Visual Outcomes of Manual, Small-Incision Cataract Surgery in Patients with Coexisting Corneal Opacity
Ma H, Weina Ren, Li J, Chen W*
School of Ophthalmology and Optometry, Wenzhou Medical University, 270 Xueyuan West Road, Wenzhou, Zhejiang, China.
*Corresponding Author
Wei Chen MD,
School of Ophthalmology and Optometry,
Wenzhou Medical University,
270 Xueyuan West Road, Wenzhou,
Zhejiang, 325027, China.
E-mail: chenweimd@hotmail.com
Received: August 02, 2015; Accepted: December 13, 2015; Published: December 16, 2015
Citation: Ma H, WeinaRen, Li J, Chen W (2015) Visual Outcomes of Manual, Small-Incision Cataract Surgery in Patients with Coexisting Corneal Opacity. Int J Ophthalmol Eye Res 03(10), 154-159. doi: dx.doi.org/10.19070/2332-290X-1500033
Copyright: Chen W© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The purpose of this study was to analyze the relationship between corneal opacity and vision acuity in patients with cataracts and coexisting corneal opacity by calculating the area of corneal opacities in the optical zone.
Methods: This retrospective study involved 177 cataract patients (184 eyes) with corneal opacity who were successfully undergoing manual, small-incision cataract extraction and intraocular lens implantation. These patients were all treated by the same surgeon from December, 2011 to March, 2014 in our hospital. The 184 eyes analyzed were divided into three groups according to the area of corneal opacity in optical zone (O/OZ): Group 1: O/OZ < 30%, Group 2: 30% ≤ O/OZ < 60%, Group 3: O/OZ ≥ 60%.
Results: Preoperative visual acuity of all 184 eyes examined was less than 20/70. Postoperative visual acuity differed significantly between the three groups. O/OZ was significantly correlated with preoperative visual acuity and visual acuity improvement (P = 0.001, P = 0.039). When O/OZ < 60%, postoperative visual acuity was associated with hardness of the lens nucleus. When O/OZ ≥ 60%, visual acuity depended on the area of corneal opacity rather than the hardness of the nucleus.
Conclusion: Findings from this study demonstrate that manual small-incision cataract extraction and intraocular lens implantation for patients with cataract coexisting corneal opacity is feasible and safe. Visual acuity was significantly correlated with both O/OZ and lens opacity.
2.Introduction
3.Methods
3.1.Research methods
3.2.Patients
3.3.Opacity/Optical Zone, O/OZ
3.4.Surgical approach
4.Results
4.1.Visual acuity preoperative
4.2.Visual acuity postoperative
5.Discussion
6.References
Keywords
Cataract; Manual Small-i Incision Cataract Extraction; Corneal Opacity in Optical Zone; Association Coefficient; Hardness of the Nucleus.
Introduction
Cataracts are the leading cause of blindness worldwide, followed by corneal disease [1]. In China, infective corneal disease is the major cause of corneal opacity [2]. Patients with corneal disease typically also have cataracts. The majority of these patients are elderly, with poor awareness of treatment and few economic resources. Often their requirements for visual outcomes are relatively low [3, 4].
Corneal transplantation is currently the only way to treat corneal opacity, and surgery is the traditional therapy for cataracts combined with corneal opacity. Combining corneal transplantationwith cataract surgery is often called a “triple procedure.” This is currently the first choice for many ophthalmologists to prevent damage to the endothelium during the second operation and shorten the recovery time [5, 6]. However, combined surgery also has drawbacks; for example, capsulorhexis is more complex, and there is risk of a posterior capsular tear [7].
Recent improvements in surgery techniques, the establishment of eye banks, and the use of artificial corneas immunosuppressive agents and other new medicines facilitated the development of the “triple procedure”. However, China faces several challenges in this regard, such as a lack of corneal donors, graft rejections incorneal transplantation surgery and other related complications [8-12]. While cataract surgery is not the first choice in these cases, cataract surgery provides hope for improving the vision of elderly patients, especially for high-risk transplantations and patients who are less likely to comply with a meticulous post-operative followup.
