Conjunctival impression Cytology; An Aid in the Diagnosis of Dry Eye Syndromes
Soumya HV1*, Anita T Girish2, Gopinath GS3, Pandu S4
1 Assistant Professor, Department of Ophthalmology, JSS Medical College and Hospital, Mysore, Karnataka, India.
2 Associate Professor, Department of Ophthalmology, Mysore Medical College and Research Institute, Mysore, Karnataka, India.
3 Ex Professor and Head, Department of Ophthalmology, Mysore Medical College and Research Institute, Mysore, Karnataka, India.
4 Assistant Professor, Department of Ophthalmology, JSS Medical College and Hospital, Mysore, Karnataka, India.
*Corresponding Author
Soumya Harapanahalli Venkatesh
Assistant Professor, Department of Ophthalmology,
JSS Medical College and Hospital, Mysore-570004, Karnataka, India.
Tel: +919448116151
E-mail: drhvsoumya@yahoo.co.in
Received: September 13, 2016; Accepted: November 22, 2016; Published: November 24, 2016
Citation: Soumya HV, Anita T Girish, Gopinath GS, Pandu S (2016) Conjunctival impression Cytology; An Aid in the Diagnosis of Dry Eye Syndromes. Int J Ophthalmol Eye Res.4(10), 256-262. doi: dx.doi.org/10.19070/2332-290X-1600054
Copyright: Soumya HV© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Dry eye syndrome is a multifactorial disease of tears and ocular surface resulting in ocular discomfort, visual disturbances
and damage to the ocular surface with tear film instability. Diagnosis is based on symptom based assessment, clinical examination and tests like Schirmer’s, tear film break up time and Rose bengal staining of ocular surface. Conjunctival impression cytology (CIC) is a non-invasive, easy to perform test which can be used with other tests to diagnose dry eye. The present study aimed at evaluating the usefulness of impression cytology in the diagnosis of dry eye syndromes and to correlate the results of impression cytology with theiraetiology.
Materials and Methods: 150 eyes which met the inclusion criteria were subjected to clinical examination and diagnostic tests after obtaining informed consent. CIC samples were obtained from temporal bulbar conjunctiva and stained with periodic acid Schiff, Hematoxylin and eosin. The epithelial cell morphology was graded according to Nelson.
Results: The eyes showed normal, grade 1, grade 2 and grade 3 scores of CIC in 26(17.33%), 41(27.33%), 55(36.67%) and 28(18.67%) respectively. Abnormal CIC increased with declining schirmer’s, tear break up time values less than 10 seconds and increasing Rose Bengal staining. Thyroid ophthalmopathy and keratoconjunctivitis sicca were associated with severe while xerophthalmia was associated with mild cytological changes.
Conclusion: Diagnostic tests when used in combination are more effective than when used alone in dry eye. CIC, a noninvasive
and simple test can be used with other tests for the diagnosis and monitoring treatment of dry eye.
2.Introduction
3.Materials and Methods
3.1.Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Conjunctival Impression Cytology; An Aid in the Diagnosis of Dry Eye Syndromes.
Introduction
Dry eyes are one among the commonest presenting complaints to an ophthalmologist. Patients with dry eyes can be most demanding and frustrating since the condition is chronic and has to be treated indefinitely. The term 'dry eye' can be attributed to the Swedish ophthalmologist Henrik. S. C Sjogren, who described the triad of dry eye, dry mouth and joint pains in 1933 [1]. Michael A Lemp defined dry eye as “ The disorder of tear film due to tear deficiency or excessive tear evaporation which causes damage to the interpalpebral ocular surface and is associated with symptoms of ocular discomfort” [2-4]. More than 6% of population over 40 yrs of age suffer from dry eye, with the prevalence increased to 15% over the age of 65[5]. Dry eye syndromes can be broadly classified into tear deficient and evaporative types [2]. Aetiology include aqueous deficiency, Mucin deficiency, lipid abnormalities, lid surfacing abnormalities and epitheliopathy. The diagnosis of dry eye conditions essentially depends upon a thorough history which, unlike in other areas of ophthalmology has a pivotal rule [6]. The battery of tests available to diagnose dry eye include Schirmer’s tests, tear film break up time, staining of the tear film and conjunctival surfaces and laboratory assays of tear film osmolality and tear lysozyme which require technical expertise.
