Profile of Secondary Glaucoma in A Semi Urban Tertiary Health Care Hospital In Nigeria
Ajite KO, Fadamiro C.O, Ajayi I.A, Omotoye O.J
Ekiti State University Teaching Hospital, Nigeria.
*Corresponding Author
Kayode Ajite,
Ekiti State University Teaching Hospital,
Nigeria.
Tel: +2348033799766
E-mail: bidemi_kayode@yahoo.com
Article Type: Review Article
Received: November 16, 2014; Accepted: March 24, 2015; Published: March 25, 2015
Citation: Ajite KO, Fadamiro C.O, Ajayi I.A, Omotoye O.J (2015) Profile of Secondary Glaucoma in a Semi Urban Tertiary Health Care Hospital In Nigeria. Int J Ophthalmol Eye Res 03(3), 97-100. doi: dx.doi.org/10.19070/2332-290X-1500019
Copyright: Ajite KO© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Glaucoma is the second-most-frequent cause of blindness in the world. Most primary glaucomas are managed by early diagnosis and treatment however secondary glaucomas differ from primary by the fact that, if the primary pathology is treated properly and the possibility of secondary glaucoma is kept in mind, glaucomatous damage can be easily prevented. This study is aimed at determining the prevalence and pattern of secondary glaucoma, the knowledge of which will help in reducing the glaucoma blindness.
Methods: A retrospective review of medical records of all consecutive newly diagnosed glaucoma patients attending the eye clinic of Ekiti state university teaching hospital,(Eksuth) Ado Ekiti, from January 2011 to December 2012 were selected for the study. Each patient had a complete ophthalmic evaluation, including relevant history, visual acuity testing, slit-lamp examination, applanation tonometry, gonioscopy with a 4mirror goniolens and standard automated perimetry. Data collected was collated and analyzed using SPSS version 16 (SPSS, Inc, Chicago, USA). Frequencies and means were generated to observe patterns of variable distribution among the patients.
Result: A total of 5655 new patients attended the eye clinic during the study period, 1660(29.4%) were diagnosed with glaucoma out of which primary glaucoma were 1561(94.0%) while secondary were 99(6.0%). The spectrum of secondary glaucoma were post traumatic glaucoma 25(25.2%), lens related glaucoma 16(16.2%), steroid induced glaucoma 14(14.2%), neovascular glaucoma 12(12.1%), uveitic glaucoma 10(10.1%), pseudoexfoliation glaucoma 10(10.1%), pigmentary glaucoma 6(6.1%), aphakic glaucoma 6(6.1%).
Conclusion: Post traumatic secondary glaucoma has the highest frequency of occurrence and as with others, requires prompt diagnosis and treatment which may help significantly in preventing resultant visual impairment and blindness.
2.Background Information on Study Location
3.Methods
4.Results
5.Discussion
6.Conclusion
7.References
Introduction
Glaucoma is the second-most-frequent cause of blindness in the world, with a total of 5.2 million blind people as a result of this disease; 80% live in developing countries [1]. Glaucoma is responsible for 16% of blindness in Nigerian adults and the foremost cause of irreversible blindness among Nigerian adults [2]. In a multicentre study involving 2 tertiary eye institutions, 7 secondary eye centres with eye care facilities in Lagos, a total of 6240 patients visited the outpatient department over the 4-week period, out of which 1577 (25.3%) were glaucoma patients [3]. Glaucoma visits constitute a significant proportion of eye clinic visits and substantial manpower, infrastructure, and equipments are usually mobilized for its optimal management [3]. Glaucoma can be primary or secondary. Secondary glaucoma is a form of glaucoma in which the aetiology is traceable to an ocular or systemic pathology. Secondary glaucoma refers to any form of glaucoma in which there is an identifiable cause of increased intraocular pressure (IOP) resulting in optic nerve damage with or without vision loss [4]. As with primary glaucoma, secondary glaucoma can be of open angle or angle closure type which can be unilateral or bilateral. Most primary glaucomas are managed by early diagnosis and treatment however secondary glaucomas differ from primary by the fact that, if the primary pathology is treated properly and the possibility of secondary glaucoma is kept in mind, glaucomatous damage can be easily prevented [4]. Early detection of the risk factors and aetiology of secondary glaucoma can help to avoid progression of this disease. Ocular trauma, cataract, diabetic, hypertension and infectious uveitis represent special risks for developing secondary glaucoma [1].
