Plasminogen Activator Inhibitor Type 2 in Human Tears and Blood during Pregnancy
Steiber Z1, Tozser J2, Silver DM3, Jakab A4, Nemeth G1, Berta A1, Csutak A1*
1 Department of Ophthalmology, University of Debrecen, Faculty of Medicine, Debrecen, Hungary.
2 Department of Biochemistry & Molecular Biology, University of Debrecen, Faculty of Medicine Debrecen, Hungary.
3 Applied Physics Laboratory, Johns Hopkins University, Laurel, MD USA.
4 Department of Obstetrics and Gynecology, University of Debrecen, Faculty of Medicine, Debrecen, Hungary.
*Corresponding Author
Adrienne Csutak,
Department of Ophthalmology, University of Debrecen,
Faculty of Medicine Debrecen, 4012-Hungary, Debrecen,
Nagyerdei krt. 98.
Tel: 36-30-535-8975
Fax: 36-52-255-456
E-mail: acsutak@med.unideb.hu and acsutak@yahoo.com
Article Type : Research Article
Received: July 06, 2015; Accepted: August 22, 2015; Published: August 25, 2015
Citation: Csutak A, et al., (2015) Plasminogen Activator Inhibitor Type 2 in Human Tears and Blood during Pregnancy. Int J Ophthalmol Eye Res 03(7), 121-125. doi: dx.doi.org/10.19070/2332-290X-1500026.
Copyright: Csutak A© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium,provided the original author and source are credited.
Abstract
Purpose: During pregnancy, systemic blood levels of plasminogen activator inhibitors (PAIs), estradiol (E2) and progesterone (P4) are expected to rise with gestational age. This work examines whether a corresponding rise in PAIs occurs in tears. Methods: Tear and blood samples were collected opportunistically from women during pregnancy: PAI-2 and PAI-1 levels were measured using enzyme-linked immunosorbent assay (ELISA) tests. Blood levels of E2 and P4 were measured using chemiluminescence immunoassays.
Results: Levels of PAI-2 from tears of pregnant women did not increase and did not correlate with gestation. Levels of PAI-2, E2 and P4 in blood significantly increased over gestation. Tear PAI-2 levels did not correlate with blood levels of PAI-2, E2 or P4. Although blood levels of PAI-1 increased with gestation, tear levels of PAI-1 were below the ELISA detection limit, similar to the situation for non-pregnant subjects.
Conclusions: Tear PAI-2 levels are dissociated from the progression of pregnancy and the concomitant elevated systemic blood PAI-2, E2 and P4 levels, indicating the possibility of local control of proteolysis in the eye during pregnancy in the absence of wounding or surgery on the eye.
2.Introduction
3.Materials and Methods
3.1.Study Subjects
3.2.Sample Collection
3.3.Measurement of PAI-2 and PAI-1
3.4.Measurement of E2 and P4
3.5.Statistical methods
4.Results and Discussion
5.Acknowledgment and Declarations
6.References
Keywords
Gestation; Human Tears; Pregnancy; Proteolysis; Tear Enzymes.
Introduction
Plasminogen activator inhibitor Type 2 (PAI-2) was isolated 45 years ago as a human placental-derived inhibitor of urokinase plasminogen activator (uPA) [1]. The biological and clinical properties of PAI-2 have been extensively studied [2] and recognized to be important in fibrinolysis, wound healing and tissue remodeling. Nevertheless, the role of PAI-2 as a serine protease inhibitor (serpin) remains enigmatic with a variety of intracellular functions attributed to PAI-2, including its ability to influence apoptosis, cell differentiation, and immune response [3, 4].
In the absence of disease, wounding or surgery, plasma levels of PAI-2 are undetectable except during pregnancy when its presence in plasma is largely due to PAI-2 secretion by the trophoblast cells of the placenta [5]. The concentration of PAI-2 in plasma increases with gestational age until term and then returns to undetectable levels within six weeks after delivery [6, 7]. Independent of pregnancy, secreted or released PAI-2 has been identified in various biological fluids, including human tears [8], gingival fluid [9] and saliva [10].
