To Study the Association of HbA1c with Retinopathy, Neuropathy and High Risk Foot among Diabetic Patients Attending Rural Tertiary Care Hospital of Tamil Nadu, India
Kamran M Hassan1*, Balaji R2, Gnaneswaran S3, Kumar JS4
1 Assistant Professor, Department of Ophthalmology, SRM Medical College Hospital & Research Centre, Kattankulatur, Chennai, Tamilnadu, India.
2 Assistant Professor, Department of Community Medicine, SRM Medical College Hospital & Research Centre, Kattankulatur, Chennai, Tamilnadu,
India.
3 Professor, Department of Ophthalmology, SRM Medical College Hospital & Research Centre, Kattankulatur, Chennai, Tamilnadu, India.
4 Professor, Department of General Medicine, SRM Medical College Hospital & Research Centre, Kattankulatur, Chennai, Tamilnadu, India.
*Corresponding Author
Kamran M Hassan,
Assistant Professor, Department of Ophthalmology, SRM Medical College Hospital & Research Centre,
Kattankulatur, Chennai, Tamilnadu – 603203, India.
Tel: +91-9176498590
E-mail: dr.kamranhassan@gmail.com
Received: April 22, 2016; Accepted: May 28, 2016; Published: May 31, 2016
Citation: Kamran M Hassan, Balaji R, Gnaneswaran S, Kumar JS (2016) To Study the Association of HbA1C with Retinopathy, Neuropathy and High risk foot among Diabetic patients attending Rural Tertiary Care Hospital of Tamil Nadu, India. Int J Ophthalmol Eye Res. 4(4), 206-211.DOI : dx.doi.org/10.19070/2332-290X-1500042
Copyright : Kamran M Hassan© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Blindness and non-traumatic amputation of foot are among the biggest morbidities complicating diabetes mellitus. Burden of diabetes and its complications is increasing in India. The current study was designed to find out the association of HbA1C with these diabetic microvascular complications i.e., neuropathy leading to high risk diabetic foot and retinopathy.
Materials and Methods: This is a cross sectional analytical study. 222 patients were examined with established Diabetes between ages 27 to 85 years, who visited the hospital from June 2012 to October 2014. Assessment of retinopathy, neuropathy and HbA1c was done by standardised methods. The obtained data was analysed statistically by SPSS version of 21.0.
Results: The mean age of the study population was 55.4 ± 11.1 years (range 27-85 years). There were 145 (65.32%) males and 77 (34.68%) were females. The mean level of HbA1c was 8.6 ± 2.1%. Patients with HbA1c >7% included 107 males and 55 females. The prevalence of DR in our study was 49.10% of which NPDR was seen in 38.29% and PDR was seen in 10.81% of patients. The prevalence of neuropathy was seen in 62 (27.93%) patients. The condition of footwear was poor in 32.5%.
Conclusion: A strong association was found between HbA1C and neuropathy leading to high risk diabetic foot and retinopathy. These associations suggest the need for earlier diagnosis of these devastating complications and predicting their severity.
2.Introduction
3.Materials and Methods
3.1.Inclusion criteria
3.2.Exclusion criteria
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Diabetes Mellitus; Retinopathy; Neuropathy; High Risk Foot; HbA1c; Health Care Education.
Introduction
Globally at present, there are an estimated 366 million people affected with diabetes mellitus. The Indian figure is around 61.3 million diabetics, which is projected to cross 100 million by the year 2030 [1]. Owing to rise of diabetes mellitus cases, the economic burden due to diabetes in India ranks the highest in the world [2]. With the increasing prevalence of diabetes, it has resulted in an increase in its complications which has resulted in increasing morbidity, mortality and health expenditure due to the requirement of specialized care [1].
