Influence of Screen Exposure on Vergence Components from Childhood to Adolescence
Ajrezo L1,2, Wiener-Vacher S1,2, Bucci MP1,2, Bui-Quoc E3*
1.UMR 1141, INSERM- Université Paris 7, Hôpital Robert Debré, 48 boulevard Sérurier, Paris, France.
2 Vestibular and Oculomotor Evaluation Unit (EFEE), ENT Department, Robert Debré Paediatric Hospital, 48 boulevard Sérurier, 75019 Paris, France.
3 Ophthalmology Department, Robert Debré University Hospital, 48 boulevard Sérurier, 75019, Paris, France.
*Corresponding Author
Emmanuel Bui-Quoc,
Ophthalmology Department, Robert Debré University Hospital,
48 boulevard Sérurier, 75019, Paris, France.
E-mail: emmanuelbui@outlook.com
Received: November 21, 2015;Accepted: January 07, 2016; Published: January 12, 2016
Citation: Ajrezo L, Wiener-Vacher S, Bucci MP, Bui-Quoc E (2016) Influence of Screen Exposure on Vergence Components from Childhood to Adolescence. Int J Ophthalmol Eye Res.4(1), 170-177.DOI : dx.doi.org/10.19070/2332-290X-1500036
Copyright: Bui-Quoc E© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The goal of our study is to explore the impact of screen exposure on vergence components in children. Sixty-eight healthy children (aged from 5.4 to 16 years old) were studied. We recorded vergence components (near point of convergence, heterophoria at far and near distances, fusional amplitudes of convergence and divergence at far and near distances, AC/A ratio). We reported the time spent in front of screens at near and far distance per day. NPC value is 1.87 ± 1.05 cm. Phoria at far is -0.29 ± 0.21 pD. Phoria at near is -3.00 ± 0.45 pD. Fusional amplitudes are as follows: convergence at far is 18.72 ± 0.73 pD; convergence at near is 38.16 ± 0.98 pD; divergence at far is 4.76 ± 0.19 pD; divergence at near is 17.01 ± 0.33 pD. AC/A ratio is 2.35 ± 0.08. Amplitude of divergence and convergence at near distance decreased significantly with age, while other vergence components did not vary. The time spent in front of screens at near distance increased significantly with age. There is a significant correlation between the amplitudes of convergence and exposure time to screens (both at near distance). Our study, beside reporting precise normative vergence data in children, suggests that near distance activity could possibly allow older children to have better vergence accuracy at near distance and a smaller range of vergence amplitude as a possible consequence of visual training.
2.Abbreviations
3.Introduction
4.Methods
4.1.Subjects
4.2.Ophthalmologic and orthoptic evaluation of vergence components
4.3.Time spent in front of screens
4.4.Statistical analysis
5.Results
6.Discussion
6.1.Normative data of vergence components
6.2.The amplitude of divergence and convergence at near distance decreased with age
6.3.The screen exposure time and amplitude of convergence at near distance
7.Conclusion
8.Acknowledgements
9.References
Keywords
Screen Exposure; Vergence Normative Data; Children; Development; Vergence; AC/A.
Abbreviations
AC/A – accommodative convergence/accommodation; cm – centimeter; m – meter; NPC – near point of convergence; pD – prism Diopters.
Introduction
Vision is a complex task, the motor component of which uses a combination of eye movements; including version and vergence. Version eye movements correspond to all conjugated eye movements where both eyes shift in tandem (i.e. saccadic movements which allow precise ballistic movements towards the visual target, but also pursuits which allow maintaining the gaze toward a moving target), while during vergence the eyes rotate in opposition, i.e. for horizontal vergences via either inward (convergence) or outward (divergence) movements. Binocular coordination is a critical skill necessary for normal vision [1, 2]. The stability of binocular vision depends on good fusional amplitudes [3]. Fusional vergence movements align the visual axes precisely to enable single binocular vision [4]. The sensory visual monocular or binocular information (i.e. information about relative depth) is sent from the visual cortex to the motor control centers in the motor cortex and in the brainstem, where different neuronal structures control vergences, such as the phasic excitatory neurons in the paramedian pontine reticular formation and the tonic neurons of the mesencephalic reticular formation [5].
