Comparative Study of Visual Outcomes Following Corrective Vitrectomy: Non-Traumatic Versus Traumatic Etiologies
Shah MA*, Shah SM, Kalyani PJ, Shah AH, Shah PD, Patel KB
Drashti Netralaya, Dahod, Gujarat, India.
*Corresponding Author
Mehul A. Shah MD,
Drashti Netralaya, Nr. GIDC,
Chakalia Road, Dahod-389151,
Gujarat, India.
Tel: 00-91-2673-645364
Fax: 00-91-2673-221232
E-mail: omtrust@rediffmail.com
Article Type: Research Article
Received: October 05, 2014; Accepted: November 06, 2014; Published: November 07, 2014
Citation: Shah MA*, et al., (2014). Comparative study of visual outcomes following corrective vitrectomy: non-traumatic versus traumatic etiologies. Int J Ophthalmol Eye Res. 02(8), 86-89. doi: dx.doi.org/10.19070/2332-290X-1400016
Copyright: Shah MA© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Nucleus drop is a rare and serious complication. We investigated visual outcomes following corrective surgery, and compared outcomes between surgeries that followed traumatic injuries and those where the etiology was nontraumatic.
Methods: A retrospective cohort study was performed using information collected from medical records regarding cases of vitrectomy performed for nucleus drop. Patients were grouped into traumatic and non-traumatic cases. After pars plana vitrectomy and nucleus removal with use of a phacofragmatome, all data were collected according to a standard follow-up format.
Results: Our cohort consisted of 37 eyes of 37 patients. Mean patient age was 58.8+/-9.35, ranging from 31 to 75 years (Table1). Of these cases, 12 (32.4%) were traumatic and 25 (67.6%) followed cataract surgeries. We found that vision in 15 (40.4%) cases improved to more than 6/24 and in 5 (13.5%) it did not improve (>1/60).
Conclusion: Visual outcome following corrective vitrectomy for nucleus drop may be satisfactory if managed well; no significant difference in outcome was noted based on etiology.
2.Methods
2.1.Design
2.2.Inclusion
3.Results
4.Discussion
5.Conclusion
6.References
Introduction
Cataracts are responsible for 47% of all cases of blindness worldwide. The epidemiological impacts of cataracts vary among different countries, and the rate of occurance is associated with economic conditions. All stakeholders wish to improve the quality and quantity of cataract surgery. [2]
Various postgraduate training programs in cataract surgery are currently available in many parts of the world, at different government and nongovernmental institutions, with a range of facilities.
[2]
Differences in infrastructure, patient load, and skill of the faculty at various training facilities lead to the acquisition of differing skill levels and differing surgical results. Modern cataract surgery has a steep learning curve.
It is important to monitor the outcomes of surgical treatment for cataracts [3]. Cataract surgery is usually performed by phacoemulsification, but manual small incision cataract surgery (MSICS) is an important technique that is often used in developing countries, with comparable surgical outcome safety and efficacy. [4,5]
Nucleus drop is one of the serious complications of cataract surgery. Visual outcomes are poor following nucleus drop. [6,7]
Trauma is a cause of monocular blindness in the developed world, although few studies have addressed the problem of trauma in rural areas. [8-11]
Ocular trauma can cause cataracts. [8] The methods used to evaluate visual outcomes in eyes managed for traumatic cataracts and senile cataracts are similar[11], but damage to other ocular tissues may compromise visual gain in eyes operated on for traumatic cataracts. Hence, the success rates may differ between eyes with these two types of cataract. Traumatic cataract is one of the important causes of loss of vision following ocular trauma. [11-13]
With the introduction of the Birmingham Eye Trauma Terminology System (BETTS), the documentation of ocular trauma has been standardized. [5] Therefore, it should be valuable to study the visual outcomes following traumatic cataract surgery and determinants predicting that outcome, especially in relation to the BETTS. Visual outcomes for traumatic cataracts have been reported in some cases. [12-15]
Methods
We enrolled all patients with nucleus drop, with iatrogenic or traumatic etiologies, following cataract surgery by phacoemulcification or by manual small incision cataract surgery. We collected data from the medical records of all such cases. We excluded cases with follow-up of less than four weeks following surgical treatment. All methods were approved by our ethics committee.