Blindness and non traumatic amputation of foot are among the biggest morbidities complicating diabetes mellitus [3]. The annual incidence of foot ulcers is as high as 2% but the lifetime risk of a person with diabetes developing a foot ulcer may be as high as 25% [4]. Studies have shown that 40% to 85% of amputations among persons with diabetes can be prevented with a team approach. Therefore, the identification of an increased risk for ulceration is of importance for amputation prevention [5].
Organizations, such as the International Diabetes Federation and the World Health Organization, have set goals to reduce the rate of amputations by up to 50% [6].
Diabetic retinopathy which leads to blindness has the potential treatability with laser photocoagulation when detected early. Studies have shown the occurrence of clinical neuropathy to be correlated with presence of retinopathy, arterial hypertension and microangiopathy. The exact pathophysiology of diabetic peripheral neuropathy (DPN) has not been well understood but association with microvascular disease like retinopathy might be implicated in its cause [7].
The recent recommendation for diagnosis of Diabetes Mellitus, as has been stated by American Diabetes Association in the position statement of 2014, that HbA1c has now been included in the diagnosis of diabetes. The HbA1c value of ≥6.5% is sufficient to make diagnosis [8].
In epidemiological analyses, HbA1C levels > 7.0% are associated with a significantly increased risk of both microvascular and macrovascular complications, irrespective of underlying treatment [9]. Inferences from the United Kingdom Prospective Diabetes Study have shown that proper control of blood glucose through diet, exercise and medications prevents the development of microvascular complications [1].
Therefore, on the basis of research literatures mentioned above, the current study was designed to find out the association with HbA1c with these diabetic microvascular complications i.e., neuropathy leading to high risk diabetic foot and retinopathy.
Furthermore, finding such an association may also be helpful in earlier diagnosis of the devastating complications and prediction of severity of them.
Materials and Methods
This is a cross sectional analytical study of patients who visited Ophthalmology department and Diabetology OPD of SRM MCH & RC, a tertiary care hospital, for their routine checkup. A two hundred and twenty two (222) patients were examined (a total of 444 eyes of 222 consecutive patients with established Diabetes) between ages 27 to 85 years, who visited the above departments from June 2012 to October 2014, were selected for the study. The patients represent the general population of the urban and rural area. Following informed consent, all patients were enrolled sequentially. An approval was obtained from the institutional ethics committee.
Study participants were given a physical examination and interviewed for exposure variables, including demographic data, literacy status, medical, surgical, and social history. Diabetes and diabetes-related complication history were noted, visual acuity for each eye was recorded with the best possible correction using Snellen’s projection chart and detailed ocular exam done. Further examination included, lower extremity neuropathy exam, any history of foot ulcer or amputation, musculoskeletal abnormality, foot deformity and condition of the footwear noted.
In this study, only those patients were included, who were known diabetics. New cases of type-2 diabetes were also included because they might have complications at the time of diagnosis because of the nature of disease. For type-1 diabetics, only those patients were selected who have duration of diabetes of more than five years, because in type-1 diabetics complications usually starts after five years of duration, in accordance to the criteria of American Diabetes Association [10].
Patients with type-1 diabetes less than 25 years of age were excluded from this study along with those patients having Gestational diabetes. Patients with mature cataracts and hazy media, whose fundus could not be examined were excluded. Patients with a history of exposure to radiation, hypertensive retinopathy without DM, sickle cell disease, co–existing vascular retinopathies and pheochromocytoma were also excluded, as these conditions could mimic fundus features with diabetic retinopathy. Also patients with history of retinal photocoagulation, intravitreal anti-VEGF injections and any intra ocular surgeries were excluded.
After taking a detailed history, a routine ophthalmological examination was done .The fundus was examined , after pupillary dilation with 1% Tropicamide eye drops a mydiatric agent , with +90D Volk lens & slit lamp bio-microscope, and subsequently taken for fundus photography using computerized digital fundus photography camera.
Findings were noted and patients were categorized according to findings, whether diabetic retinopathy was present or absent. If present, retinopathy was classified according to ICDRDS [11].
