A Mechanism for Spontaneous Closure of a Traumatic Macular Hole with Commotio Retinae in a Pediatric Patient
Mehta I1, Foster WJ2*
1 School of Osteopathic Medicine, Philadelphia College of Osteopathic Medicine, Philadelphia, PA 19131, USA.
2 Departments of Ophthalmology & Bioengineering, Temple University, Philadelphia, PA 19140, USA.
*Corresponding Author
William J Foster, MD, PhD,
Departments of Ophthalmology & Bioengineering,
Temple University,
Philadelphia, PA 19140, USA.
E-mail: william.foster@temple.edu
Article Type: Case Report
Received: December 27, 2014, Accepted: January 15, 2015,Published: February 04, 2015.
Citation: Mehta I, Foster WJ (2015) A Mechanism for Spontaneous Closure of a Traumatic Macular Hole with Commotio Retinae in a Pediatric Patient. Int J Ophthalmol Eye Res 03(2) 95-96. doi: dx.doi.org/10.19070/2332-290X-1500018
Copyright: Foster WJ© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Macular holes can arise from different etiologies and can lead to vision loss. Though various treatments have been proposed, the management of traumatic macular holes is not widely standardized. We report on a case of a traumatic macular hole in a pediatric patient that spontaneously closed through a distinct mechanism, that we characterized by ocular coherence tomography. Over 6 months, the patient’s visual acuity improved from 20/400 to 20/40 as the macular hole closed.
2.Introduction
3.Materials and Methods
4.Results and Discussions
5.References
Keywords
Traumatic Macular Hole, Eye Trauma, Ocular Coherence Tomography, OCT, Pediatric.
Introduction
Several theories have been proposed for the development of idiopathic macular holes, including the cystoid degeneration theory, the vitreous theory, and involutional macular thinning [1]. While is it now understood that the majority of idiopathic macular holes fall into one of these categories, we will discuss a case of a traumatic macular hole arising from blunt ocular trauma and propose a mechanism for the formation and closure of the traumatic macular hole. In describing the pathogenesis of traumatic macular holes, it has been found that force of impact transmitted to the posterior pole can cause rupture of the delicate foveal tissue [2]. In addition, commotio retinae (retinal edema and opacification due to the degeneration of receptor cells in the outer nuclear layer) often occurs concurrently due to the force of trauma transmitting shock waves across the retina. It is believed that the damage from this <span class="style1">commotio</span> can be reversible [3,4].
The treatment for idiopathic macular holes usually involves vitrectomy with membrane peeling and injection of intraocular gas [1]. The literature is much less clear on the appropriate management for traumatic macular holes. We describe a case of a traumatic macular hole in a pediatric patient in which we characterized the mechanism of spontaneous hole closure.
Materials and Methods
This is a case presentation with review of the literature. Consent of the patient and her mother was obtained to publish the enclosed clinical data.
Results and Discussions
A 12-year-old female suffered blunt injury when a soccer ball struck her in the left orbit, resulting in acute loss of vision. She had no medical history of ocular or systemic disease. Her visual acuity at presentation was 20/400, and the initial OCT showed a full thickness macular hole without a posterior vitreous detachment (Figure 1A). Since our patient suffered from a traumatic macular hole, after discussion with the patient and her parents, we opted for conservative management and observation. In the following image series, a gradual closure of the hole can be seen (Figures 1B, 1C, 1D). These OCT images demonstrate that as the peri-foveal <span class="style1">commotio</span> resolved, the macular hole spontaneously rolled closed. Meanwhile, over a period of 6 months, the patient’s visual acuity reached 20/40 without any intervention.
