Retinopathy of Prematurity: Incidence and Risk Factors
Verma A1, Nema N2*, Patel S3, Ishrat S3, Sidharth M3
1 Assistant Professor, Department of Ophthalmology, Sri Aurobindo Medical College and PG Institute, Indore, Madhya Pradesh, India.
2 Professor, Department of Ophthalmology, Sri Aurobindo Medical College and PG Institute, Indore, Madhya Pradesh, India.
3 Junior Resident, Department of Ophthalmology, Sri Aurobindo Medical College and PG Institute, Indore, Madhya Pradesh, India.
*Corresponding Author
Dr Nitin Nema,
Department of Ophthalmology, Sri Aurobindo Medical College and PG Institute,
Indore Ujjain State Highway, Indore, Madhya Pradesh, India.
Tel: +91-9893313145.
E-mail: nemanitin@yahoo.com
Received: February 25, 2016; Accepted: April 13, 2016; Published: April 20, 2016
Citation : Verma A, Nema N, Patel S, Ishrat S, Sidharth M (2016) Retinopathy of Prematurity: Incidence and Risk Factors. Int J Ophthalmol Eye Res. 4(3), 198-201. DOI : dx.doi.org/10.19070/2332-290X-1500040
Copyright : Nema N,© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: With improved neonatal care services across India, even the tiniest and sickest babies are surviving. However, they carry a high chance of developing retinopathy of prematurity (ROP). Therefore, pediatricians and ophthalmologists must be aware of the risk factors of ROP to detect and treat the disease at the earliest.
Aims: To study the incidence and risk factors that predispose to ROP.
Design: Observational study.
Methods: Preterm and low birth weight infants, born between the years 2012 and 2014, and admitted in the neonatal intensive care unit of Sri Aurobindo Medical College and PG Institute, Indore were screened for ROP. Neonates with gestational age ≤ 34 weeks and birth weight < 1500 grams were examined within 4 weeks of birth.
Results: The incidence of ROP was 23.4 % in 308 infants who were screened. Birth weight was significantly lower in infants with ROP than without ROP. Risk factors predisposing to ROP were septicemia (P=0.001), apnea (P<0.0001), oxygen therapy (P=0.003) and mechanical ventilation (P=0.004). However, only septicemia and apnea were found to be independent risk factors for development of ROP on multivariate analysis.
Conclusion: The incidence of ROP was 23.4 % and the risk factors predisposing to the disease were septicemia and apnea besides low birth weight and prematurity.
2.Introduction
3.Material and Methods
3.1.Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Low-Birth Weight; Preterm; Blindness; Apnea; Septicemia.
Introduction
Retinopathy of prematurity (ROP) is a disease of premature and low-birth-weight infants. The immature incompletely vascularized retina of these babies develops abnormal blood vessels in the retina in response to ischemia. It is a heterogeneous disorder ranging from mild transient changes in the retina with visual deterioration to severe progressive scarring, detachment of retina and irreversible blindness [1]. If identified early, this ischemic retinopathy can be treated successfully.
Lesser the birth weight more the chances of ROP. Approximately 50% of neonates with birth weight less than 1000 grams develop some degree of ROP. Besides prematurity and low birth weight, various other factors are known to be associated with ROP such as administration of oxygen, ventilation support, sepsis, hypoglycemia, blood transfusions, and bronchopulmonary dysplasia [2,3]. With advances in neonatology and improved survival of low birth weight infants, the incidence of ROP has been increasing.
The aim of this study was to find out the incidence and risk factors of ROP in a tertiary care center of central India.
Material and Methods
All premature neonates (≤34 weeks of gestational age) or babies with a birth weight of <1500 grams admitted to the neonatal intensive care unit (NICU) were screened for ROP between the years 2012-2014. The first screening was carried out at 4 weeks after birth or 31 to 33 weeks postmenstrual age (gestational age at birth plus postnatal age), whichever was later as suggested by National Neonatology Forum of India guidelines [4]. All the infants were screened by the same ophthalmologist. A prior informed and written consent of the parents was obtained.
Screening was also done for those neonates who had an unstable course with risk factors like ventilation, oxygen requirement, use of surfactant, septicemia, hyperbilirubinemia, congenital heart disease and apnea. A detailed history including birth weight, gestational age at birth, weight for gestation and, problems during NICU stay and its management were recorded.