Conjunctival impression cytology using cellulose acetate filter paper is an innovative technique to study the viability and surface characters of conjunctiva [16]. Its use in research has experienced an enormous growth andhas greatly contributed to the understanding of ocular surface pathology [17].
Impression cytology was introduced in ophthalmology by Egbert et al., in 1977 and involves pressing and removing cellulose acetate filter paper on the ocular surface and staining the adherent cell layer and examination under microscope [7]. Impression cytology is used to differentiate ocular surface disorders according to their etiology, also provides a qualitative analysis of the light microscopic changes that occur in conjunctival morphology and also goblet cell density in dry eye states. Impression cytology has been used to study the ocular surface in keratoconjunctivitis sicca/ ocular cicatricial pemphigoid, irradiation, chemical burns, atopic disease, superior limbic keratoconjunctivitis, erythema multiforme and blepharitis. Nelson has graded impression cytological findings into four grades. Grade 0 comprising of small, round epithelial cells with abundant goblet cells, Grade 1 has slightly larger epithelial cells, decrease in number of goblet cells, Grade 2 has markedly decreased goblet cells with larger and polygonal epithelial cells. Grade 3 has cells with basophilic cytoplasm, small pyknotic nucleus and complete absence of goblet cells [8]. Nelson JD et al in their study showed that impression cytology from bulbar and palpebral surfaces of eyes from controls and with blepharoconjunctivitis were graded as 0 and 1 respectively. Eyes with keratoconjunctivitis sicca and primary ocular surface showed grade 2 and 3 changes. They showed that as the grading of the cytological changes increased in severity so did the basal tear secretions decreased [8]. Wittpen JR et al analysed the impression cytology of conjunctiva in preschool children with Vitamin A deficiency. They compared the pre-treatment and post treatment findings (children were treated with oral vitamin A). Specimens showed normal conjunctiva with goblet cells and epithelial cells which were deranged before treatment [9]. This suggested that impression cytology also helps us to evaluate therapeutic response in dry eye states.
Hence the present study aimed at evaluating the usefulness of impression cytology in the diagnosis of dry eye syndromes and to correlate the results of impression cytology with the aetiological causes of dry eye states.
Materials and Methods
A total of 150 eyes of 77 subjects were included in this prospective study which was conducted for a period of 2 years at a tertiary eye care hospital, southern part of Karnataka, India. Approval was obtained from the institutional ethics committee and prior informed consent was obtained from the study subjects. Patients with symptoms of dry eyes and also patients presenting with conditions like blepharoconjunctivitis, chemical burns, keratoconjunctivitis sicca and vitamin A deficiency were included in this study. Subjects who had undergone tarsorrhaphy, enucleation and patients with history of mechanical injuries of the eyeball were excluded.
Demographic, socio economic and other relevant data was obtained from all patients based on a proforma. After a detailed complete history, slit lamp examination of lid margins, tear meniscus, conjunctiva, cornea and tear film was done. Relevant examination of other important ocular structures and systemic examination was done. Schirmer’s tests, Rose bengal staining and tear film break up time (TFBUT) were performed in dim illumination. The tests were done with a 10 minute interval between each one in order to avoid discrepancies in the results and to minimise
ocular surface changes secondary to testing.
With the patient in the supine position, a drop of 4% lignocaine was instilled into the right eye. After inserting a wire speculum, cellulose acetate filter paper strips of pore size 0.45 μ (Sartorius AG, Germany) was cut into wedge shaped pieces and was applied on the temporal bulbar conjunctiva with a smooth edged forceps. The rough surface of paper was used. A smooth glass rod was used to press the paper gently. The strip was then removed with a peeling motion after 2-3 seconds. The strips were fixed with 95% ethanol and were examined after staining with Haematoxylin eosin and Periodic acid Schiff stains. The specimen was dehydrated and then mounted on a glass slide and examined under light microscope. The epithelial cell morphology was then graded according to standard criteria proposed by Nelson [8]. The inferior palpebral specimens were obtained in a similar way. The same procedure was repeated in the other eye. Goblet cell counting was difficult because of the lack of 200 or 400 compound grid microscopy.
Data was analysed using Graph pad Instat software.
Results
150 Cases of 77 patients were subjected to conjunctival impression.
cytology in this study. The youngest of the subjects was 8 and the oldest was of 75 years of age. Age distribution of the subjects is as shown (Figure 1). Out of 77 subjects, 29 were males and 48 were females (Figure 2). The female to male ratio was 1.65:1. The mean age of males and females was 38.5 and 47.8 years respectively.