Myopia has been becoming more prevalent worldwide [11, 12], especially in younger individuals and Asian populations in particular [13, 14]. Laser in situ keratomileusis (LASEK) and excimer laser photorefractive keratectomy (PRK) is often chosen to ameliorate myopia. Therefore corneal wound healing and the concomitant changes in tear enzymes that affect wound healing become important processes.
Women who became pregnant after LASEK have experienced changes in visual acuity and spherical equivalent [15]. Refractive regression and corneal haze have been reported in eyes of women who became pregnant after PRK for the treatment of myopia [16]. In rabbits, pregnancy has been identified as a risk factor for the development of corneal haze after PRK [17]. In addition, corneal thickness, curvature, and sensitivity as well as tear composition and refraction can all change during pregnancy [18, 19].
Pregnant women have been found to experience more gingivitis than non-pregnant women [20, 21]. Previous studies assessed the influence of pregnancy on the concentration of PAI-2 found ingingival crevicular fluid (GCF) [9, 22]. During pregnancy, levels of estradiol (E2) and progesterone (P4) rise with gestational age. E2 and P4 have been shown to have an inhibitory effect on PAI- 2 production in monocytes [23]. Pregnancy-related hormonal changes and levels of PAI-2 in gingival crevicular fluid (GCF) are thought to be responsible for aggravated gingival inflammatory symptoms during pregnancy [20, 21]. Sex hormone changes during different phases of the menstrual cycle have effects on gingival tissues and PAI-2 levels in GCF [24].
Two types of plasminogen activators exist: uPA and tissue-type plasminogen activator (tPA). The plasminogen activator cascade is controlled at different levels, one of which is the inhibition of plasminogen activator activity (PAA) by plasminogen activator inhibitors (PAIs). In addition to PAI-2, another PAI is plasminogen activator inhibitor Type 1 (PAI-1), which is produced by vascular smooth muscle cells, platelets and hepatocytes.
In the eye, uPA is a normal component of tear fluid, originating from conjunctival vessels and corneal epithelial cells [25]. Values of PAI-2 measured in tear samples (non-pregnancy) have been reported [8] and play a role in inhibition of uPA [26]. Levels of tPA and PAI-1 were below the detection limit of 4 ng/ml of the enzyme-linked immunosorbent assay (ELISA) test in normal (non-pregnancy) human tears [8].
Here, we have measured levels of PAIs in the tears of pregnant women at different gestational times and postnatal to determine if those levels are affected by pregnancy. It should be noted that changes in levels of PAIs in tears during pregnancy have not been examined previously. In addition, we measure E2, P4, PAI-1 and PAI-2 in blood of pregnant women.
Materials and Methods
Participants were selected for these studies after obtaining informed consent in adherence to the Declaration of Helsinki since the study protocol has been approved by the institute's committee on human research. The study subjects were under survey during pregnancy at the University of Debrecen, Department of Obstetrics and Gynecology.
In this study, both tear and blood samples were collected opportunistically from pregnant women during pregnancy and within 1 week after delivery. The ages of pregnant women were between 19-33 years, with a mean (SD) age of 27.42 (4.13) years. These were all full term (39-40 weeks, one at 37 weeks), normal pregnancies, without pre- or postnatal difficulties. None of the subjects had a history of hemostatic disorders or other relevant diseases. None were taking any medications. Two pregnant women were wearing contact lenses during pregnancy.
Tear samples were collected from the participants’ eyes at the outpatient clinic of the University of Debrecen Obstetrics and Gynecology Department. Samples consisted of tears collected with glass capillaries [27] from the lower tear meniscus (a horizontal thickening of the precorneal tear film by the lower margin) at the lateral canthus. We were careful not to touch the conjunctiva. Corneal injury or incision did not occur. We used the same,standardized collection method throughout the study. The duration of the sampling time was recorded and the secretion rate was calculated in μl/min (5-18 μl/min). Samples were centrifuged (1800 rpm) for 8-10 minutes right after collection and supernatants were deep-frozen at -80°C and were thawed only once for measurements.