Vergence is a key function that can be abnormal in several conditions. It can be evaluated through the measurement of various clinical components: measurement of near point of convergence (NPC), fusional amplitudes of convergence or divergence at far or near distance, measurement of phoria, calculation of accommodative convergence/accommodation (AC/A) ratio. However, while several publications report that an insufficiency of convergence can occur in several conditions in children (e.g. Attention deficit hyperactivity disorder or ADHD, dyslexia, headaches and/or vertigo) [6-9], in the literature,normative data for vergence components varies greatly [10-18]. For convergence at far distance, values vary greatly from 8 prism Diopters (pD) [19] to a maximum of 38 pD [20]. For divergence at far distance, values vary from 2 pD [19, 21] to 10 pD [20, 22]. At near distance, convergence values vary from 15 pD [23] to a maximum of 51 pD [20] while divergence values vary greatly from 6 pD [24] to 21 pD [25, 26] (see Table 1).
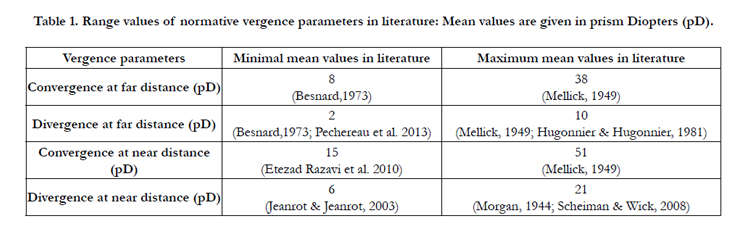

Table 1. Range values of normative vergence parameters in literature: Mean values are given in prism Diopters (pD).
Methods also vary between studies. Clinical vergence can be evaluated through measurement of fusional amplitude of convergence or divergence, at far or near. Berens et al. [10] measured horizontal vergences with prism bars in a population of 218 adults. Morgan [25] established normative vergence values in a population of 800 non-presbyopic adults by using Risley prisms and a phoropter. Mellick [20] reported vergence measurements in a population of 561 subjects (from infancy to 67 years of age), and compared the results obtained with either a prism stereoscope or a synoptophore and two types of targets (a fusion target and a stereoscopic target). No target effect was found. No significant influence of age occurred. The amplitude of convergence at far and near vision was found twice as large when measured with the synoptophore than when measured with a prism stereoscope. Wesson [11] examined a population of 79 adults by using a prism bar. Recently, Etezad Razavi et al. [23] determined normative vergence data in a population of 111 young adults by using rotatory prisms.
Several studies were performed on children: Scheiman et al. [12] determined average values of vergence in a population of 386 children from 6 to 12 years old by using a Berens prism bar and a rear illuminated and polarized target at near distance, while Rouse et al. [13] determined average values of vergence at near distance in a population of 206 children from 8 to 12 years old. More recently, Jimenez et al. [15] established vergence normative data with prism bar in a large population of 1056 children from 6 to 12 years old. Additionally, they compared vergence data between two different age groups (6–8 and 9–12 years) and they couldn’t distinguish any significant differences between the age groups. Yet, their study did not include teenagers above 12 years old while we can expect an evolution of vergence parameters during adolescence.
Moreover Radakovic et al. [18] studied vergence amplitudes with prism bar in a population of 152 children aged from 6 to 7 years old, which is a narrow range of age to establish normative vergence data. Their average results for convergence were 13.7 pD at far and 29.6 pD at near, for divergence average results were 7.3 pD at far and 16.2 pD at near. These authors found a significant correlation between far and near convergence amplitudes, and between far and near divergence amplitudes.
Another vergence measurement is the evaluation of the near point of convergence (NPC) which is the closest point of distance at which a subject is still able to converge. In previous studies, the values of NPC also varied greatly. Scheiman et al. [27] reported that 175 adults aged from 22 to 37 years had a mean NPC value of 2 cm; Rouse et al. [13] also reported an NPC of 2 cm in children. By contrast, Péchereau et al. [21] estimated an NPC of approximately 8 to 10 cm but did not specify the age of the subjects tested. These variations of values could be due to the difficulty of precisely measuring the NPC.
We noted that no one of these studies evaluated the correlation between vergence parameters in healthy children and their screen exposure (tablets, mobile phones, PC's screen) which are more and more used nowadays [28].
Indeed, nowadays, new exogenous factors such as screen exposure can influence the development of vergence in children and teenagers. It is precisely the goal of our study that is to explore the possible influence of screen exposure on vergence components in a large population of healthy children without any ophthalmologic, neurologic or vestibular pathology and to study the developmental aspect of vergence from childhood to adolescence. Indeed, because of the recognised relationship between screen exposure and visual fatigue [29], we decided to study the possible impact of the increasingly broad use of screens on these vergence components which is the novelty of this study. That is why we decided to record vergence components data in children and teenagers, to study a possible developmental pattern of the recorded parameters and to evaluate the possible effect of screen exposure on the vergence components.