All the cases with DR were explained about their ocular status and treatment was given at concession rates. DM patients with blindness or low vision disability and those with high risk foot were referred for rehabilitative services.
Retinopathy was graded as: Within Normal Limits (WNL), Non- Proliferative Diabetic Retinopathy (NPDR), or Proliferative Diabetic Retinopathy (PDR), with or without diabetic macular edema, according to International Clinical Diabetic Retinopathy Disease Severity Scale [11].
All patients with diabetes were screened for DPN by examining pinprick, temperature, and vibration perception (using a 128-Hz tuning fork), 10-g monofilament pressure sensation at the distal halluces, and ankle reflexes. Combinations of more than one test have 87% sensitivity in detecting DPN. Loss of 10-g monofilament perception and reduced vibration perception have predicted foot ulcers [12].
The feet were also examined for any other risk factors for ulcers like calluses, very dry skin, previous ulcerations or amputations and deformities, and footwear condition was also inspected and taken as high risk feet. As longitudinal studies have shown that a simple clinical examination is a good predictor of future foot ulcer risk [12].
The above methodology for screening and examination was based on risk classification system of the International Working Group on the Diabetic Foot (IWGDF) [13].
Epidemiologic data has shown a relationship between HbA1c and the risk of retinopathy similar to that which has been shown for corresponding FPG (fasting plasma glucose) and 2-hPG (2 hour post glucose) thresholds. HbA1c assay was done in the laboratory using a method that is NGSP certified and standardized to the DCCT assay [3].
Furthermore, HbA1c is an indicator of the average blood glucose concentrations over the preceding 2–3 months and is currently considered the best index of metabolic control in individuals with diabetes. The DCCT and UKPDS study have demonstrated that lowering HbA1c can reduce the risk of diabetes microvascular complications [14]. Also by International Federation of Clinical Chemists (IFCC) standards, HbA1c is now being considered for diagnostic and screening purposes. HbA1c does not need to be measured in a fasting state or with a glucose load and therefore
offers potential ease and convenience [3].
All data were analyzed using statistical software package SPSS version 21.0. Variables of interest, i.e., neuropathy, high risk foot, retinopathy status and HbA1c values were summarised using descriptive statistics. For categorical variables, frequencies and percentages were used and for continuous variables, mean and standard deviation were used. Box plots were used to show the relation between HbA1c with vibration perception, neuropathy status, high risk foot and retinopathy. Inferential statistics such as Chi-square test was used to show the relation between two variables, e.g., HbA1c and retinopathy.
Results
A total of 222 patients were included in the study. The mean age of the study population was 55.4 ± 11.1 years (range 27-85 years). There were 145 (65.32%) males and 77 (34.68%) were females. Mean duration of diabetes mellitus was 11.6 ± 6.42 years (range 1-28 years). The mean level of HbA1c was 8.6 ± 2.1%. Patients with HbA1c > 7% included 107 males and 55 females. It was observed in our study that 82.3% patients were literate and 17.7% were illiterate. The condition of footwear was poor in 32.5% and rest 67.5% patients had good conditioned footwear (Table 2).
Out of 222 patients, 109 (49.10%) had features of DR while 113 (50.90%) patients had a normal fundus. Amongst 109 patients with DR, 69 (63.30%) were males and 40 (36.70%) were females. The prevalence of DR in our study was 49.10% of which NPDR was seen in 38.29% and PDR was seen in 10.81% of patients. Diabetic macular edema was seen in 7.2%. (Table 3).
Male patients with retinopathy accounted 69 ( NPDR =50, PDR =19). As can be seen high prevalence of DR in Males co-relates with high HbA1c (>7%) in Males.
There was no evidence of neuropathy in 160 (72.07%) patients while 62 (27.93%) patients had features of neuropathy (Table 4).
The results regarding SPSS analysis for obtaining the relationship of HbA1c with neuropathy, associated sensory problems and retinopathy have been presented in box plots as Figure-1a to 1d. According to these results the level of HbA1c was significantly higher with non-proliferative retinopathies & high risk foot but very high with proliferative diabetic retinopathy, loss of vibration perception and neuropathy.