For some participants, samples were obtained at successive obstetric visits. Where the volume of tear sample was sufficient, a duplicate determination was made and the results averaged to form a “measurement.” Tear sample determinations from 19 pregnant women yielded 56 measurements of tear PAI-2. Tear sample determinations from 13 pregnant women yielded 45 measurements of tear PAI-1.
Blood samples, 4 ml from the ulnar vein, were drawn, collected in tubes containing 0.5 ml 0.105 M Trisodium Citrate as anticoagulant, and put on ice. After centrifugation (1800 rpm, 10 minutes), plasma aliquots were tested for PAI-2, PAI-1, E2 and P4. Blood sample determinations from 25 pregnant women yielded 87 measurements of blood PAI-2 and from 10 pregnant women yielded 20 measurements of blood PAI-1. Blood sample determinations from 17 women yielded 51 measurements of blood E2 and P4.
ELISA tests (Imubind ELISA, American Diagnostica GmbH. Pfungstadt, Germany) were used to analyze the tear and blood samples for PAI-2 and PAI-1based on the manufacturer’s instructions. The lower detection limit was 100 pg/ml for PAI-2 and 4 ng/ml for PAI-1. Free PAI-2 and PAI-2 complexes, as well as free PAI-1 and PAI-1 complexes, are recognized with equal sensitivity.
For comparison purposes, we also report age-matched measurements of PAI-2 and PAI-1 in tears taken from non-pregnant women who participated in a previous study [8] conducted at the University of Debrecen Ophthalmology Department. For nonpregnant tear controls, tear samples from 17 non-pregnant women produced 17 tear PAI-2 measurements and tear samples from 5 non-pregnant women yielded 12 tear PAI-1 measurements.
E2 and P4 from blood samples were analyzed according to the manufacturer’s instructions using chemiluminescence immunoassays(Elecsys Estradiol CalSet II and Elecsys Progesterone II Cal-Set, Roche Diagnostics GmbH, Mannheim, Germany).
Standard statistical procedures were used to compare measurements between different time periods using t-tests for means with equal variances. Differences resulting in P < 0.05 were considered statistically significant. In addition, repeated measurement analysis of variance was used to assess the variation of PAI-2 levels within and between individuals over the gestation periods.
Results and Discussion
Figure 1 shows the measured mean values of PAI-2 in tears of pregnant women. The differences between mean values are not statistically significant for the different time periods of measurement. Hence, the trend line is essentially flat. The non-pregnant mean value (SD) of measurements taken from our previous study was 26.7 (20.5) and the differences between it and each of the values represented in Figure 1 were not statistically significant.
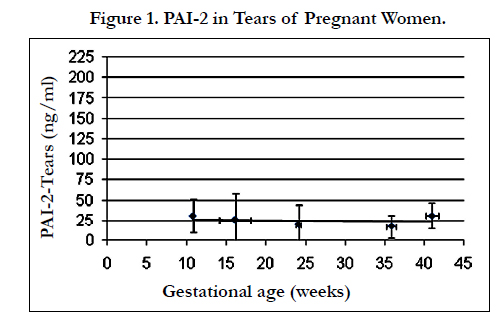
Figure 1. PAI-2 in Tears of Pregnant Women
PAI-2 levels in tear samples during pregnancy. The vertical error bars represent one standard deviation from the mean PAI-2 concentration.The horizontal error bars represent one standard deviation from the mean gestation time in weeks. The trend line is y = -0.11 x + 27.9, with R2= 0.050.
Figure 2 presents mean values of PAI-2 from blood samples of pregnant women. Here the difference between week 10.7 mean values and week 41(post-partum) mean value is not statistically significant. However, there is a steep rise in the mean value of the PAI-2 seen at week 16.1, week 24.2, and week 34.9, with statistically significant differences between each of these and week 10.7 and week 41 mean values. This is represented by a rising quadratic trend.
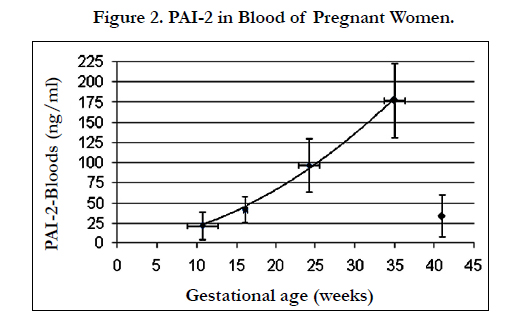
Figure 2. PAI-2 in Blood of Pregnant Women.