A study on the effects of phacoemulsification and intraocular lens implantation on patients with coexisting corneal opacity (205 eyes) undergoing phacoemulsification concluded that cataract surgery is safe and feasible [3]. Sinha et al. found that cataract surgery with pupillary sphincterotomy in the clear cornea region (14 eyes), improved vision significantly [13]. However, the visual outcomes of cataract surgery are affected by the location of opacity, the level of opacity density and the area of corneal opacity. Research is needed to determine the relationship between opacity area and vision acuity in cataract surgery. Therefore, in this study, we calculated the area of corneal opacity in the optical zone and analyzed the relationship between corneal opacity and vision acuityin patients with cataracts and coexisting corneal opacity.
Methods
This study included 177 patients (188 eyes) with significant cataracts and co-existing corneal opacity. All patients were successfully undergoing manual small-incision cataract extraction and intraocular lens implantation with the same surgeon from December 2011 to March 2014 in our hospital. According to the area of corneal opacity in optical zone (O/OZ), the 184 eyes were divided into three groups: Group 1: O/OZ < 30%, Group 2: 30% ≤ O/OZ < 60%, Group 3: O/OZ ≥ 60%.
The axial length was measured with a Zeiss IOL-Master instrument (Germany as necessary, according to the normal or contralateral eye. The presenting monocular visual acuity (PVA) was measured with the Standard Visual Acuity Chart.
1. Patients with nuclear hardness at N1 or above (nucleus hardness intraoperative III as N1, IV as N2, V as N3).
2. Patients with corneal macula or nebula partially covered optical zone (the central 4mm circle was defined as the optical zone).
3. Patients with the partial anterior capsule and pupillary margin still visible.
4. Patients with a presenting distance of visual vision of less than 20/70.
Active infections, lens dislocation or suspensory ligament rupture, endothelial dysfunction, glaucoma or severe retinopathy.
To calculate the area of corneal opacity, we collected preoperative anterior segment photographs for the 184 eyes studied. Photos were the same size, 1600 pixels in width and 1200 pixels in height, taken with SLM slit lamp image system software (V1.0 Kang Hua Company, China). No photographs were modified.
Adobe Photoshop (CS6 13.0.0) was used to analyze preoperative photographs (Figure 1).
1. The oval tool was used to mark the limbus, with four points: up, down, left, right, and the midpoint of cornea.
2. The 4 mm central circle was marked as the optical zone (assuming an average cornea size of approximately 12 mm).
3. The lasso tool was used to plot opacity, with a slash representing opacity in optical zone (O/OZ).
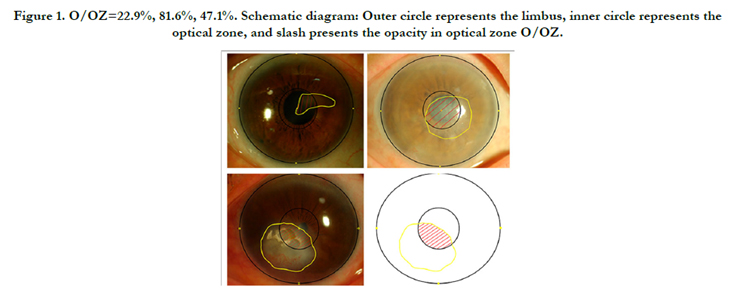
Figure 1. O/OZ=22.9%, 81.6%, 47.1%. Schematic diagram: Outer circle represents the limbus, inner circle represents the optical zone, and slash presents the opacity in optical zone O/OZ.
The location of the incision was chosen according to corneal opacities. The brightness and direction of the illuminant was adjusted accurately. Trypan blue (Vision Blue, Dorc Int., Netherlands) was used to stain the anterior capsule. Vannas capsulotomy scissors were used for patients with synechia or microcoria. Partial iridectomy or pupil reconstruction was used for patients with iris adhesions or co-existing dense corneal opacity in the optical zone. Follow-ups were conducted on postoperative day1, day7, month 1 and month 3.