All enrolled patients had their vision tested using a Snellen chart, received an anterior examination using a slit lamp, and had posterior segment findings documented using indirect ophthalmology. When the fundus was not visible, B-scan ultrasonography was used to access the posterior segment. Pars plana vitrectomies were performed using a non-contact viewing system. We removed nuclei of varying toughness using phacofragmentation. We followed up patients following a standard format and schedule.
All cases of nucleus drop due to ocular trauma had been treated with systemic corticosteroids.
All data were entered in an online pretested form, exported to an Excel spreadsheet, and analysed using SPSS [17]. Frequency distributions and cross-tabulation were analyzed, calculating 95% confidence intervals. Effects were considered significant if the value of P was <0.05.
Results
Our cohort consisted of 37 eyes of 37 patients. Mean age was 58.8+/-9.35 years, and ranged from 31 to 75 (Table 1). Of these, 12(32.4%) were classed as traumatic nucleus drop and 25 (67.6%) followed cataract surgeries (Table 2). In the iatrogenic group, 18 (48.6%) suffered nucleus drop during phacoemulcification and 7 (18.9%) following manual small incision cataract surgeries. In the entire cohort, we were able to insert a posterior chamber intraocular lens in 22 (59.5%) cases; the other 15 cases remained aphakic.
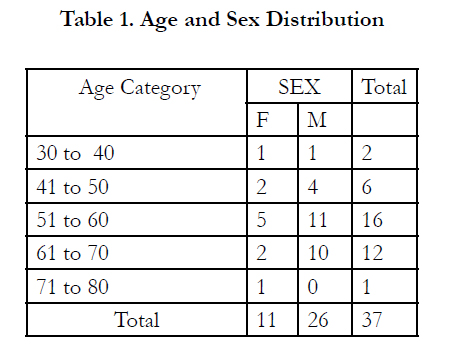

Table 1. Age and Sex Distribution
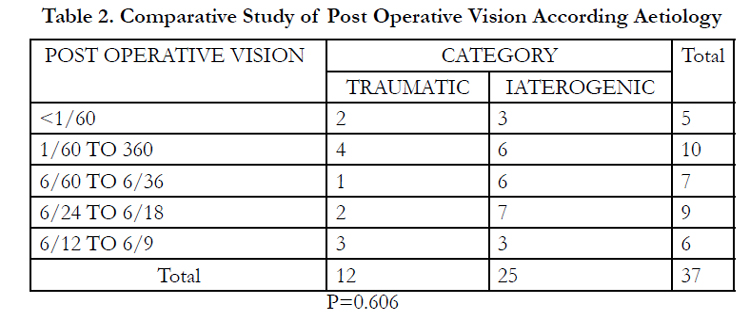
Table 2. Comparative Study of Post Operative Vision According Aetiology
When we examined visual outcomes of all patients following surgical management of nucleus drop, we found significant improvements (p=0.029, Table 3). We found that 15 (40.4%) cases improved more than 6/24, and 5 (13.5%) did not improve more than 1/60, because of comorbidities.
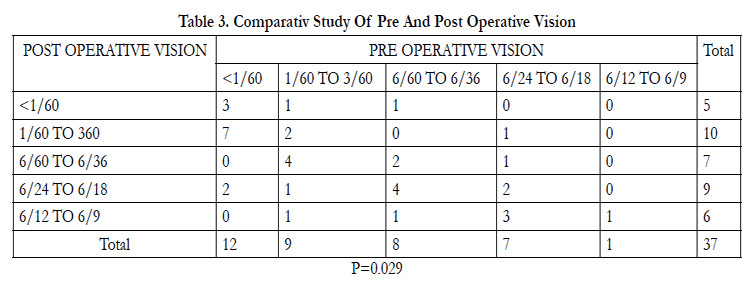
Table 3. Comparativ Study Of Pre And Post Operative Vision
We compared visual outcomes by etiology, between traumatic and non-traumatic causes, following surgical management, and did not find any significant difference between these groups (p=0.606, Table 2).
No significant difference in visual outcome was seen between surgical management using 20- and 23-gauge vitrectomy systems (p=0.747, Table 4).