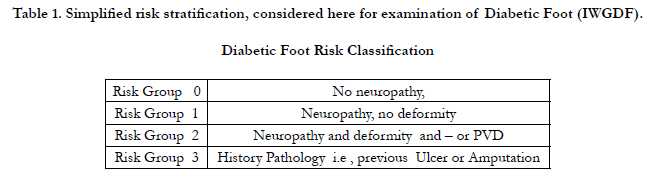

Table 1. Simplified risk stratification, considered here for examination of Diabetic Foot (IWGDF).
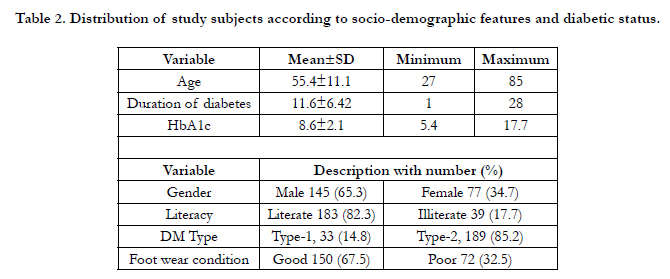
Table 2. Distribution of study subjects according to socio-demographic features and diabetic status.
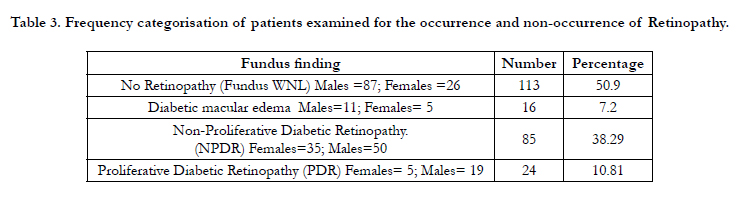
Table 3. Frequency categorisation of patients examined for the occurrence and non-occurrence of Retinopathy.
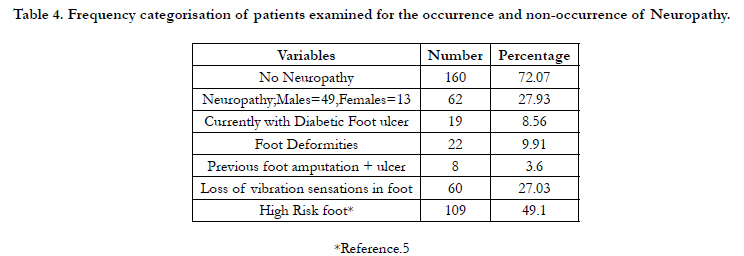
Table 4. Frequency categorisation of patients examined for the occurrence and non-occurrence of Neuropathy.
Discussion
The Diabetic retinopathy (DR) prevalence in our study was 49.10%. In the study by Giri et al [15] a hospital based study, the prevalence of diabetic retinopathy was 44.4%, which was comparable to our study. Other studies have shown DR prevalence in different geographic region as 55% in Yemen and 64.1% in Jordan as per Bamashmus et al [16]. The observed population variations in the prevalence of diabetic retinopathy could be due to genetic or due to poor control of diabetes and influence of socio-economic and cultural factors.
Whereas population based study CURES [2] have shown much lower DR prevalence rates. The reason for higher DR prevalence in our study could be because of patients who were already known Diabetics and who presented to the hospital directly were included in the study.
The DPN prevalence was comparable to Pradeepa et al [2] a population based study which showed prevalence of 26.1%. While in our clinical based study DPN was 27.93%, Ramachandran et al [17] a clinical based study also showed a similar prevalence (27.5%) of DPN. Dyck et al [18] study has shown that type 1 diabetes, DPN and retinopathy related to poor glycemic control. The EURODIAB study reported higher cumulative incidence of neuropathy related to higher HbA1c value [19,20]. Our study showed similar findings as in Figure 1b.