Strohl et al [1] in Paraguay reported the prevalence of secondary glaucoma to be 20.8% with post traumatic glaucoma the highest frequency while report from India indicates 21.8% and post vitrectomy glaucoma occurring with the highest frequency [4]. In a report by Kyari, in Tanzania, prevalence of secondary types of glaucoma was 4.16% (CI 3.5-4.9%) [5].
However in China, according to a study by Foster and Johnson [6], it was estimated that 9.4 million people aged 40 years and older in China have glaucomatous optic neuropathy. Of this number, 5.2 million (55%) are blind in at least one eye and 1.7 million (18.1%) are blind in both eyes. Primary angle closure glaucoma (PACG) is responsible for the vast majority (91%) of bilateral glaucoma blindness in China. Secondary glaucoma was 4.2% [6]. Furthermore, Foster PJ et al in another study [7] reported the prevalence of secondary glaucoma in Chinese residents of Singapore, Tanjong Pagar district to be as high as 16%. In relation to blindness, prevalence surveys suggest that glaucoma blindness is more common in cases of angle closure glaucomaand secondary angle closure glaucoma than in chronic open angle glaucoma [8, 9]. Late presentation of patients with secondary glaucoma has been identified as possible risk factor contributing to development of severe visual impairment and blindness [10]. The prevalences of morbidity and visual impairment due to primary open angle and angle-closure glaucomas have been fairly well established by population surveys in the west and, recently, in the developing world, the issue of blindness from secondary glaucomas has received little attention from most investigators [11]. Individuals with secondary glaucoma tend to report promptly to the ophthalmologist since there is often marked reduction in visual acuity, apart from pain and ocular discomfort [11]; as a consequence, these are largely self-reported [11]. Information on secondary glaucomas in published eye surveys is limited and the cause of glaucoma seldom identified [12]. This study is aimed at determining the prevalence and pattern of secondary glaucoma, the knowledge of which will help in reducing the glaucoma blindness and formulating important health education strategy.
Background Information on Study Location
The Ekiti state teaching hospital is semi urban tertiary hospital such that patients are first seen at the general outpatient department (GOPD) after initial “once and for all” consultation fee has been paid. Thereafter the patients with ophthalmic complaints/ diagnosis are referred to the Comprehensive Ophthalmologist who then sends to subspecialties as deemed fit in the hospital at no additional cost. The access is not limited by any hospital bureaucratic processes. The rural and the city dwellers have equal and unfettered access to the ophthalmologist/glaucoma specialist who runs the clinic twice a week. The implication of this is that all the patients that were needed to be seen for the purpose of this study were seen without any bias.
Methods
A retrospective review of medical records of all consecutive newly diagnosed glaucoma patients attending the eye clinic of Ekiti state university teaching hospital, (Eksuth) Ado Ekiti, from January 2011 to December 2012 were selected for the study. Each patient had a complete ophthalmic evaluation, including relevant history, visual acuity testing, slit-lamp examination, applanation tonometry, gonioscopy with a 4mirror goniolens and standard automated Perimetry. Patients with previous trabeculectomy surgery and corneal pathologies precluding gonioscopy were excluded. They all had thorough ocular examinations, intraocular pressure measured with applanation tonometer, central cornea thickness, optic disc evaluation with +78D lens, gonioscopy. The patients were classified as open angle or angle closure, primary or secondary glaucoma based on history, slit lamp biomicroscope examination findings, gonioscopic findings and biomicroscopic fundus examination. Secondary glaucoma was diagnosed when the following criteria were met: a positive history and ocular findings of pathologies such as trauma, previous ocular surgery (not trabeculectomy), neovascularisation, inflammation, or any other abnormal ocular or systemic findings that could have caused prior or current IOP elevation. Patients with unilateral glaucoma were included as secondary glaucoma only if the other eye had no evidence or family history of a primary glaucoma. The other eye had IOP, gonioscopy and fundus evaluation and if required diurnal variation and visual field to exclude primary glaucoma.