The screening was done in the NICU in the presence of a pediatrician. Prior to screening the babies were fed in order to avoid hypoglycemia. The pupils were dilated using 0.50 % cyclopentolate and 2.5 % phenylephrine eye drop (Auropent plus) meant for premature babies. The eye drop was instilled 2 to 3 times at a gap of 10 to 15 minutes apart and excess of eye drop was wiped from the cheeks. The examination was done with a binocular indirect ophthalmoscope using 20 D and 28 D lenses (especially for poorly dilating pupils) and a pediatric scleral depressor. The eyelids were separated using a pediatric eye speculum after anesthetizing the ocular surface with 0.50 % proparacaine eye drop.
The stage or severity of the disease, as shown in Table 1, was recorded during the screening according to International Classification of Retinopathy of Prematurity (ICROP) [5]. The findings were recorded in the form of fundus drawings. The children who needed treatment were advised accordingly and those who required follow-up were given the dates for the next visit.
Statistical Analysis was performed using SPSS version 20.0. Univariate analysis was conducted using Chi square test. Multiple logistic regression analysis was performed to study the predictors of ROP using independent variables as those variables which were significant in the univariate analysis.
Results
Three hundred and eight infants were screened for ROP in the NICU from year 2012-2014. Their birth weight ranged from 640 to 2000 grams with a mean of 1300 ± 242 grams. The gestational age ranged from 22 - 37 weeks with a mean of 29.1 ± 2.2 weeks. There were 188 males and 120 females. ROP was observed in 72 (23.4 %) infants; out of which 41 (57 %) were males and 31 (43 %) were females. Mean days of hospitalization was 24.8 ± 12.9 days.
The overall incidence of ROP was 23.4 %. In 69 (96 %) infants, both eyes were affected and in 3 (4 %) infants, only one eye was affected (Table 2). The mean birth weight of patients with ROP and without ROP was 1029 ± 152 grams and 1380 ± 202 grams, respectively. The difference in mean birth weight between two groups was statistically significant (P< 0.0001).
The risk factors identified were oxygen therapy, ventilation, congenital heart disease, septicemia, apnea, hyperbilirubinemia, phototherapy, hyaline membrane disease (HMD), necrotizing enterocolitis (NEC) and pneumonia. A univariate analysis was done taking each risk factor for ROP. Out of the ten risk factors that were studied, septicemia (P=0.001), apnea (P <0.0001), oxygen therapy (P=0.003) and ventilation (P=0.004) were found to be significantly associated with ROP (Table 3). On multiple logistic regression analysis, only septicemia and apnea were found to be independent risk factors for the development of retinopathy of prematurity, as shown in Table 4.
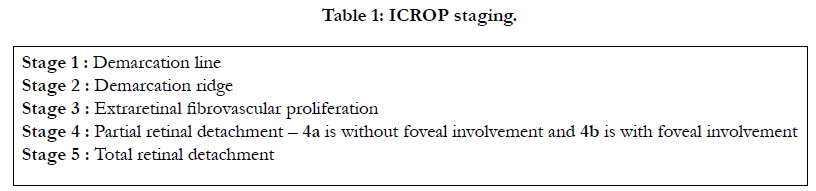

Table 1: ICROP staging.
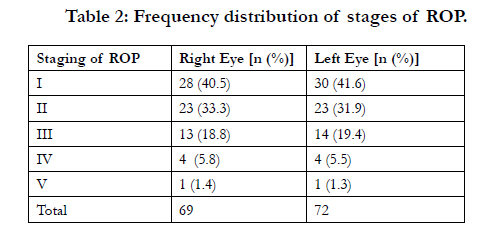
Table 2: Frequency distribution of stages of ROP.