PAI-2 levels in blood samples during pregnancy. The vertical error bars represent one standard deviation from the mean PAI-2 concentration. The horizontal error bars represent one standard deviation from the mean gestation time in weeks. The trend during gestation is y = 0.12 x2 + 0.87 x, with R2= 0.997.
Repeated measurement analysis of variance was performed on the PAI-2 measurements. For PAI-2 levels in tears, the variance of measurements taken from different participants was 4.95 times greater than the variance within the individual participant’s measurements over the five gestation periods. This represents a statistically significant difference, p < 0.01, between the measurements taken from different participants. For PAI-2 levels in blood, the variance ratio was 1.06 for the variance within an individual participant’s measurements over the five gestation periods versus between participants. Here there was not a statistically significant difference, p = 0.41, between the measurements taken from different participants.
Considering the variance of measurements between gestation periods versus the variance from measurements from all participants at each of the five gestation periods, the variance ratio was 1.66 for PAI-2 in tears representing no statistically significant difference, p = 0.30, between measurements taken at the different gestation periods. For PAI-2 in blood, the variance ratio was 1493.43 representing a statistically significant difference, p < 0.001, between the measurements taken at different gestation periods.
All of the tear PAI-1 measurements, across the span of gestation, postnatal and non-pregnant subjects (20 pregnant and 12 nonpregnant measurements) were below the 4 ng/ml detection limit of the ELISA kit. Therefore, due to the limit of sensitivity of our testing regime, PAI-1 levels were not seen to be significantly increased in tears due to pregnancy. A more sensitive test will be required to further investigate this situation [28]. The blood PAI- 1 measurements yielded mean values (SD) of 85.8 (29.0), 90.5 (32.2) and 125.9 (26.1) ng/ml at 11, 16 and 24 weeks gestation. Since PAI-1 was not at detectable levels in tears, this cannot be a basis for tear-blood comparison of PAI-1 levels.
Figures 3 and 4 present mean values of E2 and P4, respectively, from blood samples of pregnant women. In both figures, there is a steep rise in mean values with gestation.
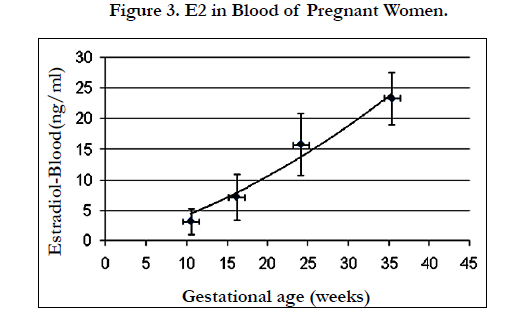
Figure 3. E2 in Blood of Pregnant Women.
E2 levels in blood samples during pregnancy. The vertical error bars represent one standard deviation from the mean PAI-2 concentration. The horizontal error bars represent one standard deviation from the mean gestation time in weeks. The trend is y = 0.01 x2 + 0.33 x, with R2= 0.971.
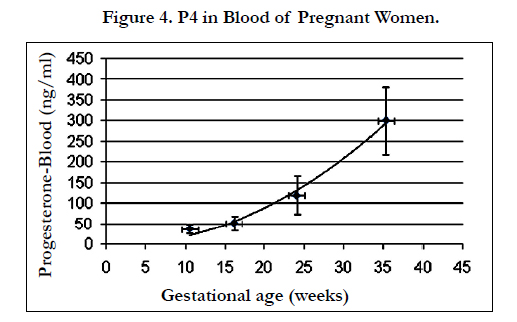
Figure 4. P4 in Blood of Pregnant Women.
E2 levels in blood samples during pregnancy. The vertical error bars represent one standard deviation from the mean PAI-2 concentration. The horizontal error bars represent one standard deviation from the mean gestation time in weeks. The trend is y = 0.01 x2 + 0.33 x, with R2= 0.971.
