Microvascular Complications of Type 1 Diabetes Mellitus in an Adolescent: Case Report
Akil H1*, BuluŞ AD2, Andiran N2
1 Doheny Eye Institute, Los Angeles, California, USA.
2 Kecioren Training and Research Hospital, Pediatric Endocrinology Clinic, Ankara, Turkey.
*Corresponding Author
Handan Akil,
Doheny Eye Institute, Los Angeles,
California, USA.
E-mail: handanakil84@gmail.com
Received: September 10, 2015; Accepted: October 07, 2015; Published: October 12, 2015
Citation: Akil H, Bulus AD, Andiran N (2015) Microvascular Complications of Type 1 Diabetes Mellitus in an Adolescent: Case Report. Int J Ophthalmol Eye Res 03(9), 145-147. doi: dx.doi.org/10.19070/2332-290X-1500030
Copyright: Akil H© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Type 1 Diabetes Mellitus is a common chronic health problem with microvascular complications such as neuropathy, retinopathy and nephropathy in the pediatric population throughout the life. Screening of these complications should be done regularly, and appropriate preventive strategies should be followed. We present a 17 year old Type 1 diabetic patient who admitted to the hospital with the complaint of unhealed wound of his toe. An integrated and personal care of his clinical status revealed that he had diabetic microvascular complications including diabetic foot, neurogenic bladder, retinopathy, cataract and nephropathy.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Type 1 Diabetes Mellitus; Microvascular Complications; Neuropathy; Nephropathy; Retinopathy; Cataract.
Introduction
Type 1 diabetes mellitus is one of the most common chronic diseases characterized by insulin deficiency due to auto-destruction of pancreatic beta cells in pediatric patients. Glycemic control is still often poor in many children with Type 1 diabetes despite easier monitoring of blood-glucose, the appearance of pen devices for injection of insulin, and the introduction of new insulin types and regimens during the last decade. It has been demonstrated that hyperglycaemia plays a major role in development of microvascular complications including neuropathy, cataract, retinopathy and nephropathy in adolescents [1]. Identifying the role of risk factors will enable to set up better prevention programs that could result in improving patients' quality of life.
We report a 17 year old patient with uncontrolled Type 1 diabetes mellitus who developed diabetic foot, nephropathy, neurogenic dysfunction of bladder, cataract and pre proliferative retinopathy at the same time.
Case Report
A 17-year-old male patient with Type 1 DM had admitted to pediatric endocrinology clinic with a wound occurring in his left toe due to ingrown nail. In history, it was learned that he had been diagnosed with Type 1 DM 12 years ago (at the age of 5), he was put on regular + regular + mix insulin therapy. But the patient had not attended any follow-up visits, checked his blood sugar or used regular insulin for 5 years. The patient was the first child of thirddegree consanguineously married Turkish parents. The pregnancy and birth were uneventful. There was nothing significant in the family history.
Physical examination at the time of admission revealed a temperature of 35.7°C, a pulse of 66 beats per minute, a respiratory rate of 24, and a blood pressure of 100/70. His height was 147.9 cm (<3 percentile; -3, 64 SD) and a weight of 41.9 kg (<3 percentile;- 3,42 SD). He was in Tanner stage 5 of puberty and he had closed epiphyses.
He had claw hands on both sides. His left toe was enlarged with irregular nail whose lateral parts were inside the tissue; a hyperemic and a 3x2 cm ulcerated lesion was present (Figure 1). He had marked loss of sensation, starting from both toe tips and extending to the 1/3 of the lower leg and from finger tips to wrists.


Figure 1. Diabetic foot
Initial laboratory tests showed his blood sugar to be 310mg/dl, hemoglobin A1c to be 17.7%, blood urine nitrogen of 32 (5, 0 – 17, 9) mg/dl, creatinin of 0.9 (0.3-0.7) mg/dl. Hemogram, hepatic and renal functions were normal. Thyroid and celiac antibodies were normal. Urine showed micro albuminuria (1168.25 mg/day; normal range: 0-30 mg/day). Thyroid and adrenal gland function tests were normal.
- Electromyography (EMG) of lower and upper extremity was consistent with polyneuropathy.
- Echocardiography was normal.
- X ray of foot showed osteolytic lesions in the left toe.
- Antibiotic treatment was started, the necrotic wound was debrided and daily dressing was conducted. While a potential for progression to amputation was considered, he responded well to treatment.
A complete ophthalmologic consultation revealed adnexa and eye motility unaffected, best corrected visual acuity 0.8 (with snellen chart) in both eyes, and intraocular pressure 15 mmHg; a slit lamp observation of the anterior segment and fundus, performed in mydriasis, showed the presence of lens cortical opacities in both eyes (Figure 2), microaneurysms, superficial hemorrhages and cotton wool spots scattered in the fundus (Figure 3). Fundus fluorescein angiography confirmed these clinical findings and also showed late phase macular leakage from microaneurysms. These retinal findings were consistent with pre proliferative diabetic retinopathy.