Results
The mean age of the 177 patients (184 eyes) was 73.4 ± 8.3years. Regarding opacities in optical zone O/OZ, 71 eyes with less than 30% opacity were included in Group 1, 62 eyes (with 30% to 60% opacity were included in Group 2, and 51 eyes more than 60% opacity included in Group 3. The average age of patients in Groups 1, 2 and 3 was 74.2 ± 7.1, 73.2 ± 10.8 and 71.0 ± 11.1 years, respectively. No significant differences were found in terms of age between three groups. More than half of the eyes (119, 64.7%) had corneal opacity due to healed keratitis. There were no statistically significant differences between three groups in terms of pathogenesis (Table 1).
In terms of intraoperative hardness of the nucleus, the proportions of N3 in each group were 25.4%, 37.1% and 37.3%. There were no statistically significant differences between three groups, P = 0.402. (See Figure 2).
On postoperative day 1, eleven eyes revealed a grade II-III AC reaction, which was controlled with intensive topical and systemic corticosteroid use. There was no clinically detectable cystoid macular edema, corneal endothelial decompensation were observed in any of the eyes during follow-ups. Mild corneal edema was observed in some cases, which disappeared within 1 week postoperatively.
Although we aimed to measure corneal endothelium and corneal astigmatism, this was not possible for most patients. Since opacity in the cornea, especially in the pupil, produced inaccurate results, we did not process this data. There was a slight fluctuation in subjective refraction during the follow-ups, which remained stable after 1 month postoperative (data not shown).
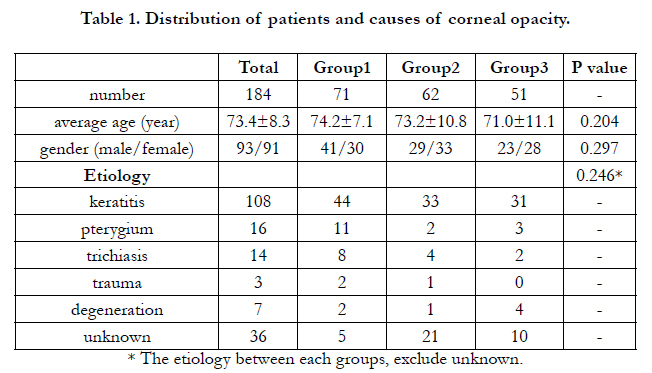

Table 1. Distribution of patients and causes of corneal opacity.
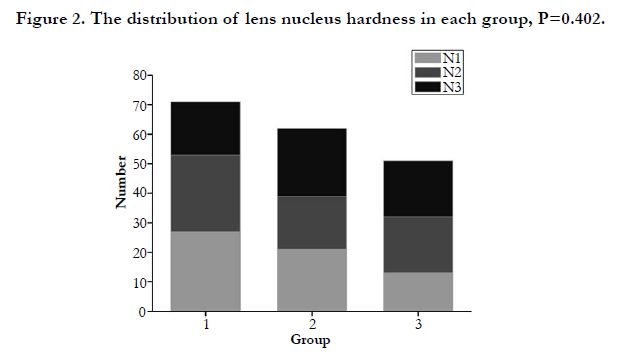
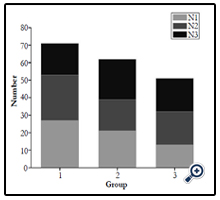
Figure 2. The distribution of lens nucleus hardness in each group, P=0.402.
Visual acuity before surgery in all 184 eyes was less than 20/70. In 93 eyes (50.5%), visual acuity was less than 20/400. This included 28 eyes in Group 1 (39.4%), 29 eyes in Group 2 (46.8%), and 36 eyes in Group 3 (70.6%). The average visual acuity in each group was 1.33 ± 0.57 logMAR, 1.42±0.53 logMAR and 1.69±0.55 log- MAR. All groups showed significant differences, P=0.001.