Methods
Ninety-two asymptomatic healthy children were examined. Sixtyeight children (aged from 5.4 to 16 years old with a mean age of 9.68 ± 0.38) were included in this study. Inclusion criteria required in children >5 years old and <16 years old, a visual acuity < or =20/20 in each eye at far and near distances. No subject could have a myopia < -1.00 Diopter or a hyperopia > + 1.00 Diopter, or an astigmatism < -1.00 Diopter. All had to have a normal stereoacuity = or < 60 seconds of arc (TNO test); indeed, all included subjects had normal stereoscopic vision (mean value 59.91 ± 1.05 seconds of arc).
The inclusion criteria were established to create a more homogeneous population since refraction may influence the vergence values. Hence 24 children were excluded from our analysis due to the fact that they had at least one criterion out of range of the normal visual parameters cited above.
The subjects included in the study did not suffer from vertigo or headaches. All subjects underwent a neurological and vestibular evaluation to assess normality of neurological, hearing and vestibular functions.
An ophthalmologic and orthoptic evaluation was undertaken. None of the subjects showed any strabismus.
The investigation adhered to the principles of the Declaration of Helsinki and was approved by our institutional Human Experimentation Committee (Comité de Protection des Personnes CPP Ile de France V, Hôpital Saint-Antoine). Informed written consent was obtained for each subject and their parents after careful review of the experimentation with the subjects.
Ophthalmologic examination included visual acuity with a decimal visual acuity scale at far distance (Auto chart projector ACP-8 Series), and a near vision Parinaud test at near distance. The corrected monocular visual acuity was normal for both eyes (≥ 20/20) at far and near distances for all subjects. Ten of the children were wearing spectacles and for them all orthoptic tests were carried out with their spectacles on. Ametropia was excluded in the other children through visual examination with subjective refraction. Vergence measures were therefore recorded in all children in their habitual conditions of daily activity.
To define the stereo-acuity, we used the TNO random dot test (Netherlands Organization of Applied Scientific Research Test of stereo-acuity).
The near point of convergence (NPC) was evaluated by slowly bringing a small target from 25 centimeters (cm) on the midline of the subject’s forehead to his or her nasal base while he or she had to keep his or her eyes on the target and by determining when one eye broke fixation. The subject was instructed to concentrate on the small target to keep it clear and single. When the small target doubled, the operator had to stop moving forward and had to ask the subject if he or she could make the object single. If the subject was able to fuse the target, then the operator could slowly move the small character closer. When the subject could no longer maintain fusion, the distance was measured. The measure was repeated at least twice [30].
Heterophoria (i.e. the latent deviation of one covered eye when the other is not covered) was measured at far (5 m, i.e. meters) and near (30 cm) distances with the cover–uncover test. The horizontal deviation was neutralized with a base-in or base-out prism bar of Berens.
Fusional amplitudes of divergence and convergence were measured at far distance (5m) and near distance (30cm) by using a base-in and a base-out prism bar of Berens. We noted the breakpoint, i.e. the prism power obtained before the subject reports diplopia. Most subjects are able to recognize diplopia when the breakpoint is reached, but some do not. In such cases the breakpoint is determined by observation. Recall that when testing vergence ranges, the observation of the eye behind the prism is also important to avoid suppression. Divergence amplitude was measured before the amplitude of convergence.
The ratio of accommodative convergence (AC) over accommodation (A) indicates the relationship between the amount of convergence produced by a stimulus to accommodate and the amount of accommodation which participates in that convergence [31]. To measure the AC/A ratio, we used the gradient method, in which the calculation of the ratio requires the measurement of phoria in several conditions (Jeanrot and Jeanrot, 2003). The heterophoria at near distance (30cm) was measured initially with + 3.00 glasses, then with + 1.00 glasses, then without the addition of test glasses. Then heterophoria was measured with concave glasses of -1.00 and then -3.00 Diopters.
In order to determine whether the time spent in front of visual screens influences the development of vergence eye movements in children, some questions were asked to each child and their parents by the examiner. By these questions, we collected data regarding the mean time spent in front of a TV screen (far distance) and the mean time spent in front of computer games, video games and touch pads (near distance) per day.
Data were analysed using ten different multiple linear regression models with convergence, divergence, phoria, NPC and AC/A ratio and screen exposure time (at respectively near and far distances). Predictor variables for each test were the children’s ages (in months) and the screen exposure time.
Results
The mean values of all vergence components for all children are shown at Table 2.