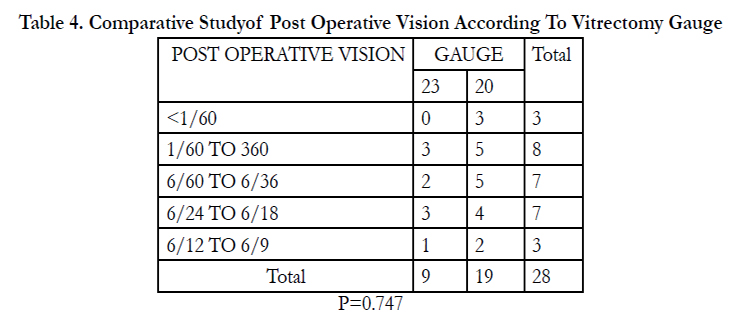
Table 4. Comparative Studyof Post Operative Vision According To Vitrectomy Gauge
In comparing visual outcomes of surgical management with different time lags after primary procedure or trauma, we found no significant difference found. [11] (p=0.135 Table 5).
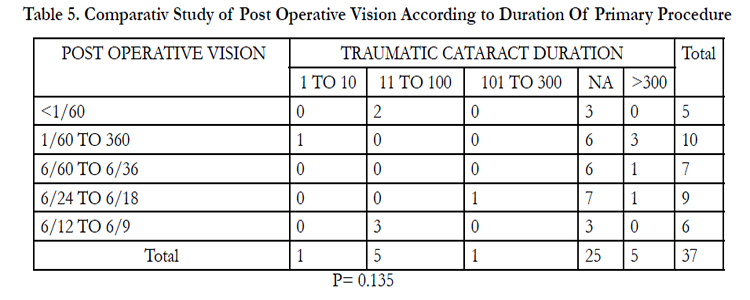
Table 5. Comparativ Study of Post Operative Vision According to Duration Of Primary Procedure
In the non-traumatic cases, no significant difference in visual outcome following surgical management was seen between primary surgery using phacoemulcification or manual small incision (p=0.09 Table 6).
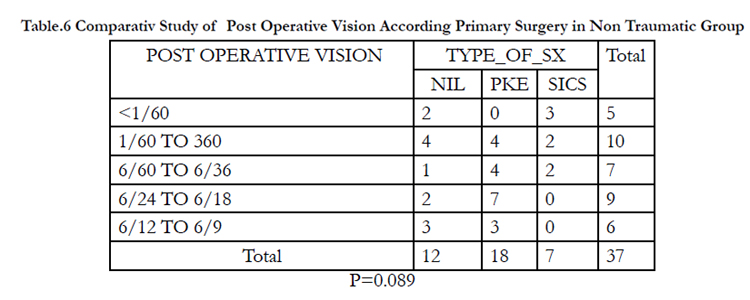
Table.6 Comparativ Study of Post Operative Vision According Primary Surgery in Non Traumatic Group
Patients who were aphakic or pseudophakic showed no difference in visual outcome (p=0.328, Table 7).
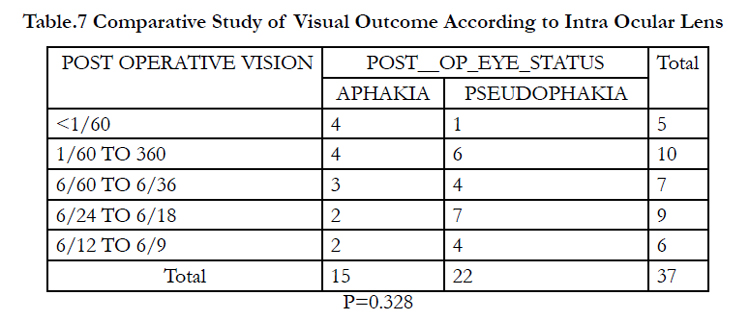
Table.7 Comparative Study of Visual Outcome According to Intra Ocular Lens
Discussion
In this patient cohort, visual outcomes significantly improved following surgical management, as has been found by other authors. [6,7]
Kelantan et al. reported on the incidence of nucleus drop in posterior polar type cataracts, but we found it associated with all types of morphology, as many surgeries are performed by junior surgeons. [6,7]
Visual outcome was not significantly different when compared according to etiology (p=0.606). We are not aware of any other study that has examined this variable. In cases of ocular trauma, the lens is not the only structure that influences visual outcome. [16,17]
When we examined the time duration between primary insults and corrective surgery, we found no significant effect of greater time lag (p=0.135) on later vision. This may be because inflammation following the primary insult had subsided during the early period. When vitrectomy is performed late, visibility is better and no retinal detachment is found, suggestive of a better prognosis. Shah et al. suggested late intervention in traumatic cases. [17]
We did not find significant differences due to vitrectomy gauge, primary procedure, or presence or absence of an intraocular lens. We did not find any other study with which to compare these findings.