Secondary glaucoma was diagnosed in the presence of above history and chronically raised IOP ≥ 22 mmHg with or without glaucomatous optic neuropathy (cupped disc ratio (CDR≥ 0.7). Exfoliative glaucoma (XFG), a form of secondary glaucoma was defined as glaucoma (open angle or closed angle) associated with characteristic exfoliation material on the anterior lens surface on slit lamp biomicroscopy in addition to any of the following on gonioscopy:
Hyperpigmented trabecular meshwork or Sampaolesi line or exfoliative material in the angle recess. In patients with phacomorphic glaucoma, where a lenticular opacity precluded a view of the optic disc, glaucoma was defined as the presence of a hyper mature cataract, a visual acuity of HM or worse, the presence of an afferent pupillary defect and an IOP of ≥30 mmHg. Data collected was collated and analyzed using SPSS version 16 (SPSS, Inc, Chicago, USA). Frequencies and means were generated to observe patterns of variable distribution among the patients.
Results
A total of 5655 new patients attended the eye clinic during the study period, 1660(29.4%) were diagnosed with glaucoma out of which primary glaucoma were 1561(94.0%) while secondary were 99 (6.0%). The patients with secondary glaucoma, male:female ratio was 1.3:1, age range was 30-73 years, and median age was 55+/-2 years. Secondary glaucoma was found to be unilateral in 76.5% and bilateral in 23.5 %( Figure 1). The spectrum of secondary glaucoma were post traumatic glaucoma 25(25.2%), lens related glaucoma 16(16.2%), steroid induced glaucoma 14(14.2%), neovascular glaucoma 12(12.1%), uveitic glaucoma 10(10.1%), pseudoexfoliation glaucoma 10(10.1%), pigmentary glaucoma 6(6.1%), aphakic glaucoma 6(6.1%). Majority (80%) of patients with neovascular glaucoma and uveitic glaucoma presented at diagnosis with severe visual impairment and blindness in the affected eye. (Table 1, 2).
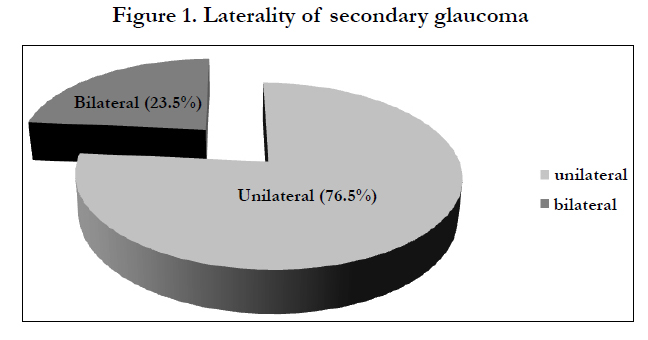
Figure 1. Laterality of secondary glaucoma
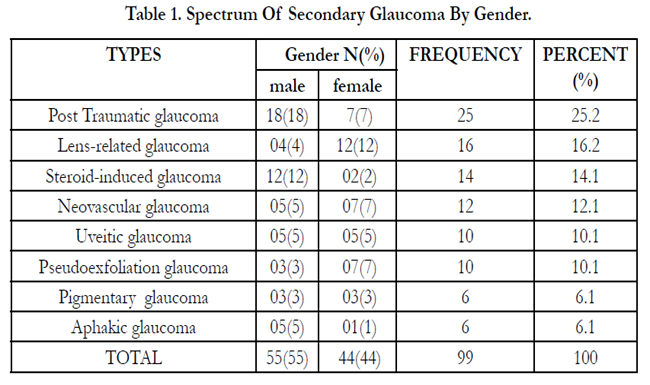

Table 1. Spectrum Of Secondary Glaucoma By Gender
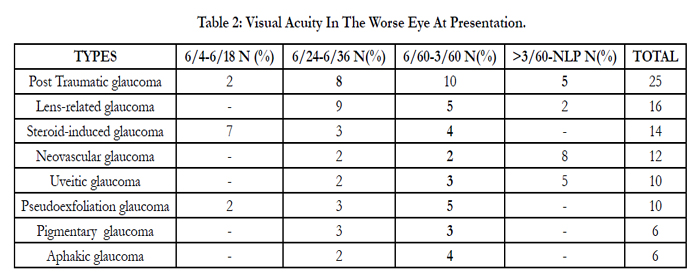
Table 2: Visual Acuity In The Worse Eye At Presentation.