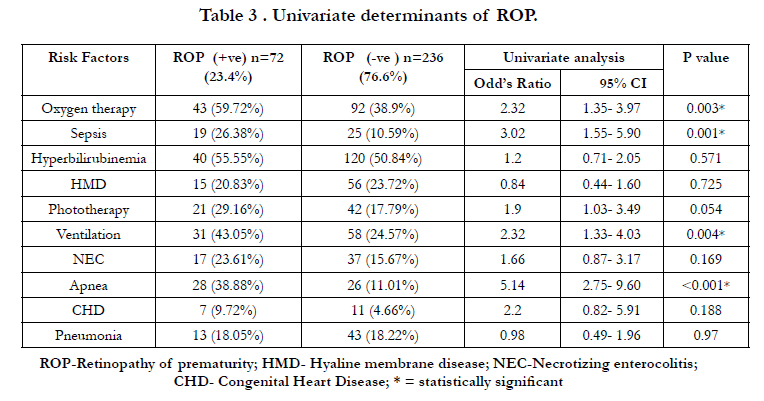
Table 3 . Univariate determinants of ROP.
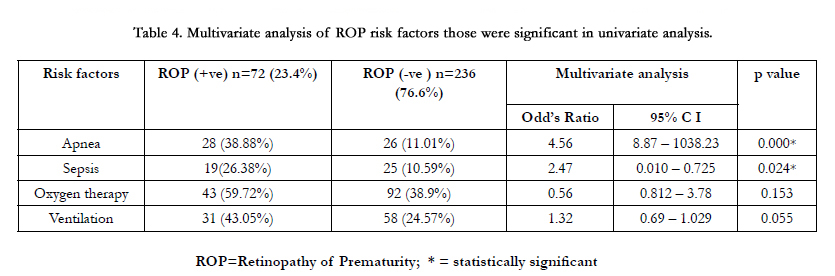
Table 4. Multivariate analysis of ROP risk factors those were significant in univariate analysis.
Discussion
The incidence of ROP in India is reported to be between 38 and 51.9 % in low birth weight infants [6-8]. With improved survival rates of sick neonates the incidence of ROP in India has increased. The nasal retina is vascularized at birth in a normal term newborn while temporal retina gets vascularized by 39 to 41 weeks postnatally. During intrauterine life, the avascular retina produces vascular endothelial growth factor (VEGF) that helps in vasculogenesis of developing retina. In premature and preterm infant there occurs down regulation of VEFG due to hyperoxia. However, due to increased oxygen demand of fast developing eye, VEGF is up regulated which results in ROP within 4 to 5 weeks after birth.
Screening for ROP is mandatory in order to detect and diagnose infants with early treatable form of the disease [9]. The treated eyes show a better visual outcome than untreated eyes [10-12]. Different countries follow different ROP screening guidelines [13-18]. American Academy of Pediatrics recommended to screen all neonates with a birth weight <1500 grams or gestational age ≤28 weeks, as well as selected children between 1500 and 2000 grams with an unstable course who are believed to be at high risks by their attending pediatrician [13]. According to the Joint Working Party of the Royal College of Ophthalmologists and the British Association of Perinatal Medicine infants with a birth weight of ≤1500 grams or a gestational age of ≤31 weeks should be screened for ROP [18].
National Neonatology Forum of India has recommended the guidelines for ROP screening of Indian babies [4]. According to it, all preterm neonates who are <34 weeks of gestation and/ or <1750 grams birth weight should be screened for ROP. Tiny infants who are <28 weeks or <1200 grams birth weight should be screened early at 2 to 3 weeks of post menstrual age (gestational age at birth plus postnatal age in weeks) because they may develop an aggressive form of ROP (aggressive posterior ROP, AP-ROP) [15, 19]. AP-ROP is reported to be common in Indian babies which has a worse visual prognosis as compared to classical ROP [20, 21]. The cessation of screening is recommended on full retinal vascularization or regression of retinal signs of ROP.
We screened all neonates admitted in NICU with birth weight <1500 grams and gestation ≤34 weeks as recommended by many authors [22-25]. Infants with birth weight ≥1500g and gestation more than 34 weeks were also screened when the treating neonatologist felt the requirement for it. Tiny and younger infants were screened at 2 to 3 weeks of birth. The incidence of ROP in our study was 23.7 %. It was same as reported in other studies [26-28]. In a recent study done on Indian population, Chatopadhayay et al [29] found 44 % incidence of ROP which was almost similar to that noted by Gopal et al (38 %) [7].