The coefficient of association between O/OZ and visual acuity preoperative r = 0.206, P = 0.005 was statistically significant. However, for all groups, the coefficient of association was not significant. O/OZ was found to be significantly correlated with preoperative visual acuity preoperative; the larger the O/OZ, the worse the preoperative visual acuity. After grouping, O/OZ was found to have no significant effect on preoperative visual acuity.
The coefficient of association between preoperative visual acuity and nucleus hardness r = 0.766, P = 0.001 was statistically significant. There were no significant differences between each group, P = 0.939. The P value in each group was smaller than 0.05.
Results show that 47.8% of the 184 eyes reached or exceeded 20/70 visual acuity postoperatively. Group 1 had 55 cases (77.5%). Figure 3 shows changes in visual acuity for each group.
Results also show statistical differences between each group for postoperative visual acuity. The coefficient of association between postoperative visual acuity and O/OZ r = 0.594, was statistically significant, P=0.001. There was no statistical difference in the coefficient of association for each group (Figure 4).
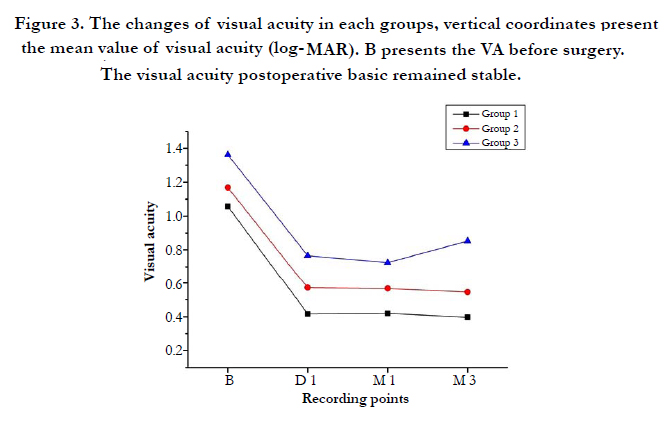
Figure 3. The changes of visual acuity in each groups, vertical coordinates present the mean value of visual acuity (log- MAR). B presents the VA before surgery. The visual acuity postoperative basic remained stable.
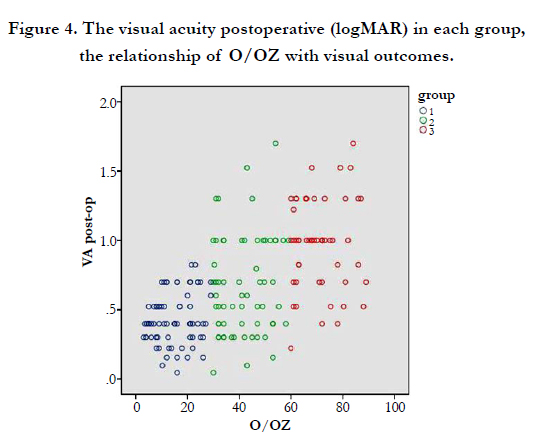
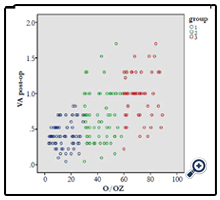
Figure 4. The visual acuity postoperative (logMAR) in each group, the relationship of O/OZ with visual outcomes.
The coefficient of association between postoperative visual acuity and nucleus hardness r = 0.303, P = 0.001, which was statistically significant. Postoperative visual acuity in Group 1 and Group 2 was significantly correlated (P=0.032, 0.026), while for Group 3, there was no correlation (P = 0.201). That is, when O/OZ < 60%, postoperative visual acuity was associated with the lens nucleus hardness. When O/OZ ≥ 60%, visual acuity depended on the area of corneal opacity rather than the hardness of the nucleus.