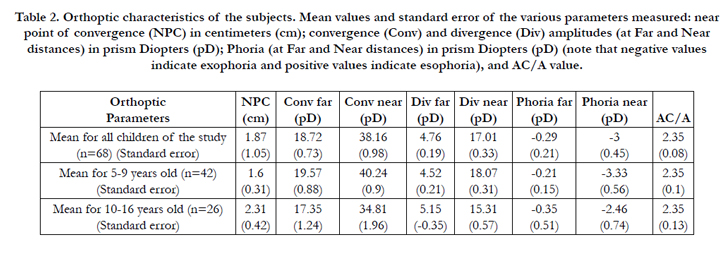
Table 2. Orthoptic characteristics of the subjects. Mean values and standard error of the various parameters measured: near point of convergence (NPC) in centimeters (cm); convergence (Conv) and divergence (Div) amplitudes (at Far and Near distances) in prism Diopters (pD); Phoria (at Far and Near distances) in prism Diopters (pD) (note that negative values indicate exophoria and positive values indicate esophoria), and AC/A value.
NPC value is 1.87 ± 1.05 cm. Phoria at far is -0.29 ± 0.21 pD. Phoria at near is -3.00 ± 0.45 pD. Fusional amplitudes are as follows: convergence at far is 18.72 ± 0.73 pD; convergence at near is 38.16 ± 0.98 pD; divergence at far is 4.76 ± 0.19 pD; divergence at near is 17.01 ± 0.33 pD. AC / A ratio is 2.35 ± 0.08.
The NPC (R²=0.0334; R=0.1828; p=0.136), the phoria at far (R²=0.012; R= -0.1096; p=0.374) and near distance (R²=0.0065; R=0.0805; p=0.514) and the AC/A value (R² = 0.0054; R= -0.734; p=0.552) do not vary with age (Figure 1, Figure 2A, Figure 2B, Figure 3).
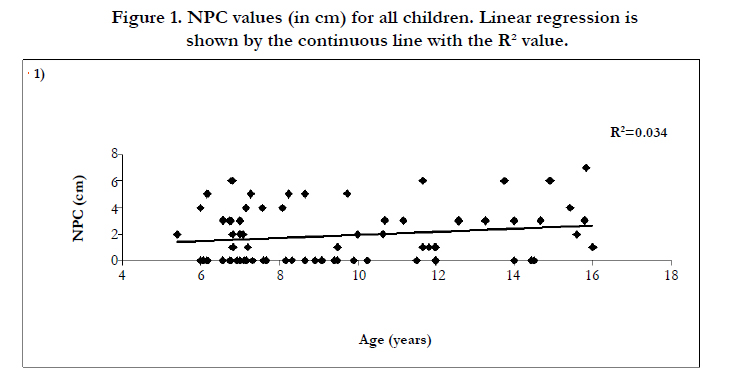
Figure 1. NPC values (in cm) for all children. Linear regression is shown by the continuous line with the R² value.
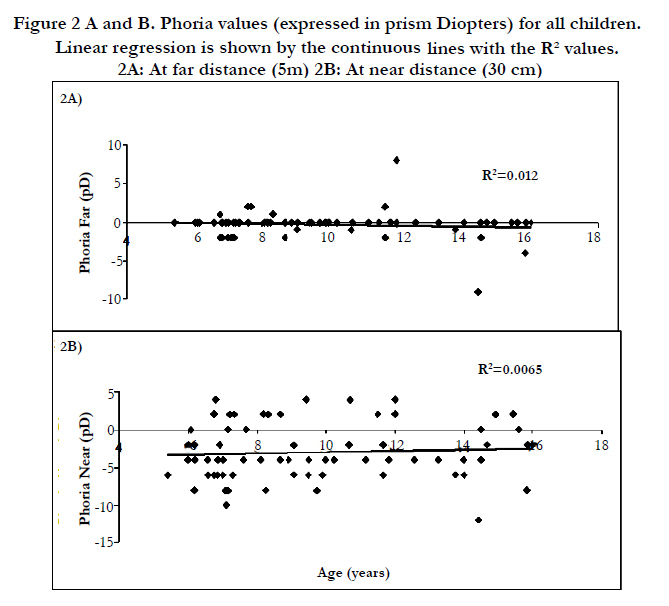
Figure 2 A and B. Phoria values (expressed in prism Diopters) for all children. Linear regression is shown by the continuous lines with the R² values. 2A: At far distance (5m) 2B: At near distance (30 cm)
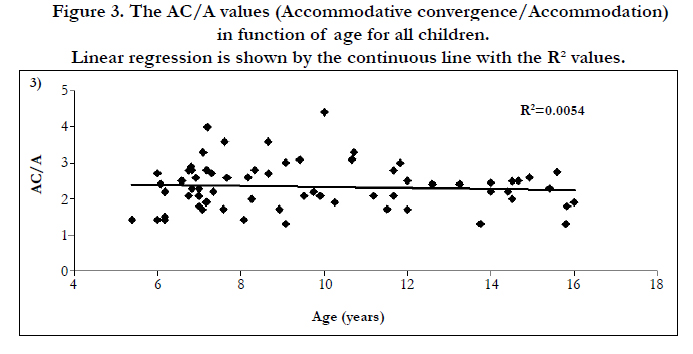
Figure 3. The AC/A values (Accommodative convergence/Accommodation) in function of age for all children. Linear regression is shown by the continuous line with the R² values.