Conclusion
We conclude that, although nucleus drop is a serious complication, if it is managed well, a good visual outcome may be achieved. There was no difference in visual outcomes between traumatic and non-traumatic etiologies.
References
- Lawani R, Pommier S, Roux L, Chazalon E, Meyer F. (2007) Magnitude and strategies of cataract management in the world. Med Trop (Mars) 67:644-50.
- Shah MA, Shah SM, Upadhyay PK, Appalwar AH, Gupta AS. (2011) Final visual outcome following re exploration of cataracts performed by trainee surgeons in India. Indian J Med Sci 65:365-70.
- Bulletin of the World Health Organization (1999) 77 (6).
- Hennig A, Kumar J, Yorston D, Foster A. (2003) Suture less cataract surgery with nucleus extraction: outcome of a prospective study in Nepal. Br J Ophthalmol 87:266–270.
- Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD, Joshi SA. (2005) Safety and efficacy of phacoemulsification compared with manual small incision cataract surgery by a randomized controlled clinical trial: six-week results. Ophthalmology 112: 869–74.
- Kalantan H. (2012) Posterior polar cataract: A review. Saudi J Ophthalmol 26(1): 41-9.
- Das S, R. Khanna. (2008) Surgical and visual outcomes for posterior polar cataract. Br J Ophthalmol 92:1476-8.
- Khatry SK, Lewis AE, Schein OD, Thapa MD, Pradhan EK, et al. (2004) The epidemiology of ocular trauma in rural Nepal. Br J Ophthalmol. 88:456-60.
- Abraham D. I, Vitale S. I, West S. I, Isseme I. (1999) Epidemiology of eye injuries in rural Tanzania. Ophthalmic Epidemiol. 6:85-94.
- D. Virgil Alfaro, Eric P. Jablon, Monica Rodriguez Fontal, Simon J. Villalba, Robert E.Morris, et al. (2005) Fishing-related ocular trauma. American Journal of Ophthalmology. 139:488-492.
- Shah M, Shah S, Khandekar R. (2008) Ocular injuries and visual status before and after their management in the tribal areas of Western India-A historical cohort study. Grafes Arch Clin Exp Ophthalmol 246:191–197.
- Kuhn F, Morris R, Witherspoon CD, Mester V. (2004) The Birmingham Eye Trauma Terminology system (BETT). J Fr Ophtalmol. 27:206-10.
- Shah M, S. Shah. (2011) Visual recovery and predictors of visual prognosis after managing traumatic cataracts in 555 patients. Indian J Ophthalmol 59: 217-22.
- Shah M. A, S. M. Shah. (2012) Ocular Trauma Score as a predictor of final visual outcomes in traumatic cataract cases in pediatric patients. J Cataract Refract Surg 38: 959-65.
- Shah M. A, S. M. Shah. (2012) OcularTrauma Score: a useful predictor of visual outcome at six weeks in patients with traumatic cataract. Ophthalmology 119:1336-41.
- Shah M. A, S. M. Shah. (2011) Comparative study of final visual outcome between open- and closed-globe injuries following surgical treatment of traumatic cataract. Graefes Arch Clin Exp Ophthalmol 249:1775-81.
- Shah M. A, S. M. Shah. (2011) Effect of interval between time of injury and timing of intervention on final visual outcome in cases of traumatic cataract. Eur J Ophthalmol 21: 760-5.