Normal pregnancies are associated with major changes in all aspects of hemostasis [29, 30]. Thrombosis is rare in the first trimester but coagulation due to a decrease of fibrinolytic activity is enhanced during pregnancy, especially in the second and third trimester. Thus normal pregnancy presents as a hypercoagulable state. This condition protects pregnant women from fatal hemorrhage during delivery, but predisposes them to thromboembolism. The coagulation activity is balanced despite large changes in blood levels of tPA, uPA, PAI-1 and PAI-2 [31, 32] in normal pregnancy. This balance and change are needed to make uterine artery and umbilical artery hemodynamics more baby-friendly (i.e. high flow, low resistance) with increasing gestational age and to ensure that the delivery is not fatal for the mother. The proteolytic activity of the human body, including this function of PAI in tears, is under sensitive control and serious complications may occur if this system is disturbed.
One observation from our study (Figure 1) is that PAI-2 levels in tears of pregnant women are not higher than the levels found in non-pregnant women and are not correlated with gestational age (R2 = 0.050). Another observation (Figure 2) is that PAI-2 levels in blood showed a continuous increase through the duration of pregnancy, with a quadratic trend with respect to gestation age (R2 = 0.997). The analysis of variance results give further validation to these observations by showing that the error bars in Figure 1 do not hide a potential rhythmic trend of PAI-2 in tears in each woman.
The PAI-2 levels in blood, rising with gestational age, are significantly higher than the mean PAI-2 values measured in tears. Thus the PAI-2 levels in tears are not correlated with blood PAI-2 levels and not driven by the increased systemic levels of PAI-2 in the blood stream. Also, although the E2 and P4 values increase with gestation (Figures 3 and 4), the tear PAI-2 values are not correlated with these hormone levels. These results suggest that PAI-2 levels in tears and PAI-2 regulated proteolysis at the ocular surface are under local control.
Although pregnancy is a risk factor for the development of corneal haze after PRK [17], our measurements on tears of pregnant women indicate that tear PAI-2 is not elevated during pregnancy in the absence of wounding or surgery. However, if the ocular surface is wounded or undergoes surgery, local PAI-2 elevating mechanisms could be more effective during pregnancy than in the absence of pregnancy, especially if these local mechanisms were stimulated by increased systemic PAI-2 levels during pregnancy.
In pathological conditions, after wounding or following surgery, the permeability of conjunctival blood vessels generally grows, thereby pro-enzyme forms of proteases and protease inhibitors may appear in tears via transudation [33]. In addition to tear specific proteins, serum proteins, such as albumin, transferrin and IgG, can also be present in tears [34]. Furthermore, increases of PAI levels in tears may occur due to release from complexes in the tear fluid or from damaged epithelial cells at the ocular surface. Conjunctival epithelial cells and systemic hormone levels can also affect corneal conditions [35]. These are local mechanisms that could raise the levels of PAIs in tears as a response to pathological conditions and cause incomplete wound healing.
The common carotid artery separates into internal and external carotid arteries as it supplies blood to the head and neck. The ophthalmic artery is a branch of the internal carotid and supplies blood to the brain and eyes. The maxillary artery is a branch of the external carotid and supplies the cheek mucosa, teeth, gingivae, and palate. The degree of systemic influence or isolation from the biochemical constituents in the carotid blood stream could differ in the eye (tear constituents) and mouth (GCF constituents) depending on differences in the properties of the internal and external carotid systems. The independence of PAI-2 levels in tears and GCF from the progression of pregnancy might indicate the possibility of tight junction barriers to the elevated systemic blood composition levels.
In general, performing surgery on pregnant women is not recommended [36]. For refractive surgery, waiting three months is suggested after giving birth and/or breastfeeding because of hormonal changes that can affect the refractive error and possibly induce effects on corneal wound healing. However in some cases, pregnant women undergo corneal surgeries, typically because of traumatic causes or when pregnancy was not identified in its early stage [15, 16].
Some knowledge of the enzymatic changes during pregnancy might help to improve our understanding [37, 38]. Further research into this complex system is necessary so that ophthalmic interventions and surgeries, which may become necessary during pregnancy, can be performed with greater safety and with reduced risk of postoperative complications.