At far distance there is no significant correlation between age and divergence (R² = 0.0062; R=0.0789; p=0.523) or convergence values (R² = 0.0185; R= -0.1361; p=0.269) (Figure 4A & Figure 4B). In contrast, at near distance (Figure 4C & Figure 4D) values of divergence and convergence decrease significantly as the children’s ages increase (respectively, R²= 0.2794; R= -0.5286; p <0.0001 and R²= 0.1602; R= -0.4002; p<0.001).
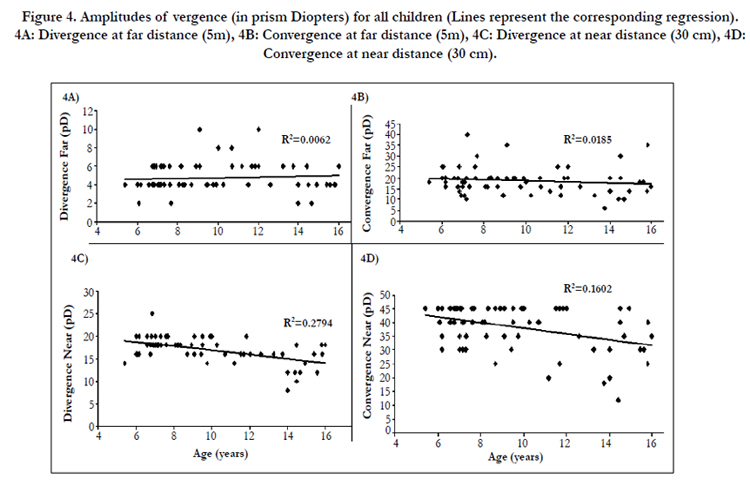
Figure 4. Amplitudes of vergence (in prism Diopters) for all children (Lines represent the corresponding regression). 4A: Divergence at far distance (5m), 4B: Convergence at far distance (5m), 4C: Divergence at near distance (30 cm), 4D: Convergence at near distance (30 cm).
The time spent in front of screens at far distance does not vary with age (R² = 0.0266; R= -0.1630; p=0.191). On the contrary the time spent in front of screens at near distance significantly increases with age (R² = 0.1769; R= 0.4206; p<0.0001) (Figure 5A & 5B). Furthermore, the amplitude of convergence at near distance decreases significantly while the time of screen exposure at near distance increases (R²=0.1459; R=-0.3819; p <0.002) (see Figure 6). However there is no correlation between the amplitude of divergence at near distance and the time of screen exposure at near distance (R²=0.000007; R=0.0026; p=0.983).
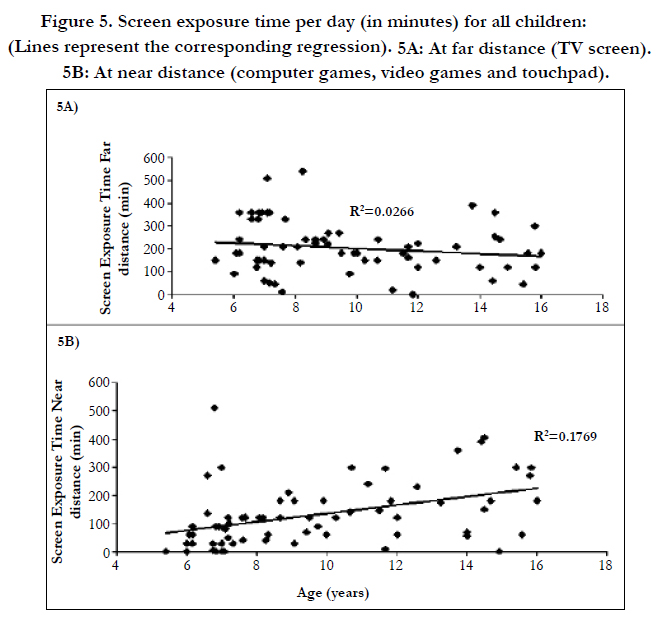
Figure 5. Screen exposure time per day (in minutes) for all children: (Lines represent the corresponding regression). 5A: At far distance (TV screen). 5B: At near distance (computer games, video games and touchpad).