Discussion
A total of 5655 new patients attended the eye clinic during the study period, 1660(29.4%) were diagnosed with glaucoma out of which primary glaucoma were 1561(94.0%) while secondary were 99(6.0%). This is similar to result obtained from the GlaucomaServices at the Aravind Eye Hospital, a large tertiary eye care centre in South India, where 367(6%) patients with various secondary glaucomas were seen in the year 2000 [11]. This prevalence is also slightly lower than the report from Tanzania [5] and China [6]; although far lower than study of Foster et al, in Singapore [7] (16%). This may be due to the higher population involved in Singapore study. Furthermore in our study, the male to female ratio was 1.3:1 slightly lower than 2:1 reported by Strohl et al [1] although theirs was a population based study. The prevalence of secondary glaucoma has been reported with varied age range [10, 11, 13] and in our study age range was 30-73 years, with median age of 55+/-2 years.
Post traumatic glaucoma was found to be the commonest cause of secondary glaucoma in this study; this is different from reports from India [4] and Paraguay [1] where it occurred as second most common cause of secondary glaucoma. In Singapore [7] and Tanzania [5], Pseudoexfoliation glaucoma was second and third most common type respectively. Pseudoexfoliation syndrome (a type of secondary glaucoma) was not common in our study although it is fairly common in East African and South African black people, but it is rare in West Africa, this may largely be due genetic predispostion [14].
In our study, blunt trauma was the mode of injury in 80% of cases, 60% were work-related, assaults or accidental injury. Angle recession was found in 35% of these patients with aid of gonioscopy. Hyphema, sphincter tear, iridodialysis, lens dislocation, cataract, vitreous haemorrhage, retinal detachment, were seen in coexisting with this post traumatic glaucoma in our study similar to reports from study in India [4].
Phacomorphic and phacolytic glaucoma are the lens related glaucoma seen in our study. The patients can associate visual reduction with eyeache, but present late to hospital. This may be due to low socio economic status of the patients and hence possible reason for the occurrence this type of glaucoma in our community. In India, similar reports were given by Ritu et al [4], although a decline in the prevalence of lens related glaucoma was observed.
Steroid-induced glaucoma was present in 14.1% of all cases in our study. This is far higher than report from Paraguay [1] with occurrence of 3% of all cases of steroid-induced glaucoma seen. The differences may be due to the indiscriminate use of steroids by patients for treatment of ocular allergies or postoperatively eye drops obtained over the counter without prescription. It is important to mention that steroid-induced response depends on the duration of therapy, type of steroids used, as well as genetic influence of a person. Most of the cases included in this study had glaucomatous optic neuropathy due to long-term use of systemic and/or local steroids, indicating their late presentation to this hospital. Therefore, medical practitioners need to be thoroughly educated on the side-effects of steroids and the importance of regular follow-up starting from initiation of steroid therapy with an ophthalmologist.
Secondary glaucomas had very poor vision (<6/60-NLP) at presentation in almost all types of secondary glaucoma seen in our study, however 80% of neovascular and uveitic glaucoma presented with severe low vision and blindness.
Unilateral eye involvement was observed in 76.5% of secondary glaucoma cases seen in our study. This is higher than reports from other authors [1, 4, 8] the reason for this may be traceable to the fact that majority of the secondary glaucoma seen in this study are due to ocular trauma which usually results in monocular visual impairment and blindness.