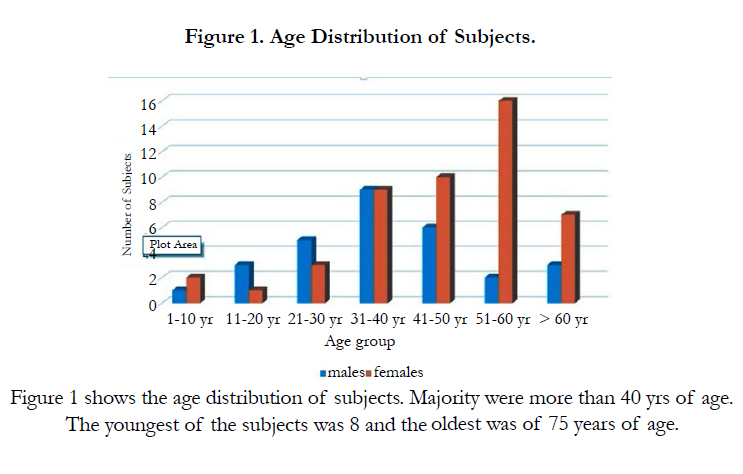
Figure 1. Age Distribution of Subjects.
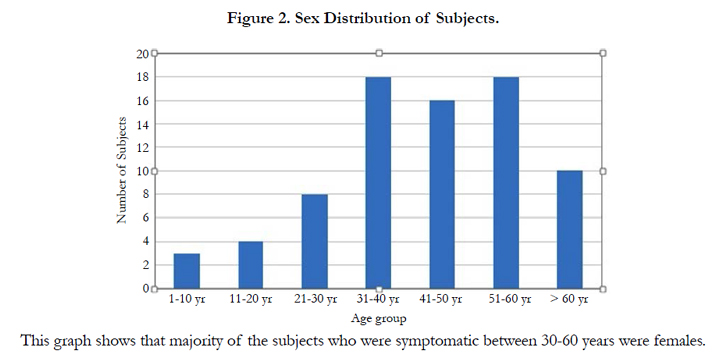
Figure 2. Sex Distribution of Subjects.
Out of 77 subjects, 27 (35.06%) were housewives, 15 (19.48%) were agriculturists and (10.38%) of them were officials.
Out of 150 eyes, 26 had grade 0, 41 had grade 1, 55 had grade 2 and 28 had grade 3 CIC changes. The cellular atypia increased with advancing age as shown in the table. (Table 1).
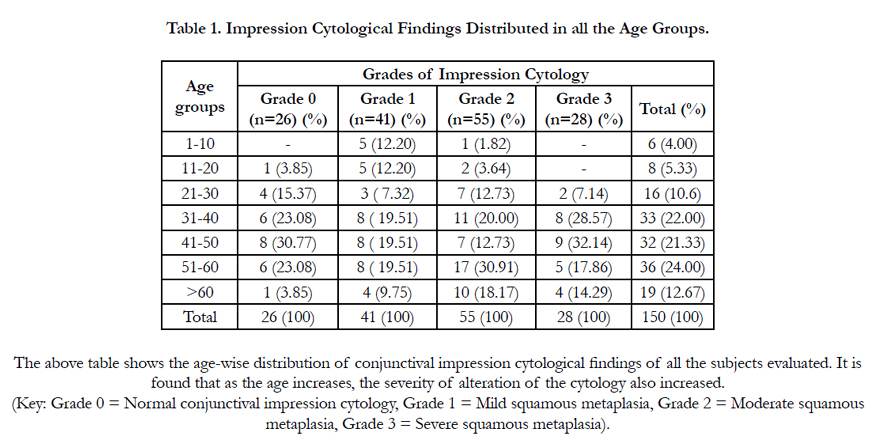

Table 1. Impression Cytological Findings Distributed in all the Age Groups.
Among the subjects examined, burning sensation and foreign body sensation were the commonest complaints in all the four grades of CIC (Table 2). The commonest signs were decreased tear meniscus height, xerosis and presence of mucus strands and debris. These were found in increasing number in patients with grade 3 changes (Table 3).