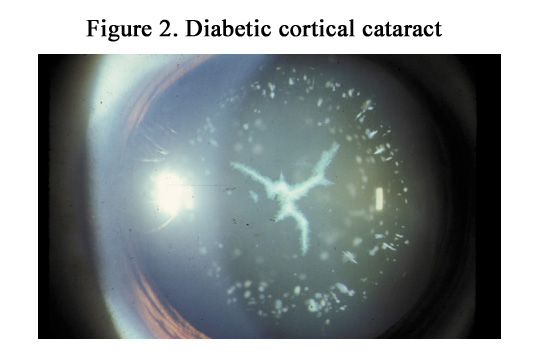
Figure 2. Diabetic cortical cataract
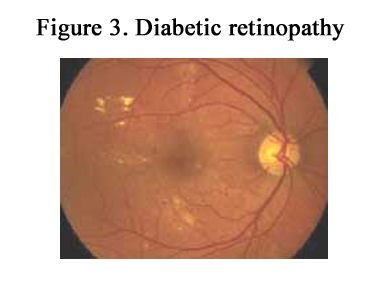

Figure 3. Diabetic retinopathy
The patient, who developed urinary retention and globus on the 2nd day, was detected to have a neurogenic bladder with a pine tree appearance on urography. Ultrasonography of the urinary tract showed a distended bladder with normal kidneys. Urodynamic study demonstrated an impaired bladder sensation, increased cystometric capacity and detrusor areflexia.
Treatment with amitriptyline, thioctacid and benexol tablet was started.
Insulin treatment was changed to insulin lispro (morning, noon, evening) and glargine insulin. The follow-up visit performed 3 months later revealed a HbA1c value of 9.2%. Neurogenic bladder showed improvement and the foot wound healed.
Discussion
Type 1 Diabetes is a major health problem for adolescents who have a long life expectancy. The complications should be prevented with the onset of Type 1 diabetes mellitus by working on risk factors. A new pediatric glycemic control target of HbA1c < 7.5% across all ages according to the American Diabetes Association [2]. An integrated and personalized approach would reduce the risk of development of microvascular complications in Type 1 Diabetes patients. The child with diabetes who receives limited care is more likely to develop long-term complications at an earlier age. We should pay attention to the screening for subclinical complications and early interventions with intensive therapy.
Diabetic neuropathy is the most common generalised sensorimotor polyneuropathy. It causes diffuse damage to all peripheral nerve fibers, motor, sensory and autonomic. Such damage occurs insidiously and progressively and is characterised at first by sensory loss and later by loss of motor function, in a stocking and glove distribution [3].
There is considerable uncertainty of the prevalence of diabetic neuropathy in the pediatric age group and the percentage of peripheral neuropathy ranges from 7 to 57 % in some epidemiological studies [1, 4]. This wide difference among the studies can be due to different diagnostic criteria and to the lack of consensus for the appropriate diagnostic criteria of neuropathy. Clinical symptoms of autonomic neuropathy generally do not occur until long after the onset of diabetes, but subclinical autonomic dysfunction can occur within 2 years in Type 1 Diabetes. The autonomic and sensory motor abnormalities may coexist and approximately 50% of people with peripheral neuropathy have asymptomatic autonomic involvement [5]. Children with diabetes are at greater risk of developing foot pathology such as foot ulcer, gangrene, and amputation than non-diabetic children, because of the sensory polyneuropathy. Many studies showed that the prevalence of the diabetic foot complications increased clearly with age and diabetes duration [6, 7]. Our male patient was diabetic for 12 years and he admitted to the clinic with a foot ulcer and high HbA1c which shows uncontrolled blood glucose levels. The gender effect on subclinical neuropathy in children with IDDM is also controversial [8]. The total and age-specific prevalence of foot ulcer, gangrene and amputation was significantly higher in males than females in some studies [9] and could be emphasized that, males are known to have limited joint mobility and higher foot pressure but the gender effect is not as prominent as the influence of age of onset, duration of illness, or glycemic control.
Other chronic diabetes complications, namely nephropathy, retinopathy were significantly associated with increased risk of diabetic foot ulcer, gangrene, and amputation due to the microangiopathic changes [7], which is also the same observation in our case. The importance of diabetic retinopathy as a significant independent risk factor that has to be taken into account during screening for foot problems in diabetic patients [9].
Early and regular neurophysiological tests for the measurement of subclinical disease are essential in this group of patients to identify high-risk individuals who may be candidates for more active intervention to prevent clinical disease [10].
Diabetic autonomic bladder dysfunction is a kind of diabetic polyneuropathy which is considered more prevalent in adults and elderly as a late complication of diabetes, can also occur in children early in the disease [11]. Urinary symptoms of a child or adolescent with poorly controlled diabetes should be cared in case of neurogenic bladder as seen in our case.
Generally, cataracts are uncommon in diabetic children and adolescents and are usually associated with prolonged poor metabolic control [12]. The pathogenesis is not fully understood. But recent studies have emphasized the polyol pathway, in which glucose is converted to sorbitol. In the lens, sorbitol is produced faster than it is converted to fructose; the increased accumulation of sorbitol creates a hyperosmotic effect that results in an infusion of fluid. The accumulation of intracellular sorbitol leads to osmotic changes resulting in the formation of cataracts [13]. Typical cataracts in diabetic children are characterized by anterior and/or posterior subcapsular or cortical ‘’snowflake’’ opacities. Our patient also had cortical opacities at presentation.