The coefficient of association between visual acuity improvement and O/OZ was statistically significant (r=0.152, P=0.039). However, there was no significant visual acuity improvement for each group. In other words, visual acuity improvement was significantly correlated with O/OZ, and the larger the O/OZ, the greater the visual acuity improvement.
The coefficient of association between visual acuity improvement and nucleus hardness was statistically significant (r =-0.606, P = 0.001). The visual acuity improvement in each group was significantly correlated. The visual acuity improvement in each groups was: 0.89 ± 0.53 logMAR, -0.75 ± 0.58 logMAR and -0.72 ± 0.54 logMAR (Table 2).
Typical cases shows are depicted in Figure 5.
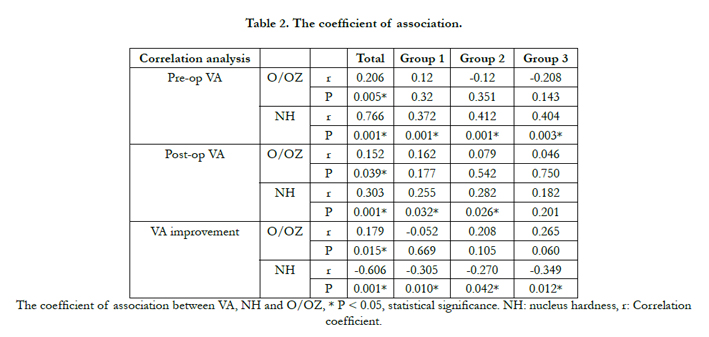
Table 2. The coefficient of association.
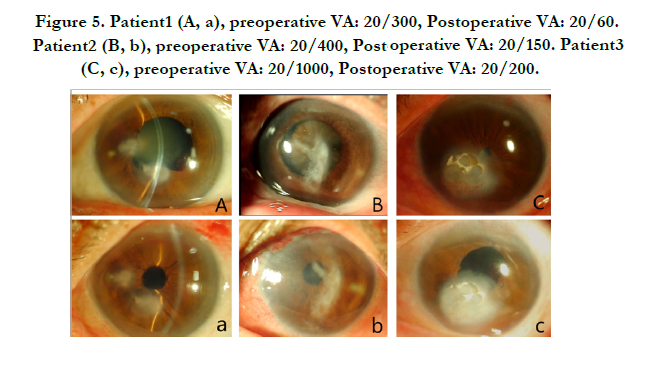
Figure 5. Patient1 (A, a), preoperative VA: 20/300, Postoperative VA: 20/60. Patient2 (B, b), preoperative VA: 20/400, Postoperative VA: 20/150. Patient3 (C, c), preoperative VA: 20/1000, Postoperative VA: 20/200.
Discussion
Cataract is the leading cause of blindness worldwide, followed by refractive errors and corneal opacity [1, 14]. Corneal transplantation is an ideal procedure to remove corneal opacity. However, this procedure is less common in China due to the scarcity of donor material, rejection, and surgical complications [15].
Varying degrees of corneal opacity, especially dense opacity in the optical zone, significantly affect visual acuity. Some studies show that contact lenses can improve visual acuity in patients with cornealopacities by correcting corneal astigmatism. However, this effect is limited by many factors [16]. Keratoplasty requires better compliance and long-term follow-up. Patients with both cataracts and corneal opacity are often elderly [17]. The goal for these patients is to achieve basic vision for a normal life, and safety is the essential requirement [18]. Cataract surgery is a viable approach for these patients.
Currently, there are two main surgeries for cataracts: phacoemulsification and manual small-incision cataract extraction (MSICS) [19]. Studies demonstrate that they are equally safe and effective, and the cost-benefit of manual small-incision cataract extraction is better than phacoemulsification [20]. What’s more, the extended time required for ultrasound in phacoemulsification cancause cornea endothelial damage, may cause tissue damage, and can even lead to edema and infection. Intraocular operation in patients with cataracts co-existing with corneal opacity requires more time and caution due to poor visualization of intraocular morphology and altered dynamics. In addition, scleral tunnel incision must be used to prevent limbus lesions [20].