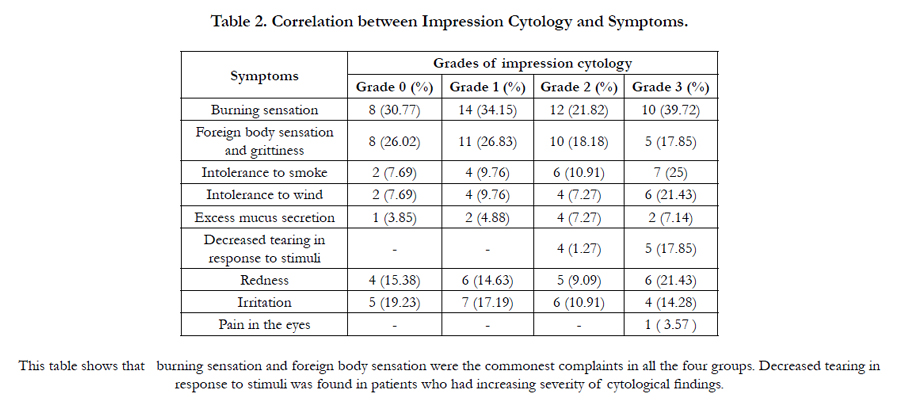
Table 2. Correlation between Impression Cytology and Symptoms.
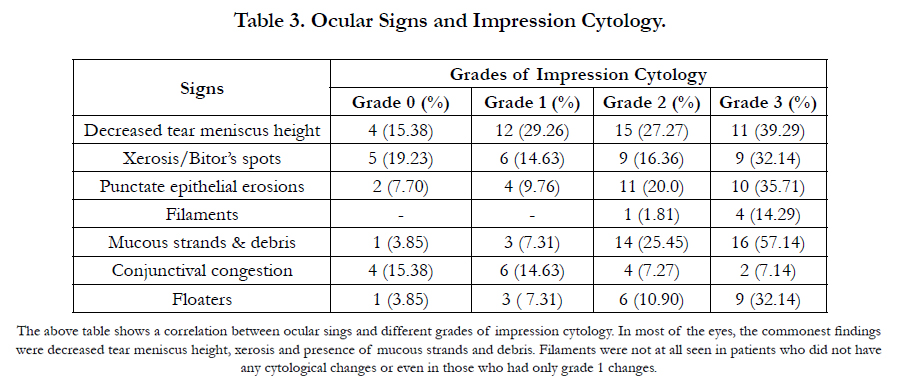
Table 3. Ocular Signs and Impression Cytology.
Schirmer’s tests scores between 0-5 mm were taken as positive, 6-10 mm as borderline and more than 10 mm negative. Based on these tests, 13 subjects (16.88%) showed scores less than or equal to 5 mm, 37 (48.05%) showed 6-10 mm and 27 (35.07%) had more than 10 mm.
Out of 150 eyes, 20 eyes (13.33%) had positive Schirmer’s test values (0-5mm) out of which 4 were of males and 16 were of females. The mean Schirmer’s test scores among males who had positive values was 3.4 mm. The mean Schirmer’s test scores among female patients who had positive values was 2.4 mm.
As the severity of the cytological changes increased, it was noted that there was a decline in the Schirmer’s test values (Figure 3).
The significance level estimated using ‘Fisher’s exact test’ comparing grade 0 and grade 3 impression cytology with positive Schirmer’s tests was statistically extremely significant (p<0.0001). With borderline Schirmer’s test scores, it was no significant. (p >0.05) and with negative Schirmer’s test scores it was significant.(p<0.01).
In this study, the TFBUT had a range of 1 second to 23.8 sec. The mean TBUT was 10.5 sec. 59 eyes had TBUT of less than 10 sec with a mean 6.6 sec. 91 eyes had TBUT of more than 10 sec with a mean 13.2 sec. Of the 26 eyes which had no cytological changes, only 4 of them had TBUT of less than 10 sec. The remaining 22 had TBUT values more than 10 sec with the mean value being 13.2 sec. Out of 41 eyes with grade 1 changes, 5 had TBUT values less than 10 sec and 36 had values more than 10 sec with the mean being 12.7 sec. Among the 55 eyes with grade 2 changes, 23 had TBUT values less than 10 sec and 32 had values more than 10 sec with the mean being 9.7 sec. Out of 28 eyes with grade 3 changes, 27 had TBUT values less than 10 sec and only one had value more than 10 sec with the mean being 6.3 sec.
TBUT values decreased progressively as the severity of impression cytology findings increased. TBUT values of less than 10 sec and more than 10 sec compared between grade 0 and grade 3 impression cytology groups were extremely significant (P <0.0001).