Diabetic retinopathy may be an early and serious complication of Type 1 Diabetes. In adolescence, the prevalence of diabetic retinopathy rises sharply after 2 years' duration of diabetes and almost all patients have developed some degree of retinopathy after 20 years' duration [14]. The progression may be rapid, especially in those with poor glycaemic control [1]. So adolescence is the time when efforts should be directed to screening for early signs of diabetic retinopathy and modifiable risk factors.
Minimum assessment for retinopathy should be done by ophthalmoscopy through dilated pupils. The frequency of retinopathy screening, in general, should occur annually but should be more frequent if there are high risk features for visual loss. Laser treatment reduces the rate of visual loss for vision-threatening retinopathy.
International Society for Pediatric and Adolescent Diabetes recommends that screening for retinopathy, neuropathy and nephropathy should start from the age of 11 years to after 2 years of having diabetes and from 9 years with 5 years duration in children [15].
Our patient had microalbuminuria despite the normal values of kidney function tests. Persistent microalbuminuria has been shown to predict the progression to end stage renal failure [16] and is associated with an increased risk of macrovascular disease.
Conclusion
In conclusion, a team approach is a must as diabetes is a complex condition, and different team members are needed each with a different focus varying from diabetic complications. The child with diabetes who receives limited care is more likely to develop long-term complications at an earlier age as in our case. Early intensive therapy can prevent microvascular complications.
References
- Diabetes Control and Complications Trial Research Group (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329(14): 977-986.
- Chiang JL, Kirkman MS, Laffel LM, Peters AL (2014) Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care 37: 2034-2054.
- Donaghue KC, Chiarelli F, Trotta D, Allgrove J, Dahl-Jorgensen K (2009) Microvascular and macrovascular complications associated with diabetes in children and adolescents. Pediatr Diabetes 10(Suppl 12): 195-203.
- Olsen BS, Nir M, Kjaer I, Vølund A, Mortensen HB (1994) Elevated vibration perception threshold in young patients with type 1 diabetes in comparison to nondiabetic children and adolescents. Diabet Med 11(9): 888-892.
- Trotta D, Verrotti A, Salladini C, Chiarelli F (2004) Diabetic neuropathy in children and adolescents. Pediatr Diabetes 5(1): 44-57.
- Shahi SK, Kumar A, Kumar S, Singh SK, Gupta SK, et al. (2012) Prevalence of Diabetic Foot Ulcer and Associated Risk Factors in Diabetic Patients From North India. The Journal of Diabetic Foot Complications 4(3): 83-91.
- Moss SE, Klein R, Klein BE (1992) The prevalence and incidence of lower extremity amputation in a diabetic population. Arch Intern Med 152(3):610-616.
- Duck SC, Wei FF, Parke J, Swick HM (1991) Role of height and glycosylated hemoglobin in abnormal nerve conduction in pediatric patients with type I diabetes mellitus after 4 – 9 yr of disease. Diabetes Care 14(5): 386-392.
- Bruun C, Siersma V, Guassora AD, Holstein P, de Fine Olivarius N (2013) Amputations and foot ulcers in patients newly diagnosed with type 2 diabetes mellitus and observed for 19 years. The role of age, gender and comorbidity. Diabet Med 30(8): 964-972.
- Lee SS, Han HS, Kim H (2010) A 5-yr follow-up nerve conduction study for the detection of subclinical diabetic neuropathy in children with newly diagnosed insulin-dependent diabetes mellitus. Pediatr Diabetes 11(8): 521-528.
- Solders G, Thalme B, Aguirre-Aquino M, Brandt L, Berg U, et al. (1997) Nerve conduction and autonomic nerve function in diabetic children. A 10 year follow-up study. Acta Paediatr 86(4): 361-366.
- Nabarro JD (1991) Diabetes in the United Kingdom: a personal series. Diabet Med 8(1): 59-68.
- Pollreisz A, Schmidt-Erfurth U (2010) Diabetic cataract- pathogenesis, epidemiology and treatment. J Ophthalmol 2010: 1-8.
- Goldstein DE, Blinder KJ, Ide CH, Wilson RJ, Wiedmeyer HM, et al. (1993) Glycemic control and development of retinopathy in youth-onset insulin-dependent diabetes mellitus. Ophthalmology 100(8): 1125-1132.
- Hanas R, Donaghue KC, Klingensmith G, Swift PG (2009) ISPAD Clinical Practice Consensus Guidelines 2009 Compendium. Pediatric Diabetes 10(Suppl 12): 1-2. Available on CD from www.ispad.org.
- Ruggenenti P, Remuzzi G (2007) Kidney Failure Stabilizes after a Two-Decade Increase: Impact on Global (Renal and Cardiovascular) Health. Clin J Am Soc Nephrol 2(1): 146-150.