Prematurity and low birth weight are recognized as major risk factors for ROP [30-32]. The lower the gestational age or birth weight, the higher the risk of developing severe ROP. The third factor besides the two major risk factors also plays a role in the pathogenesis of the disease. This includes prolonged unmonitored oxygen therapy, anemia, double volume exchange, packed cell volume transfusion, septicemia, apnea and ventilation [14, 26, 33, 34]. Many studies have found erythrocyte transfusion to be an independent risk factor for ROP due to the presence of non-protein bound iron load in the plasma, a potent catalyst of oxidative injury [35-37]. In our study, children having septicemia, apnea, prolonged oxygen therapy and mechanical ventilation showed high frequency of ROP. However, only septicemia and apnea were found to be independent significant risk factors for the development of ROP. Similar to our finding, other authors have also reported septicemia and apnea to be the risk factors for ROP [14, 26, 29].
Conclusion
Screening for ROP aids in diagnosing the disease early and helps in preventing childhood blindness. A carefully timed retinal examination by an ophthalmologist, of at risk infants determined by pediatrician, becomes extremely important in ROP as the disease in its initial stages remains asymptomatic.
References
- Terry TL (1942) Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Am J Ophthalmol 25(2): 203-204.
- Hammer ME, Mullen PW, Fergusson JG, Poi S, Cosbox C, et al. (1986) Logistic analysis of risk factors in acute retinopathy of prematurity. Am J Ophthalmol 102(1): 1-6.
- Seiberth V, Linderkamp O (2000) Risk factors in retinopathy of prematurity. A multivariate statistical analysis. Ophthalmologica 214(2): 131-135.
- National Neonatology Forum of India, National Neonatal Perinatal Database, Report for Year 2002-2003, National Neonatology Forum of India, New Delhi, 2005.
- International Committee for the Classification of Retinopathy of Prematurity (2005) The International Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol 123(7): 991-999.
- Charan R, Dogra MR, Gupta A, Narang A (1995) The incidence of retinopathy of prematurity in a neonatal care unit. Indian J Ophthalmol 43(3):123-126.
- Gopal L, Sharma T, Ramchandran S, Shanmugasundaram R, Asha V (1995) Retinopathy of prematurity. A study. Indian J Ophthalmol 43: 50-61.
- Varughese S, Jain S, Gupta N, Singh S, Tyagi V, et al. (2001) Magnitude of the problem of retinopathy of prematurity. Experience in a large maternity unit with a medium size level-3 nursery. Indian J Ophthalmol 49(3): 187-188.
- Gurdian SJ, Gehlbach PI, Hunyor AP, Robertson JE (2001) Retinal detachment associated with subthreshold retinopathy of prematurity. J Pediatr Ophthalmol Strabismus 38(5): 279-283.
- Cryotherapy for Retinopathy of Prematurity Cooperative Group (2001) Multicenter trial of cryotherapy for retinopathy of prematurity: Ophthalmological outcomes at 10 years. Arch Ophthalmol 119(8): 1110-1118.
- Laws F, Laws D, Clark D (1997) Cryotherapy and laser treatment for acute retinopathy of prematurity: Refractive outcomes, a longitudinal study. Br J Ophthalmol 81(1): 12-15.
- Foroozan R, Connolly BP, Tasman WS (2001) Outcomes after laser therapy for threshold retinopathy of prematurity. Ophthalmology 108(9): 1644- 1646.
- American Academy of Pediatrics, Section on Ophthalmology (2013) Screening examination of premature infants for retinopathy of prematurity. Pediatrics131(1): 189-195.
- Vinekar A, Dogra M, Sangtam T, Narang A, Gupta A (2007) Retinopathy of prematurity in Asian Indian babies weighing greater than 1250 grams at birth: ten year data from a tertiary care center in a developing country.Indian J Ophthalmol 55(5): 331-336.
- Jalali S, Anand R, Kumar H, Dogra MR, Azad RV, et al. (2003) Programme planning and screening strategy in retinopathy of prematurity. Indian J Ophthalmol 51(1): 89-97.
- Jalali S, Hussain A, Matalia J, Anand R (2006) Modification of screening criteria for Retinopathy of Prematurity in India and other middle income group countries. Am J Ophthalmol 141(5): 966-968.