Acknowledgment and Declarations
The authors declare that there is no conflict of interests regarding the publication of this paper.This work was supported in part by the European Union, co-financed by the European Social Fund, under project TAMOP-4.2.2.A-11/1 KONYV-2012-0045. AC was the recipient of a Bolyai and a Szodoray Grant. Partial presentation at EVER conference, 11 October 2012.
References
- Kawano T, Morimoto K, Uemura Y (1970) Partial purification and properties of urokinase inhibitor from human placenta. J Biochem 67(3): 333-342.
- Kruithof EK, Baker MS, Bunn CL (1995) Biological and clinical aspects of plasminogen activator inhibitor type 2. Blood 86(11): 4007-4024.
- Lee JA, Cochran BJ, Lobov S, Ranson M (2011) Forty years later and the role of plasminogen activator inhibitor type 2/SERPINB2 is still an enigma. Semin Thromb Hemost 37(4): 395-407.
- Medcalf RL (2011) Plasminogen activator inhibitor type 2: still an enigmatic serpin but a model for gene regulation. Methods Enzymol 499: 105-134.
- Astedt B, Lindoff C, Lecander I (1998) Significance of the plasminogen activator inhibitor of placental type (PAI-2) in pregnancy. Semin Thromb Hemost 24(5): 431-435.
- Koh CL, Viegas OA, Yuen R, Chua SE, Ng BL, et al. (1992) Plasminogen activators and inhibitors in normal late pregnancy, postpartum and in the postnatal period. Int J Gynaecol Obstet 38(1): 9-18.
- Coolman M, de Groot CJ, Steegers EA, Geurts-Moespot A, Thomas CM, et al. (2006) Concentrations of plasminogen activators and their inhibitors in blood preconceptionally, during and after pregnancy. Eur J Obstet Gynecol Reprod Biol 128(1-2): 22-28.
- Csutak A, Silver DM, Tőzsér J, Steiber Z, Bagossi P, et al. (2008) Plasminogen activator inhibitor in human tears after laser refractive surgery. J Cataract Refract Surg 34(6): 897-901.
- Kinnby B, Matsson L, Åstedt B (1996) Aggravation of gingival inflammatory symptoms during pregnancy associated with the concentration of plasminogen activator inhibitor type 2 (PAI-2) in gingival fluid. J Periodontal Res 31(4): 271-277.
- Virtanen JO, Sirén V, Multanen J, Färkkilä M, Leivo I, et al. (2006) Plasminogen activators and their inhibitors in human saliva and salivary gland tissue. Eur J Oral Sci 114(1): 22-26.
- Pan CW, Ramamurthy D, Saw SM (2012) Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt 32(1): 3-16.
- Morgan IG, Ohno-Matsui K, Saw SM (2012) Myopia. Lancet 379(9827): 1739-1748.
- Shimizu N, Nomura H, Ando F, Niino N, Miyake Y, et al. (2003) Refractive errors and factors associated with myopia in an adult Japanese population. Jpn J Ophthalmol 47(1): 6-12.
- Saw SM, Katz J, Schein OD, Chew SJ, Chan TK (1996) Epidemiology of myopia. Epidemiol Rev 18(2): 175-187.
- López-Prats MJ, Hidalgo-Mora JJ, Sanz-Marco E, Pellicer A, Perales A, et al. (2012) Influence of pregnancy on refractive parameters after LASIK surgery. Arch Soc Esp Oftalmol 87(6): 173-178.
- Sharif K (1997) Regression of myopia induced by pregnancy after photorefractive keratectomy. J Refract Surg 13(5 Suppl): S445-S446.
- Csutak A, Silver DM, Tőzsér J, Hassan Z, Berta A (2004) Urokinase-type plasminogen activator to prevent haze after photorefractive keratectomy, and pregnancy as a risk factor for haze in rabbits. Invest Ophthalmol Vis Sci 45(5): 1329-1333.
- Barbazetto IA, Pizzarello LD (2007) Ocular changes during pregnancy. Compr Ophthalmol Update 8(3): 155-167.