Mean age of the patients in our study was 55.4 ± 11.1 years and that of Giri et al [15] was 58.24 ± 13.76 years. The mean age of patients with DR was 54.4 ± 11.8 yrs in Bamashmus et al [16]. In our study males were more affected. Similar finding was seen in the study of Khandekar et al [21]. The reason for the sex predilection remains unclear and needs further investigation.
The mean HbA1c in our study was 8.6 ± 2.1, comparable to that of the Diabcare–Asia study which had mean HbA1c of 8.9 ± 2.1%, which was higher than the levels recommended by the American Diabetes Association and the ICMR guidelines in India [2]. Our study was also comparable to Agrawal et al [22], who demonstrated that poor glycemic control (HbA1c > 8%) was significantly associated with neuropathy and retinopathy. Comparable trend was seen in the mean HbA1c in other regions (South Asian) i.e, mean HbA1c of 8.9% in India, mean HbA1c of 9.1% in Pakistan and Sri Lanka showed mean HbA1c of 8.89%. These South Asian data have demonstrated poor glycemic control to be associated with the diabetes complications [23].
Higher HbA1c levels, around 9 or more, have definitely developed one or more of the microvascular diabetic complications as in Fig 1, a-d. But, those patients who were having average HbA1c levels of 7 or less; they are within normal limits or have not yet developed retinopathy or neuropathy, when examined in the current study , in accordance with ADA’s expected results for DM complications prevention [8].
Studies have shown that graded severity of retinopathy is strongly associated with severity of DPN [18]. Our study also had similar trend as shown in Figure 1, a-d. Therefore it is suggested that patients with PDR referred to neurologist should have complete neurologic examination to exclude DPN as it is a pivotal risk factor for both amputation and ulceration in persons with diabetes mellitus [5].
Therefore, it is suggested on the basis of results of the present study that the risk stratification should be followed (Table-1), while examining the diabetic patient with or without foot ulceration. According to results shown in Table-2, 17.7% of the patients were illiterate and their footwear or shoes were inappropriate which accounts to be 32.5%, being significant. The poor footwear, neuropathic foot & ulceration and higher HbA1c levels are interlinked in terms for pathogenesis to develop again and again. This can be prevented at least by educating the patient at diabetic educator clinic and diabetic foot clinic, and regular foot examination by health care professional.
Those patients whose HbA1c was around 9 or more, have definitely developed one of the chronic complications as has been shown by the results in the present study. The most important aspect of this study was to determine the association between the diabetic complications i.e., the high risk foot and the development of the progressive retinopathy which was found to be highly significant.
One of the inferences from the present study is that, diabetic patients with high HbA1c levels who have developed retinopathy with visual loss, cannot well examine their feet daily and are dependent on other persons at home. It should also be noted that visual impairment is one of the risk factors for the development of diabetic foot ulcer. Therefore, diabetic patients at risk for foot lesions and their relatives must be educated about risk factors and the importance of foot care [3].
Also there is a need for multidisciplinary team including the diabetologist, the Podiatrist, the vascular surgeon, the radiologist, ophthalmologist and the infectious disease specialist for better management and care for diabetic patients. The study by Malone et al have shown and emphasized the implementation of a multidisciplinary diabetic foot team [24].
In the presence of diabetic neuropathy, footwear can play a critical role in the pathogenesis of foot complications. Therefore, before choosing suitable footwear and insoles for such people, their lifestyle should also be taken into account, especially with regard to their level of activity [25].
In other words, to prevent the complications, the blood sugars should be controlled to the target levels as recommended by American Diabetes Association and other associations as well. Lowering HbA1c to below or around 7% has been shown to reduce microvascular and neuropathic complications of type-1 and type-2 diabetes [16].