- Jalali S, Anand R, Rani PK, Balakrishnan D (2014) Impact of the day-30 screening strategy on the disease presentation and outcome of retinopathy of prematurity. The Indian twin cities retinopathy of prematurity report number 3. Indian J Ophthalmol 62(5): 610-614.
- Joint working party of the Royal College of Ophthalmologists and the British Association of Perinatal Medicine (1996) Retinopathy of prematurity: Guidelines for screening and treatment. Early Hum Dev 46(3): 239-258.
- Quiram PA, Capone A (2007) Current understanding and management of retinopathy of prematurity. Current Opinion in Ophthalmology 18(3): 228-234.
- Sanghi G, Dogra MR, Das P, Vinekar A, Gupta A, et al. (2009) Aggressive posterior retinopathy of prematurity in Asian Indian Babies: Spectrum of Disease and Outcome after Laser Treatment. Retina 29(9): 1335-1339.
- Shah PK, Narendran V, Sarvanan VR, Raghuram A, et al. (2005) Fulminate retinopathy of prematurity – Clinical characteristics and laser outcome. Indian J Ophthalmol 53(4): 261-265.
- Early treatment for retinopathy of prematurity cooperative group (2003) Revised indications for the treatment of retinopathy of prematurity: Results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol 121(12): 1684-1694.
- Cryotherapy for Retinopathy of Prematurity Cooperative Group (1988) Multicenter trial of cryotherapy for retinopathy of prematurity: Preliminary results. Pediatrics 81(5): 697-706.
- The STOP-ROP Multicenter Study Group (2000) Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity (STOP-ROP), A randomized, controlled trial. I: Primary outcomes. Pediatrics 105(2): 295-310.
- Castro Conde JR, Echániz Urcelay I, Botet Mussons F, Pallás Alonso CR, Narbona E, et al. (2009) Retinopathy of prematurity. Prevention, screening and treatment guidelines. Ann Pediatr (Barc) 71(6): 514–523.
- Aggarwal R, Deorari AK, Azad RV, Kumar H, Talwar D, et al. (2002) Changing profile of retinopathy of prematurity. Trop Pediatr 48(4): 239-242.
- Gupta VP, Dhaliwal U, Sharma R, Gupta P, Rohatgi J (2004) Retinopathy of prematurity – risk factors. Indian J Pediatr 71(10): 887- 892.
- Chaudhari S, Patwardhan V, Vaidya U, Kadam S, Kamat A (2009) Retinopathy of Prematurity in a Tertiary Care Center – Incidence, Risk Factors and Outcome. Indian Pediatr 46: 219-224.
- Chattopadhyay MP, Pradhan A, Singh R, Datta S (2015) Incidence and Risk Factors for Retinopathy of Prematurity in Neonates. Indian Pediatr 52:157-158.
- Hussain N, Clive J, Bhandari V (1999) Current incidence of retinopathy of prematurity, 1989-97. Pediatrics 104(3): e26.
- Nguyen QD, Tawansy K, Hirose T (2001) Recent advances in retinopathy of prematurity. Int Ophthamol Clin 41(4): 129-151.
- Larsson E, Carle-Petrelius B, Cerneurd G, Ots L, Wallin A, et al. (2001) Incidence of ROP in two consecutive Swedish population based studies. BrJ Ophthalmol 86(10): 1122-1126.
- Rekha S, Battu RR (1996) Retinopathy of prematurity: incidence and risk factors. Indian Pediatr 33(12): 999-1003.
- Dutta S, Narang A, Dogra MR, Gupta A (2004) Risk factors of threshold retinopathy of prematurity. Indian Pediatr 41(7): 665-671.
- Termote JUM, Donders ART, Schalij-Delfos NE, Lenselink CH, van Angeren, et al. (2005) Can screening for retinopathy of prematurity be reduced?Biology of the neonate 88(2): 92-97.
- Cooke RWI, Clark D, Mickey-Owyer M, Weindling AM (1993) The apparent role of blood transfusions in the development of retinopathy of prematurity.Eur J Pediatr 152(10): 833-836.
- Inder TE, Clemett RS, Austin NC, Graham P, Darlow BA (1997) High iron status in very low birth weight infants is associated with an increased risk of retinopathy of prematurity. J Pediatr 131(4): 541-544.