Therefore, this study suggests that manual small-incision cataract extraction is safer than phacoemulsification and is suitable for patients with cataract co-existing corneal opacity. Our results showno significant complications in follow-ups. In this investigation, the iris was removed in the case of iris adhesions, and multiple sphincterotomy was used to enlarge the visible pupillary area, increasing visual acuity [13].
Some studies suggest that cataract surgery may aggravate existing corneal diseases, including inflammation, infection and dry eye [21, 22]. Therefore, it is important to identify existing corneal diseases and exclude activity eye infection before performing this procedure. Corneal opacities, especially in the optical zone, affect cataract surgery outcomes. The use of trypan blue and lighting system increases the safety of cataract surgery [23]. Our results show no serious complications in follow-ups.
Uncorrected refractive error in the postoperative period can also affect presenting visual acuity (PVA). Therefore, it can be difficult for elderly patients to adapt to glasses, especially in rural areas. Accurate measurement and calculation of IOL dioptric preoperative are particularly important. In addition, corneal opacity, especially dense in the pupil, black cataracts and instable or eccentric fixation,can affect the accuracy of the IOL-Master. In this study, the Zeiss IOL-Master (Germany) was used to calculate the IOL dioptric.When the axial < 22mm, SRK-II, formula was used. When the axial ≥ 22mm, the SRK/T formula was used. When it was difficult to measure the operative eye, this referred to the other eye or the normal value.
Our findings show significant differences in visual acuity preoperatively and postoperatively between each group. This was related to O/OZ and nuclear hardness. The aim of this study is to discuss the relationship between corneal opacity and vision acuity in patients with cataracts and coexisting corneal opacity. We did not make any treatment for corneal opacity before and after cataract surgery. Thereby, corneal opacity remained unchanged, including the location and distribution. The astigmatism caused by corneal opacity would not change either. When we consider the improvement in visual acuity after cataract surgery, the astigmatism remains constant, it would not influence the results and conclusions. Visual acuity is obviously correlated with corneal opacity, but there is no conflict with the present study.
In each group, the postoperative visual acuity showed no statistical correlation with O/OZ. However, it was significantly correlated with nuclear hardness in Group 1 and Group 2. In Group 3, there was no significant correlation. Results show a significant correlation between O/OZ and postoperative visual acuity. However, when O/OZ ≥ 60%, there was no correlation between postoperative visual acuity postoperative and nuclear hardness. The improvement in visual acuity was significantly correlated with O/ OZ and nuclear hardness. Findings also suggest that single cataract surgery can improve visual acuity when O/OZ is less than 60%, and that removal of crystal opacity can improve visual acuity. On the other hand, for O/OZ of more than 60%, single cataract surgery may not be as effective.
This study demonstrates that poor preoperative visual acuity and heavier lens opacity play an important role in vision loss. Therefore, if opacity is removed from the lens, vision improves dramatically. Findings of this study reveal that the vision of most cataract patients with co-existing corneal opacity can be significantly improved by simple cataract surgery rather than the triple procedure. This indicates that if doctors cannot determine whether corneal opacity and lens opacity is impairing a patient’s vision impairment, then it economical and safe to perform simple cataract surgery first.
References
- Pascolini D, Mariotti SP (2012) Global estimates of visual impairment: 2010. Br J Ophthalmol 96(5): 614-618.
- Xu L, Wang Y, Li Y, Wang Y, Cui T, et al. (2006) Causes of blindness and visual impairment in urban and rural areas in Beijing: the Beijing Eye Study. Ophthalmology 113(7): 1131e1-11.
- Panda A, Krishna SN, Dada T (2012) Outcome of phacoemulsification in eyes with cataract and cornea opacity partially obscuring the pupillary area. Nepal J Ophthalmol 4(2): 217-223.