Out of 150 eyes, 87 showed some staining of the cornea and / or conjunctiva, 63 did not show any staining with Rose Bengal. Of the 87 eyes, 56 had van Bijstervald scores of less than 3.5 and 31 had scores more than 3.5 (indicative of dry eye). Number of eyes that stained with rose Bengal increased progressively as the severity of conjunctival impression cytology changes increased.
Discussion
A total of 150 eyes of 77 patients were taken up for the present study. All the patients were diagnosed based on the Schirmer’s tests, tear film break up time, rose Bengal staining and then the findings were confirmed by conjunctival impression cytology. The youngest patient in this study was 8 years old and the oldest was 60 years old with the mean being 44.36 years. The maximum numbers of patients were in the age group of 51-60 years.
In a study done by Khurana AK et al., [10] the youngest patient was [5] years old and the oldest was 78. The mean age of the present study (44.36 years) compared well with the mean age of the above mentioned study were in the age group of 60-69 years.
Out of 150 eyes of 77 patients, 26 eyes were grade 0. The remaining 124 had some changes out of which 41 showed grade 1, 55 showed grade 2 and 28 showed grade 3. Therefore 82.6% of the eyes showed some alteration in the cytology.
Nepalia et al., [11] studied the impression cytology in 60 patients who complained of dry eye symptoms. They found that the CIC of all the 120 eyes (100%) were abnormal. Only 8 (6.67%) had grade 1 changes while 44 (36.67%) had grade 2 and 68 (56.67%) had grade 3 changes. The findings in the present study cannot be compared with the study done by Nepalia et al., since the latter study segregated the subjects into controls and cases. Moreover, all the cases in the above study were selected after being examined for the presence or absence of dry eye unlike in the present study, which just included all the subjects complaining of symptoms of dry eye. Hence, the probability of finding abnormal conjunctival impression cytology is more in the study done by Nepalia et al., Out of 77 patients, 29 were males and 48 were females. The incidences of dry eyes were found to be more common in females than males, with the female to male ratio of 1.65:1. According to impression cytology, 124 of 150 eyes had abnormal changes. 40 were of males and 84 were of females. Based on impression cytology, the female to male ratio was 2.1:1.
The present study showed a higher female to male ratio reflecting the fact that dry eyes are more common among women similar to Khurana A K et al., [10], Moss S E et al., [12] and Lee S H et al., [13].
The symptoms with which the subjects presented were burning sensation, foreign body sensation, intolerance to wind, intolerance to smoke and redness of the eyes. All the grades of impression cytology were found in these patients. However grade 2 and 3 changes were more frequently associated with those subjects who complained of intolerance to wind, smoke, decreased tearing in response to stimuli and excess mucus secretion in the eyes.
Among the ocular signs, grade 2 and grade 3 changes were associated with mucus stands and debris, decreased tear meniscus height, punctuate epithelial erosions and floaters in the decreasing order of frequency. The non-specific signs of xerosis and conjunctival congestion were found in most of the patients. Filaments were associated only with grade 2 and grade 3 changes. Value of the Schirmer’s test in this study had a range from 0 to 25 mm with a mean of 10.46 mm. The mean Schirmer’s test scores of male subjects was 11.28 mm and the mean of females was 9.96 showing a decreased value in females.
The present study compared well with the Schirmer’s test values in grade 3 changes with Nelson J.D et al.,
The mean TBUT values of the eyes in this study that showed grade 0, 1, 2 and 3 changes were higher when compared with the study done by Nepalia et al., [11]. Some of the patients with dry eye syndromes, had a definite etiology for the same. Conjunctival impression cytology done in all the subjects, showed varying grades of squamous metaplasia according to the etiology. Thyroid ophthalmopathy, keratoconjunctivitis sicca and alkali burns were associated with more severe alteration of cytology suggesting multiple mechanisms for the occurrence of dry eyes, while cases of xerophthalmia were associated with mild changes (Table 4) .On palpebral conjunctival impression cytology, more number of eyes had grade 0 and grade 1 change and only 10 had grade 3 changes when compared to bulbar conjunctival impression cytology (Table 5). This could probably be due to more severe bulbar than palpebral involvement in most of the eyes.
Conclusion
The diagnosis of dry eye is empirically made on the basis of tests like Schirmer’s tests, tear film break up time and rose Bengal staining of the ocular surface. No single test by itself is useful in determining the etiology of dry eye. However, they are more sensitive and specific if performed in combination.