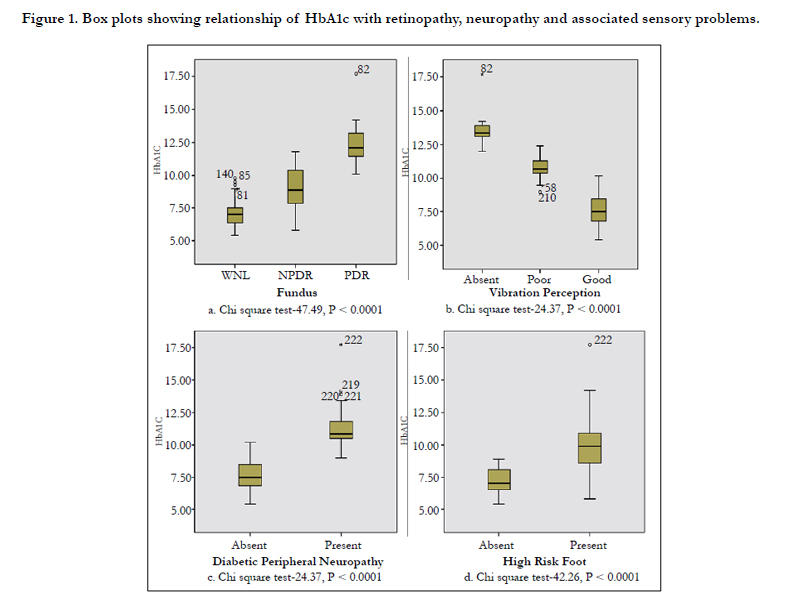
Figure 1. Box plots showing relationship of HbA1c with retinopathy, neuropathy and associated sensory problems.
Conclusion
A strong association was found between HbA1c and diabetic microvascular complications i.e., neuropathy leading to high risk diabetic foot and retinopathy. These associations suggest the need for earlier diagnosis of these devastating complications and predicting their severity.
For proper planning of a public health program, evidencebased information is crucial. Our study although hospital-based, provided information that would be useful for the Prevention of Blindness program of this region, as well as for proper combined screening for DPN patients in relation to HbA1c. The limitation of this study includes a limited sample of patients visiting one institution which could have introduced health-seeking bias.
References
- Saurabh S, Sarkar S, Selvaraj K, Kar SS, Kumar SG, et al., (2014) Effectiveness of foot care education among people with type 2 diabetes in rural Puducherry, India. Indian J Endocr Metab, 18(1): 106-10.
- Joshi SR, Das AK, Vijay VJ, Mohan V (2008) Challenges in Diabetes Care in India: Sheer Numbers, Lack of Awareness and Inadequate Control. J Assoc Physicians India 56(6): 443-50.
- Aziz KMA (2010) Association between High risk foot, Retinopathy andHbA1c in a Saudi diabetic population. Pak J Physiol 6(2): 22-28. pps.org.pk/PJP/6-2/Kamran.pdf
- Arad Y, Fonesca V, Peters A, Vinik A (2011) Beyond the Monofilament forthe Insensate Diabetic Foot: A systematic review of randomized trials to prevent the occurrence of plantar foot ulcers in patients with diabetes. Diabetes Care 34:1041-46.
- Lavery LA, Armstrong DG, Vela SA, Quebedeaux TL, Fleischli JG (1998) Practical Criteria for Screening Patients at High Risk for Diabetic Foot Ulceration. Arch Intern Med 158(2): 157-62.
- Bakker K, Apelqvist J, Schaper NC (2012) Practical guidelines on the management and prevention of the diabetic foot 2011. Diabetes Metab Res Rev 28(1): 225–31.
- Abdollahi A, Moghimi S, Tabasi A, Rajabi MT, Sabet B (2009) Neuropathy and retinopathy in diabetes: Is there any association. Int J Ophthalmol 2(1): 57-60.
- American Diabetes Association (ADA) 2014 Guidelines: Standards of medical care in diabetes. Diabetes Care 37(suppl 1): S14-S80.