- Liang YB, Friedman DS, Wong TY, Zhan SY, Sun LP, et al. (2008) Prevalence and causes of low vision and blindness in a rural chinese adult population: the Handan Eye Study. Ophthalmology 115(11): 1965-1972.
- Baykara M, Ucan G (2008) Modifying the position of cataract incisions in triple procedure. Eur J Ophthalmol 18(6): 891-894.
- Zaki AA, Elalfy MS, Said DG, Dua HS (2015) Deep anterior lamellar keratoplasty- triple procedure: a useful clinical application of the pre-Descemet's layer (Dua's layer). Eye (Lond) 29(3): 323-326.
- Shimmura S, Ohashi Y, Shiroma H, Shimazaki J, Tsubota K (2003) Corneal opacity and cataract: triple procedure versus secondary approach. Cornea 22(3): 234-238.
- Kobayashi A, Segawa Y, Nishimura A, Shirao Y, Sugiyama K (2004) Indocyanine green staining for the triple corneal procedure. Ophthalmic Surg Lasers Imaging 35(1): 23-25.
- Chen W, Ren Y, Zheng Q, Jhanji V (2014) Stabilized triple procedure for management of coexisting corneal opacity and cataract. J Cataract Refract Surg 40(12): 1966-1970.
- Magalhaes OA, Marinho DR, Kwitko S (2013) Topical 0.03% tacrolimus preventing rejection in high-risk corneal transplantation: a cohort study. Br J Ophthalmol 97(11): 1395-1398.
- Dohlman TH, Omoto M, Hua J, Stevenson W, Lee SM, et al. (2015) VEGF-trap Aflibercept Significantly Improves Long-term Graft Survival in High-risk Corneal Transplantation. Transplantation 99(4): 678-686.
- Avadhanam VS, Liu CS (2014) A brief review of Boston type-1 and osteoodonto keratoprostheses. Br J Ophthalmol 2014: 305359.
- Sinha R, Sharma N, Vajpayee RB (2004) Visual outcome of cataract surgery with pupillary sphincterotomy in eyes with coexisting corneal opacity. BMC Med 2: 10.
- Singh N, Eeda SS, Gudapati BK, Reddy S, Kanade P, et al. (2014) Prevalence and causes of blindness and visual impairment and their associated risk factors, in three tribal areas of Andhra Pradesh, India. PLoS One 9(7):e100644.
- Yu JF, Huang YF (2011) Keratoprosthesis in china. Ophthalmology 118(7): 1486-1487.
- Singh K, Jain D, Teli K (2013) Rehabilitation of vision disabling corneal opacities: is there hope without corneal transplant? Cont Lens Anterior Eye 36(2): 74-79.
- Zhao J (2014) To promote universal eye health to push forward sustaining development of the prevention of blindness in China. Zhonghua Yan Ke Za Zhi 50(3): 161-163.
- Dev MK, Shrestha GS, Paudel N, Joshi ND, Thapa M, et al. (2012) Visual status and ocular morbidity in older adults living in residential care. Graefes Arch Clin Exp Ophthalmol 250(9): 1387-1393.
- Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD, Joshi SA, et al. (2005) Safety and efficacy of phacoemulsification compared with manual small-incision cataract surgery by a randomized controlled clinical trial: sixweek results. Ophthalmology 112(5): 869-874.
- Gogate PM (2009) Small incision cataract surgery: Complications and minireview. Indian J Ophthalmol 57(1): 45-49.
- Greene JB, Mian SI (2013) Cataract surgery in patients with corneal disease. Curr Opin Ophthalmol 24(1): 9-14.
- Cho YK, Kim MS (2009) Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol 23(2): 65-73.
- Habeeb SY, Varma DK, Ahmed II (2011) Oblique illumination and trypan blue to enhance visualization through corneal scars in cataract surgery. Can J Ophthalmol 46(6): 555-556.