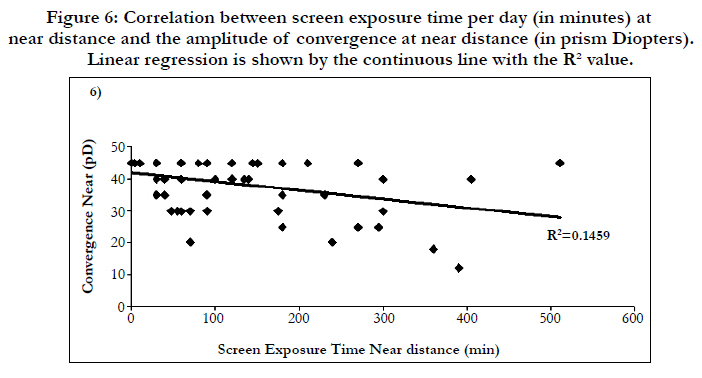
Figure 6: Correlation between screen exposure time per day (in minutes) at near distance and the amplitude of convergence at near distance (in prism Diopters). Linear regression is shown by the continuous line with the R² value.
Discussion
The main findings of this study are as follows: (i) This study provides normative data of vergence components in healthy children and teenagers for clinicians; (ii) The amplitude of divergence and convergence at near distance decreases significantly as the age of children increases; (iii) The screen exposure time at near distance increases significantly with age and is significantly correlated to the value of convergence but not the value of divergence. These findings are discussed individually below.
This study provides normative vergence data based on a population of 68 children aged from 5.4 to 16 years. The mean values for divergence at far distance in our pediatric population are similar to those reported in children by Jeanrot and Jeanrot [24], Scheiman and Wick [26] and Radakovic et al. [18]; while for near distance, the mean values of divergence are similar to the results of Rouse et al. [13] and Radakovic et al. [18]. For convergence at far distance, our values are similar to those reported by Scheiman and Wick [26] and Jimenez et al. [15]; and for convergence at near distance, our values are similar to those found by Besnard [19]; Hugonnier and Hugonnier [22] and Péchereau et al. [21].
The mean NPC’s found in our population is similar to that found by Rouse et al. [13] in a population of 8 to 12-year-old children.
Our values of phoria at far distance, as well as phoria at near distance, are similar to those reported by Scheiman and Wick [26] and close to the data of Rouse et al. [13] and Radakovic et al. [18].
Our mean AC/A value ratio is similar to the result of Jimenez et al. [15] using the same measurement method. These authors also did not find a modification of AC/A ratio with age. Note that according to Sen and Malik [31] and Péchereau et al. [32], the AC/A ratio is innate and constant during life and varies from one subject to another.
In summary, our data support a significant amount of the vergence data reported by previous literature. However, our results should be confirmed in larger populations of healthy children in future studies.
Another new finding of the present study is that the amplitude of divergence and convergence at near distance was decreasing significantly as the age of the children was increasing. Also Lyon et al. [16] who studied vergence with prism bar in a population of 879 children from 6 to 11 years old, found a decrease with age of the divergence amplitude at near distance only. Contrary to our findings, Scheiman et al. [12] reported a significant lower value of vergence at near distance for 6-year-old children in comparison to 7 to 12–year-old children. These authors suggest that this difference could be due to the cognitive difficulty of the task for the youngest children. In this study, children were asked to name the target (a letter or a number) during the vergence examination and the letter or number recognition is generally more difficult and takes longer for 6-year-old children compared to older children. Moreover Jimenez et al. [15] did not find a significant evolution of convergence and divergence at far and near distances between 6 and 12 years old in a population of 1056 children. Such difference could stem from the different method used by Jimenez’ study and our study. Indeed, these authors placed the subjects on a chin rest placed at 40 cm from the target that they had to fixate at near distance while we measured vergence amplitude at 30 cm at near and subjects were not placed on a chin rest. Moreover the reason why we found a decrease of vergence at near may be because we extended the age range of our studied subjects to teenagers.