- Imran AS, Rabasa-Lhoret R,Ross S (2013) Targets for Glycemic Control:Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Can J Diabetes 37(1): S31-S34.
- American Diabetes Association (ADA) 2008 Standards of medical care in diabetes (Position Statement). Diabetes Care 31(Suppl. 1): S12–S54.
- Wilkinson CP, Ferris FL, Klein RE, Lee PP, Agardh CD, Davis M, et al (2003) Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 110(9): 1677-1682.
- Boulton AJM, Vinik AI, AREZZO JC, Bril V, Feldman EL, Freeman ER, et al (2005) Diabetic Neuropathies: A statement by the American Diabetes Association. Diabetes Care 28(4): 956-962.
- Peters EJ, Lavery LA (2001) Effectiveness of the diabetic foot risk classification system of the International Working Group on the Diabetic Foot. Diabetes Care 24(8):1442–1447.
- Mohan V, Vijaychandrika V, Gokulakrishnan K, Anjana RM, Ganesan A, Weber MB et al (2010) A1C Cut Points to Define Various Glucose Intolerance Groups in Asian Indians. Diabetes Care 33(3): 515–519.
- Giri PA, Bangal SV, Phalke DB (2012) Prevalence of diabetic retinopathy and associated risk factors among diabetic patients attending Pravara Rural Hospital, Loni, Maharashtra. Journal of Academy of Medical Sciences 2(2):64-67.
- Bamashmus MA, Gunaid AA, Khandekar RB (2009) Diabetic retinopathy, visual impairment and ocular status among patients with diabetes mellitus in Yemen: A hospital-based study. Indian J Ophthalmol 57(4): 293-298.
- Ramachandran A, Snehalatha C, Satyavani K, Latha E, Sasikala R, Vijay V (1999) Prevalence of vascular complications and their risk factors in type 2 diabetes. J Assoc Physicians India 47(12): 1152-1156.
- Dyck PJ, Davies JL, Wilson DM, Service FJ, Melton LJ, O’Brien PC (1999)Risk Factors for Severity of Diabetic Polyneuropathy: Intensive longitudinalassessment of the Rochester Diabetic Neuropathy Study cohort. Diabetes Care 22(9): 1479–1486.
- Sveen KA, Karime B, Ellen J, Mellgren SI, Fagerland MW, et al. (2013) Small and Large Fiber Neuropathy after 40 Years of Type 1 Diabetes: Association with glycemic control and advanced protein glycation: The Oslo Study. Diabetes care 36(11):3712-3717.
- TesfayeS, Chaturvedi N, Eaton SE, Ward JD, Manes C, Ionescu-Tirgoviste C, et al (2005) EURODIAB Prospective Complications Study Group. Vascular risk factors and diabetic neuropathy. N Engl J Med 352: 341-350.
- Khandekar R, Al Lawatii J, Mohammed AJ, Al Raisi A (2003) Diabetic retinopathy in Oman: A hospital based study. Br J Ophthalmol 87(9): 1061- 1064.
- Agrawal RP, Ranka M, Beniwal R, Sharma S, Purohit VP, Kochar DK, et al (2004) Prevalence of micro and macrocomplications in type 2 diabetes and their risk factors. Int J Diab Dev Countries 24: 11-16. Prevalence of micro and macrocomplications in type 2 diabetes and their risk factors
- Wijesuriya MA, De-Abrew WK, Weerathunga A, Perera A, Vasantharajah L (2012) Association of chronic complications of type 2 diabetes with the biochemical and physical estimations in subjects attending single visit screening for complications. Journal of Diabetology1(3):1-10.
- Malone JM, Snyder M, Anderson G, Bernhard VM, Holloway GA Jr, Bunt TJ (1989) Prevention of amputation by diabetic education. Am J Surg 158(6): 520–523.
- Uccioli L, Giacomozzi C (2013) Biomechanics and choosing footwear for the diabetic foot. Wounds International 4(3): 7-11.





