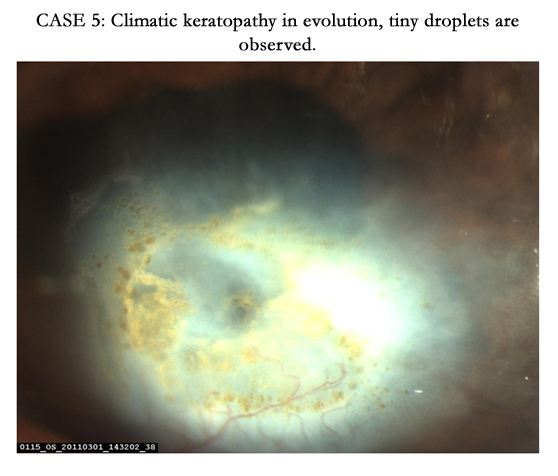

CASE 5: Climatic keratopathy in evolution, tiny droplets are observed.
UVR carries higher energy than visible light, and its effects on tissues include DNA damage, gene mutations, immunosuppression, oxidative stress and inflammatory responses. In the eye, UVR is strongly associated with the development of basal and squamous cell carcinoma of the eyelid, pterygium, photokeratitis, climatic droplet keratopathy, ocular surface squamous neoplasia, cataracts, and uveal melanoma, and is weakly associated with age-related macular degeneration [8].
CDK is associated with chronic UV-A and UV-B exposure. A high prevalence has been reported in geographical areas with high levels of UV exposure. CDK is very highly correlated with chronic UVR exposure. CDK is a spheroidal degeneration of the superficial corneal stroma. Translucent material accumulates in the superficial corneal stroma within the interpalpebral strip, beginning peripherally and spreading centrally. In young subjects, the deposits appear in narrow bands close to the limbus nasally and temporally symmetrically in both eyes; with time and continued exposure, they accumulate over the visual axis and form a complete band. In the most advanced stages, raised nodules develop that are yellow-brown in color.
Cornea is naturally shielded from direct solar rays by brow ridge for this reason photokeratitis occurs during walking on snow. This effect is aggravated by looking down towards the ground while walking which causes the reflected UV radiation to strike cornea directly and not obliquely. In this position corneal UV-B irradiance from snow is as heavy as 10 percent of direct solar UV-B irradiance. oblique angles of incident radiations are not
absorbed nearly as effectively as direct incident radiation due to angular dependence of Fresnel reflection [9].
The management options include superficial keratectomy (manual or laser), with or without amniotic membrane grafts,
lamellar keratoplasty or penetrating keratoplasty may be required for deeper involvement.
Conclusion
Despite overwhelming evidence regarding the deleterious effects on UVR, public health measures to encourage UV protection of the eyes is generally lacking. Options for photoprotection include sunglasses, wide brim hats, windshields, plastic films for side windows in cars, UV blocking contact lenses. High level of UV radiation reflected from snow have been implicated in pathology of spheroidal degeneration which may be one of reasons that prevalence of spheroidal degeneration is more in snowy areas of himachal.
References
- FT Fraunfelder MD, Calvin Hanna PhD, And J. Parker MD (1973) Spheroid Degeneration Of The Cornea And Conjunctiva. Clinical Course And Characteristics. Am J O 76: 821-828.
- Varsha M Rathi, Sharadini P Vyas, Virender S Sangwan (2012) Phototherapeutic Keratectomy. Ijo 60(1): 5-14.
- Daljit Singh, Mohindar Singh, Shiv Inder Singh Rudra (1979) Climatic Keratopathy.Ijo 27(4): 180-184.
- Sridhar Ms, Garg P, Das S, Vemuganti G, Gopinathan U, Rao GN (2000) Infectious Keratitis In Climatic Droplet Keratopathy. Cornea 19(4): 455-458.
- Fraunfelder FT, Hanna C, Cable M, Hardberger RE (1973) Entrapment of ophthalmic ointment in the cornea. Am J Ophthalmol 76(4): 475-484.
- Alec Garner (1970) Keratinoid Corneal Degeneration.Bjo 54: 769-780.
- T Hida, K Kigasawa, E Tanaka, S Akiya, Y Tashiro and Y Hosoda. Primary Band Shaped Spheroidal 70(5): 347-353.
- H Sliney, J Mellerio. (1980) DSafety with Lasers and Other Optical Sources: A Comprehensive Handbook. (1st edtn), Springer US, USA.
- Mercede Majdi 1,*, Behrad Y. Milani 1,†, Asadolah Movahedan 1,†, Lisa Wasielewski 2,†, Ali R. Djalilian 1 (2014) The Role of Ultraviolet Radiation in the Ocular System of Mammals. Photonics 1(4): 347-368; doi:10.3390/photonics1040347.