Eventually, we found that the exposure time at near distance (time spent in front of the screens at near distance) increased significantly with age and is significantly correlated to a smaller amplitude of convergence, this is not, however, the case for divergence. This result differs from Gratton et al. [33], who evaluated the variation of vergence parameters after a two-year follow-up in a population of 70 video display terminal operators and concluded that screen exposure had no influence on vergence parameters. Note that this study was carried out on adults only. We did not find any studies on the possible correlation between vergence components and screen exposure in children.
On one hand, our findings suggest that children could perform convergence with lower amplitudes to avoid effort because they obtain better and more accurate convergence movements by training their vision at near distance (for instance using screens such as video games, touch pads, etc.) but do not improve their divergence with this type of daily activity. This interpretation is supported by the results of Van Leeuwen et al. [34] and Jainta et al. [35] who showed that repetitious eye movements improve the dynamic of vergence along the midline. To complete this observation, eye movements should be recorded in children to precisely measure latency and gain of vergence in a dynamic condition before and after training during near vision activities. On the other hand, this decrease of vergence amplitude with age could be due to an innate developmental aspect of the maturation of different cortical and sub-cortical areas controlling vergence during childhood [36].
Conclusion
Our study reports new normative data of vergence components in a population of children from 5.4 to 16 years old and shows that screen exposure increases with age. It shows that there is a significant correlation between the amplitudes of convergence and exposure time to screens (both at near distance); indeed, a significant correlation was found between age and the amplitude of divergence and convergence at near distance; furthermore, the time spent at near distance increased significantly with age and is significantly correlated to a decrease of convergence amplitude. This suggests that children could improve their convergence performances by spending more time at near distance, but this activity does not improve divergence performance as divergence amplitudes could be decreased if too much effort at near distance is performed. This also suggests that daily activities such as visual training at near distance possibly using screens could have an impact on oculomotor development in children.
Acknowledgements
The authors wish to thank the parents and children of this study for their kind participation. We also thank Cynthia Lions and Damien Melithe for their support in writing this article. The authors are grateful to the APHP (Assistance Publique Hôpitaux de Paris) for their financial support (PHRC Régional which grant number is: 10801-AOR09078-IDRCB2010- AOO361-38VERVE). We are deeply grateful to Ms Chloe Ann Barker and Omar Zerkly for revising the manuscript.
References
- Alvarez TL, Kim EH (2013) Analysis of saccades and peak velocity to symmetrical convergence stimuli: binocularly normal controls compared to convergence insufficiency patients. Invest Ophthalmol Vis Sci 54(6): 4122- 4135.
- Gaertner C, Bucci MP, Ajrezo L, Wiener-Vacher S (2013) Binocular coordination of saccades during reading in children with clinically-assessed poor vergence capabilities. Vision Res 87: 22-29.
- Fray KJ (2013) Fusional Amplitudes: Exploring Where Fusion Falters. Am Orthopt J 63: 41-54.
- Leigh RJ, Zee DS (2006) The neurology of eye movements. (4th edtn), Oxford University Press, New York.
- Cullen KE, Van Horn MR (2011) The neural control of fast vs. slow vergence eye movements. Eur J Neurosci 33(11): 2147-2154.
- Scheiman M, Mitchell GL, Cotter S, Cooper J, Kulp M, et al. (2005) A Randomized Clinical Trial of Treatments for Convergence Insufficiency in Children. Arch Ophthalmol 123: 14-24.
- Bucci MP, Kapoula Z, Bui-Quoc E, Bouet A, Wiener-Vacher S (2011) Saccades and Vergence Performance in a Population of Children with Vertigo and Clinically Assessed Abnormal Vergence Capabilities. PLoS ONE 6(8): e23125.
- Bucci MP, Bui-Quoc E, Gerard CL (2013) The Effect of a Stroop-like Task on Postural Control in Dyslexic Children. PLoS ONE 8(10): e77920.
- Bucci MP, Seassau M, Larger S, Bui-Quoc E, Gerard CL (2014) Effect of visual attention on postural control in children with attention-deficit/hyperactivity disorder. Res Dev Disabil 35(6): 1292-1300.
- Berens C, Losey RR, Hardy LH (1927) Routine examinations of the ocular muscles and non-operative treatement. Am J Ophthalmol 10(12): 910-918.
- Wesson MD (1982) Normalization of prism bar vergences. Am J Optom Physiol Opt 59(8): 628-634.
- Scheiman M, Herzberg H, Frantz K, Margolies M (1989) A normative study of step vergence in elementary schoolchildren. J Am Optom Assoc 60(4):276-280.