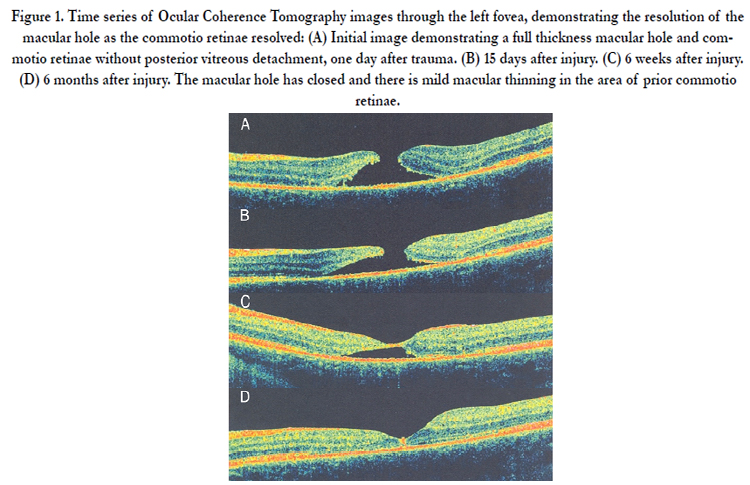

Figure 1. Time series of Ocular Coherence Tomography images through the left fovea, demonstrating the resolution of the macular hole as the commotio retinae resolved: (A) Initial image demonstrating a full thickness macular hole and commotio retinae without posterior vitreous detachment, one day after trauma. (B) 15 days after injury. (C) 6 weeks after injury. (D) 6 months after injury. The macular hole has closed and there is mild macular thinning in the area of prior commotio retinae.
Other mechanisms have been proposed for the spontaneous closure of traumatic macular holes. For example, a previously published case report in a much older patient, without macular <span class="style1">commotio</span>, suggested that the initial step in healing was the bridging of neuroretinal tissue across an empty subretinal space [5]. Other authors [6], after a thorough review of proposed mechanisms for a traumatic macular hole, emphasized the effectiveness and benefits of an early interventional approach, pursuing surgery. Proposed mechanisms reviewed by these authors include the force of impact being transmitted to the macula with rupture of the fovea, sudden vitreous separation, outward expansion of the equator of the eye, flattening and subsequent posterior displacement of the posterior pole, trampoline-like movement, tangential tractional forces on the retinal surface, contusion necrosis, cystoid degeneration, subfoveal hemorrhage, choroidal rupture, and anterioposterior vitreous traction.
Markedly different from other published cases [5,6], our case highlights the key role that resolution of macular edema, secondary to commotio retinae, can play in closure of a macular hole. In figure 1A, a full-thickness macular hole, with surrounding edema, including edema from commotio retinae, is present. Over time, as the edema resolved, the retinal tissues ‘rolled’ inward, re-attaching itself to the underlying RPE cells. Eventually, as the edema dissipated and through such a rolling process, the macular hole completely resolved.
Currently there is no widely accepted method of treatment for traumatic macular holes. Prior case series have documented, in select cases, spontaneous closure of traumatic macular holes, while other publications advocate early intervention with pars plana vitrectomy, especially in pediatric patients [6,7]. We suggest that, in some instances, observation can also lead to a good outcome.
We have presented a case of spontaneous resolution of a macular hole with several distinct features, including the young age of the patient and association with commotio retinae, and we have described the mechanism of closure. We suggest an initial period of observation of traumatic macular holes, rather than immediate surgical intervention, particularly in pediatric patients with juxtafoveal commotio retinae.
References
- Ho AC, Guyer DR, Fine SL (1998) Macular hole. Survey of Ophthalmology 42:393–416. DOI:10.1016/S0039-6257(97)00132-X
- Yanagiya N, Akiba J, Takahashi M, Shimizu A, Kakehashi A, et al (1996) Clinical characteristics of traumatic macular holes. Japanese Journal of Ophthalmology 40(4):544-547. PMID: 9130060
- Sipperley JO, Quigley HA, Gass DM (1978) Traumatic retinopathy in primates. The explanation of commotio retinae. Archives of Ophthalmology 96(12):2267–2273. PMID:718521
- Liem AT, Keunen JE, van Norren D (1995) Reversible cone photoreceptor injury in commotio retinae of the macula. Retina 15(1):58-61. PMID:7754249
- Menchini U, Virgili G, Giacomelli G, Cappelli S, Giansanti F (2003) Mechanism of spontaneous closure of traumatic macular hole: OCT study of one case. Retina 23(1):104-106. PMID: 12652242
- Azevedo S, Ferreira N, Meireles A (2013) Management of pediatric traumatic macular holes – case report. Case Reports in Ophthalmology 4(2):20-27. PMCID: PMC3725024
- Johnson RN, McDonal HR, Lewis H, Grand MG, Murray TG, et al (2001) Traumatic macular hole: observations, pathogenesis, and results of vitrectomy surgery. Ophthalmology 108(5):853-857. PMID: 11320012
- Yamada H, Sakai A, Yamada E, Nishimura T, Matsumura M (2002) Spontaneous closure of traumatic macular hole. American Journal of Ophthalmology 134(3):340-347. PMID: 12208244