An obvious limitation of this study is that it was retrospective data in nature and such bias as missing records and incomplete data were encountered, this probably may result in low figures of secondary glaucoma seen during the study period and may eventually affect the overall prevalence of secondary glaucoma. The potential bias due to incomplete data also may limit the spectrum of secondary glaucoma reported in this study.
Conclusion
In conclusion, secondary glaucoma, although with low frequency of occurrence unlike the primary glaucoma, prompt diagnosis and treatment may help significantly in preventing resultant visual impairment and blindness.
Highlighting the weakness of the study in terms of Glaucoma diagnosis (Visual field test etc.)
Visual field test (Perimetry) was done for the entire patients seen for the study, the following were however the weakness/limitation of the study in terms of diagnosis of secondary glaucoma.
- Octopus visual field test and not Humphrey visual field test(which is the Gold standard in diagnosis) was used.
- Anterior segment OCT(optical coherence tomography) was not available in the hospital which would have helped in confirming the diagnosis of angle recession instead of using only gonioscopy.
- Furthermore other ophthalmic equipments such as Scanning Laser Polarimeter (GDX VCC) and Heidelberg retinal tomograph (HRT) were lacking in the centre. They could have helped in the diagnosis in early onset glaucomatous optic nerve damage in secondary glaucoma.
References
- Strohl A, Pozzi S, Wattiez R, Roesen B, Miño de Kaspar H, et al. (1999) Secondary glaucoma in Paraguay. Etiology and incidence. Ophthalmologe 96(6):359-63.
- Awoyesuku EA, Pedro-Egbe CN (2012) Clinical forms of glaucoma in a tertiary hospital in Nigeria. Port Harcourt Medical Journal 6: 3.
- Adekoya BJ, Onakoya AO, Shah SP, Adepoju F (2014) Surgical output and clinic burden of glaucoma in Lagos, Nigeria. J Glaucoma 23(1):41-5.
- Ritu Gadia, Ramanjit Sihota, Tanuj Dada, Viney Gupta (2008) Current profile of secondary glaucomas. Indian J Ophthalmol 56(4): 285–289.
- Fatima Kyari, Mohammed M Abdull, Andrew Bastawrous, Clare E Gilbert, Hannah Faal (2013) Epidemiology of glaucoma in Sub-Saharan Africa: Prevalence, incidence and risk factors. Middle East Afr J Ophthalmol 20:111-125.
- P. Foster, G. Johnson (2001) Glaucoma in China: how big is the problem? Br J Ophthalmol 85(11): 1277–1282.
- Foster PJ, Oen FT, Machin D, Ng TP, Devereux JG, et al. (2000) The prevalence of glaucoma in Chinese residents of Singapore: a cross-sectional population survey of the Tanjong Pagar district. Arch Ophthalmol 118(8):1105-11.
- Olawoye OO, Sarimiye TS (2014) Is angle closure glaucoma a problem in Nigeria? Niger J. Clin. Pract 17:159-162.
- Buhrmann RR, Quigley HA, Barron Y, West SK, Oliva MS, et al. (2000) Prevalence of glaucoma in a rural East African population. Invest Ophthalmol Vis Sci 41:40-8.
- Congdon N, Wang F, Tielsch JM (1992) Issues in the epidemiology and population-based screening of primary angle-closure glaucoma. Surv Ophthalmol 36:411-23.
- R Krishnadas, R Ramakrishnan (2001) Secondary Glaucomas: The Tasks ahead Community Eye Health Journal 14(39): 40–42.
- Quigley H A (1996) The number of people with glaucoma worldwide.Br J Ophthalmol 80: 389–393.
- Sunny Y. Shen, Tien Y. Wong, Paul J. Foster, Jing-Liang Loo, Mohamad Rosman, et al. (2008) The Prevalence and Types of Glaucoma in Malay People: The Singapore Malay Eye Study. Invest. Ophthalmol. Vis. Sci 49(9):3846-3851.
- Peter R Egbert (2002) Glaucoma in West Africa: a neglected problem. Br J Ophthalmol 86(2): 131–132.