- Rouse MW, Hyman L, Hussein M, Solan H (1998) Frequency of convergence insufficiency in optometry clinic settings. Convergence Insufficiency and Reading Study (CIRS) Group. Optom Vis Sci 75(2): 88-96.
- Von Noorden GK, Campos EC (2002) Binocular vision and ocular motility: theory and management of strabismus. (6th edtn), Mosby, St. Louis MO.
- Jimenez R, Perez MA, Garcia JA, Gonzalez MD (2004) Statistical normal values of visual parameters that characterize binocular function in children. Ophthalmic Physiol Opt 24(6): 528-542.
- Lyon DW, Goss DA, Horner D, Downey JP, Rainey B (2005) Normative data for modified Thorington phorias and prism bar vergences from the Benton-IU study. Optometry 76(10): 593-599.
- Espinasse-Berrod MA (2008) Strabologie, approches diagnostique et thérapeutique. (2nd edtn), Elsevier Masson.
- Radaković M, Ivetić V, Naumović N, Canadanović V, Stankov B (2012) Heterophoria and fusional convergence and divergence in preschool children. Med Glas (Zenica) 9(2): 293-298.
- Besnard M J (1973) Orthoptie pratique. Doin, Paris.
- Mellick A (1949) Convergence; An investigation into the normal standards of age groups. Br J Ophtalmol 33(12): 725-763.
- Péchereau A, Denis D, Speeg-Schatz C, Toesca E (2013) Insuffisance de convergence. In Strabisme: Rapport 2013 de la Société française d’ophtalmologie. Elsevier-Masson.
- Hugonnier R, Hugonnier S (1981) Strabismes: Hétérophories, paralysies oculo-motrices, les déséquilibres oculo-moteurs en clinique. Masson.
- Etezad Razavi M, Sagheb Hossein Poor S, Daneshyar A (2010) Normative Values for the Fusional Amplitudes and the Prevalence of Heterophoria in Adults (Khatam-Al-Anbia Eye Hospital-2009). Iran J Ophthalmol 22:41-46.
- Jeanrot N, Jeanrot F (2003) Manuel de strabologie: Aspects cliniques et thérapeutiques. Elsevier Masson.
- Morgan MW (1944) The clinical aspects of accommodation and convergence. Optometry & Vision Science 21(8): 301-313.
- Scheiman M, Wick B (2008) Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. Lippincott Williams & Wilkins.
- Scheiman M, Gallaway M, Frantz KA, Peters RJ, Hatch S, et al. (2003) Nearpoint of convergence: test procedure, target selection, and normative data. Optom Vis Sci 80(3): 214-225.
- Houghton S, Hunter SC, Rosenberg M, Wood L, Zadow C, et al. (2015) Virtually impossible: limiting Australian children and adolescents daily screen based media use. BMC Public Health 15(1): 5.
- Benedetto S, Drai-Zerbib V, Pedrotti M, Tissier G, Baccino T (2013) Ereaders and visual fatigue. PloS One 8(12): e83676.
- Alvarez TL, Vicci VR, Alkan Y, Kim EH, Gohel S, et al. (2010) Vision therapy in adults with convergence insufficiency: clinical and functional magnetic resonance imaging measures. Optom Vis Sci 87(12): E985-E1002.
- Sen DK, Malik SR (1972) Accommodative-convergence over accommodation (AC-A) ratio (in normal Indian subjects). Indian J Ophthalmol 20(4):153-157.
- Péchereau A, de Bideran M, Charlot JC, Clergeau G, Cordonnier M, Denis D, et al. (2003) Bases Cliniques de la Sensorio-Motricité Oculaire. Le strabisme accommodatif. FNRO éditions.
- Gratton I, Piccoli B, Pierini F, Bergamaschi A (1993) Mean-term variations of visual function of video display terminal operators: observations on 70 cases. Med Lav 84(6): 482 486.
- Van Leeuwen AF, Westen MJ, van der Steen J, de Faber JT, Collewijn H (1999) Gaze-shift dynamics in subjects with and without symptoms of convergence insufficiency: influence of monocular preference and the effect of training. Vision Res 39(18): 3095-3107.
- Jainta S, Bucci MP, Wiener-Vacher S, Kapoula Z (2011) Changes in vergence dynamics due to repetition. Vision Res 51(16): 1845-1852.
- Alkan Y, Biswal BB, Alvarez TL (2011) Differentiation between vergence and saccadic functional activity within the human frontal eye fields and midbrain revealed through fMRI. PLoS One 6(11): e25866.