Conjunctival impression cytology (CIC) is a non-invasive, simple, very well tolerated and a reliable test to diagnose ocular surface changes in dry eye. This can be performed by people with little technical expertise and can be repeated many times in the same individual. This can also be used to assess the effect of treatment on dry eyes. It is a cost effective method which can be used even in a large series of patients.
However, this test carries the possibility of inter observer variations in its interpretation. Also, this test per se cannot be a confirmatory one for the diagnosis of dry eye.
Despite these shortcomings, conjunctival impression cytology is found to be much more useful compared to other tests especially when used in combination with them.
Conjunctival impression cytology offers a high development potential for the analysis of eye surface sebaceous carcinoma [18] and recently impressions of conjunctiva have been used for indirect immunofluorescence performedwith mouse immunoglobulin G1 (IgG1) anti-HLA-DR-α chain as primary monoclonal antibody [19].
References
- Brewitt H, Sistani F (2001) Dry eye disease: the scale of the problem. SurvOphthalmol 31(45): S199-202.
- Lemp A (1995) Report of the National Eye Institute/Industry Workshop on clinical trials in dry eyes. Eye Contact Lens. 21(4): 221-32.
- Pflugfelder SC, Solomon A, Stern ME (2000) The diagnosis and management of dry eye: a twenty-five–year review. Cornea. 19(5): 644-9.
- Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL (2000) Reliability and validity of the ocular surface disease index. ArchOphthalmol;118(5): 615-21.
- Pflugfelder SC. (2004) Antiinflammatory therapy for dry eye. Am J Ophthalmol; 137(2): 337-42.
- Nelson J (1982) Dry eye syndromes. Current Diagnosis and Management. Current practice in Ophthalmology: Mosby Year Book, Inc Missouri, Unite States of America. 49-67.
- Farris RL (1998) Abnormalities of the tears and treatment of dry eyes. The Cornea, (2nd edition) Newton: Butterworth Heinemann.
- Nelson JD, Havener VR, Cameron JD (1983) Cellulose acetate impressions of the ocular surface: dry eye states. Arch Ophthalmol; 101(12):1869-72.
- Wittpenn JR, Tseng SC, Sommer A (1986) Detection of early xerophthalmiaby impression cytology. Arch Ophthalmol; 104(2):237-9.
- Khurana AK, Choudhary R, Ahluwalia BK, Gupta S(1991) Hospital epidemiology of dry eye. Indian J Ophthalmol; 39(2):55.
- Nepalia LK (1999) Early and prompt diagnosis of dry eye states. Proceedings of All India Ophthalmological Society.
- Moss SE, Klein R, Klein BE (2000) Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 118(9):1264-8.
- Lee SH, Tseng SC (1997) Rosebengal staining and cytologic characteristics associated with lipid tear deficiency. Am JOphthalmol; 124(6):736-50.
- Haller-SchoberEM, Schwantzer G, Berghold A, FischlM, TheislA et al., (2006) Evaluating animpression cytology grading system (IC score) inpatients with dry eye syndrome. Eye (Lond); 20: 927-933.
- Zhu YF, Zheng LB, Yao YF (2016) Impression cytological study for ocular surface disorders of late stage eye burns .Eur. Rev. Med. Pharmacol. Sci.; 20(4): 605-12.
- Mocanu CL, Jurja S,Deca AG, Bîrjovanu F, Olaru A, et al., (2015) Impression conjunctival cytology in sicca syndrome-correlations between clinical and histological findings related to dry eye severity. Rom J MorpholEmbryol;57(1): 197-203.
- Calonge M, Diebold Y, Sáez V, Enríquez de Salamanca A,García-Vázquez C et al., (2004) Impressioncytology of the ocular surface: a review. Exp Eye Res, 78(3): 457–472.
- Sawada Y, Fischer JL, Verm AM, Harrison AR, Yuan C, et al (2003) Detection by impression cytologic analysis ofconjunctival intraepithelial invasion from eyelid sebaceous cell carcinoma. Ophthalmology, 110(10):2045–2050.
- Kawasaki S, Kawamoto S, Yokoi N, Connon C, Minesaki Y, et al., (2003) Up-regulated gene expression in theconjunctival epithelium of patients with Sjögren’s syndrome. Exp Eye Res 77(1):17–26.