- Pizzarello LD (2003) Refractive changes in pregnancy. Graefes Arch Clin Exp Ophthalmol 241(6): 484-488.
- Yin X, Bunn CL, Bartold PM (2000) Detection of tissue plasminogen activator (t-PA) and plasminogen activator inhibitor 2(PAI-2) in gingival crevicular fluid from healthy, gingivitis and periodontitis patients. J Clin Periodontol 27(3): 149-156.
- Kinnby B (2002) The plasminogen activating system in periodontal health and disease. Biol Chem 383(1): 85-92.
- Buduneli N, Becerik S, Buduneli E, Baylas H, Kinnby B (2010) Gingival status, crevicular fluid tissue-type plasminogen activator, plasminogen activator inhibitor-2 levels in pregnancy versus post-partum. Aust Dent J 55(3):292-297.
- Kinnby B, Åstedt B, Casslen B (1995) Reduction of PAI-2 production in cultured human peripheral blood monocytes by estradiol and progesterone – No effect on t-PA, u-PA and PAI-1. Fibrinolysis 9(3): 152-156.
- Becerik S, Özçaka Ö, Nalbantsoy A, Atilla G, Celec P, et al. (2010) Effects of menstrual cycle on periodontal health and gingival crevicular fluid markers. J Periodontol 81(5): 673-681.
- Hayashi K, Sueishi K (1988) Fibrinolytic activity and species of plasminogen activator in human tears. Exp Eye Res 46(2): 131-137.
- Williams DL, Risse B, Kim S, Saunders D, Baker MS, et al. (1999) Plasminogen activator inhibitor type 2 in human corneal epithelium. Invest Ophthalmol Vis Sci 40(8): 1669-1675.
- van Haeringen NJ, Glasius E (1976) The origin of some enzymes in tear fluid, determined by comparative investigations with two collection methods. Exp Eye Res 22(3): 267-272.
- Zhang X, Dimeski G, Punyadeera C (2014) Validation of an immunoassay to measure plasminogen-activator inhibitor-1 concentrations in human saliva.Biochem Med 24(2): 258-265.
- Brenner B (2004) Haemostatic changes in pregnancy. Thromb Res 114(5-6): 409-414.
- Hui C, Lili M, Libin C, Rui Z, Fang G, et al. (2012) Changes in coagulation and hemodynamics during pregnancy: a prospective longitudinal study of 58 cases. Arch Gynecol Obstet 285(5): 1231-1236.
- Kruithof EKO, Tran-Thang C, Gudinchet A, Hauert J, Nicoloso G, et al. (1987) Fibrinolysis in Pregnancy: A study of plasminogen activator inhibitors. Blood 69(2): 460-466.
- van Wersch JW, Ubachs JM (1991) Blood coagulation and fibrinolysis during normal pregnancy. Eur J Clin Chem Clin Biochem 29(1): 45-50.
- Kosugi T, Takagi I, Kinjo K, Sueno K, Noda K, et al. (1984) Interaction of fibrinolytic activity between the tracheobronchial secretion and circulating blood of rats. Laryngoscope 94(3): 386-390.
- Gachon AM, Richard J, Dastugue B (1982) Human tears: Normal protein pattern and individual protein determinations in adults. Curr Eye Res 2(5): 301-308.
- Gagliano C, Caruso S, Napolitano G, Malaguarnera G, Cicinelli MV, et al. (2014) Low levels of 17-β-oestradiol, oestrone and testosterone correlate with severe evaporative dysfunctional tear syndrome in postmenopausal women: a case-control study. Br J Ophthalmol 98(3): 371-376.
- Bower KS, Woreta F (2014) Update on contraindications for laser-assisted in situ keratomileusis and photorefractive keratectomy. Curr Opin Ophthalmol 25(4): 251-257.
- Reeves SW, Davis EA, Dana MR (2008) Pregnancy and the eye: Principles and Practice of Ophthalmology. (3rd edtn), Saunders-Elsevier, Philadelphia.
- Ness T, Paulus W (2010) Eye and pregnancy. Ophthalmologe 107(9): 863- 872.





