Anatomical Differences of Corneal Surface Parameters
Benes P1,2, Holoubková Z2, Sylvie Petrová1,3
1 Department of Optometry and Orthoptics, Medical Faculty, Masaryk University, Brno, Czech Republic.
2 Ocni optika–RUBIN, Brno, Czech Republic.
3 Department of Ophthalmology and Optometry, St. Anne´s University Hospital, Brno, Czech Republic.
*Corresponding Author
Pavel Benes,
Ocní optika – Rubin, Makovskeho nam.2,
616 00 Brno, Czech Republic.
E-mail: optika.rubin@seznam.cz, 15347@med.muni.cz
Article Type: Case report
Received: August 08, 2014; Accepted: October 30, 2014; Published: October 30, 2014
Citation: Benes P, Holoubková Z, Sylvie Petrová (2014). Anatomical Differences of Corneal Surface Parameters. Int J Ophthalmol Eye Res. 2(7), 82-85. doi: dx.doi.org/10.19070/2332-290X-1400015
Copyright: Benes P© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The aim of this study was to analyze possible anatomical differences of corneal surface parameters in the sample
of population and between the genders.
Methods: This study is presenting the sample of population which has consisted of 1354 subjects, 794 female and 560 male
eyes. Subjects were chosen randomly. To determine and evaluate all values of corneal surface parameters, auto refractor
keratometer with Placido disc (KR 8100P, Topcon, Japan) and the program Software Corneal Analyzer, Version 3.0 were
used. The results were registered and then processed statistically.
Results: From a large amounts of data, tere are chosen only the results in this study that showed statistically significant (p<0. 05) differences between right and left eye and between the genders. Found variations are in: the steepest meridian, the axis of the steepest meridian, corneal astigmatism, astigmatic difference and corneal diameter (HVID).
Conclusion: The study shows that in optometric practice is also important to pay attention not only to functional but also individual anatomical parameters of corneal surface.
2.Introduction
3.Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Cornea, Anterior Surface, Astigmatism, Topography, Population.
Introduction
Distinguishing between left and right sides is one of the fundamental properties of nature. Scientists claim that the environment we know is due to other things because there are differentiates between right and left side. This is done consistently, from elementary particles to the human brain. Similar lateral anatomical differences visible to the unaided eye validated measurement or visible in the imaging was found numerous. The human eye is a paired organ. Thanks positioned eyes together we are able to perceive space. Eye, organ of vision, is among the sensory organs. It brings up to three quarters of all our perceptions. It allows us to perceive our surrounding through the light that reflects from him. Light is electromagnetic waving. Rays of light are focused onto the retina by optical system surfaces. The amount of transmitted light is modulated activities of the iris that changes the diameter of the pupil.
Changes in the optical power of the eye or the lens itself cause inaccurate impact of light rays on the retina, nearsightedness (myopia) or farsightedness (hyperopia). Human cornea is a very important tissue involved in the mediation of visual perception. It is necessary to measure its shape and pay attention especially in the case of correction of refractive errors and the possibility of ectatic corneal dystrophies [1,2]. Anterior eye are ocular tissue structures whose physiology and proper function is also influenced by wearing contact lenses. Nowadays many clients, especially teenagers give priority to wear contact lenses to correct their refractive error [2,4].
Contact lenses are medical-cosmetic invention fitted to corneal surface and to sclera partially. The must meet a number of criteria to have certain characteristics and parameters to the actual course of a successful fitting to minimize effects of this foreign body on the metabolism of the anterior eye in the result. Client undergo an examination in which refractive error and basic eye parameters are measured. The following is a selection of suitable type of contact lens with respect to the used material. Contact lenses provide wearers many benefits from unlimited visual field–which is limited by the shape of spectacle frames. For active and sportoriented clients they are irreplaceable [2,3].
But contact lens producers have a tendency to distribute these corrective aids only in very limited parameters. The experience of optometrists is that each corneal surface is different and therefore it is necessary to have more contact lenses parameters than only ranges are produced. Limited range then reduce the number of contact lens wearers and potential clients.
The aim of this study was to analyze possible anatomical differences of corneal surface parameters in the sample of population and between the genders.
Methods
This study is presenting the sample of population which has consisted of 1354 subjects, 794 female and 560 male eyes. Subjects for this study were chosen randomly. To determine and evaluate all values of corneal surface parameters, auto refractor keratometer with Placido disc (KR 8100P, Topcon, Japan) and the program Software Corneal Analyzer, Version 3.0 were used. For a detailed assessment of all parameters of the anterior eye serves sophisticated device that display the corneal tissue across its course. Repeatability of the data's on this device were evaluated based on three measurements obtained by the same optometrist of all clients. In optometric practice is a very popular method for monitoring the shape of the cornea corneal topography. In the form of color maps showing the values of radii of corneal anterior surface curvature in millimeters or directly in diopters. Corneal topography is an effective technique for detection of degenerative diseases and abnormalities of corneal tissue, such as keratoconus. Especially for teenagers and young clients served noninvasive detection and screening of potential degenerative changes of the cornea.
The results were registered and then processed statistically, statistical evaluations and analysis were performed by Statistical 10 (Stat Soft). The one-sample t-test, paired t test and one-way ANOVA were used for statistical significance. P values of less than 0.05 were considered to be statistically significant. Average of corneal values were expressed as mean±standard deviation. Differences in values among groups of gender and refractive errors were analyzed by one-way analysis of variance (ANOVA). The normal distribution of variables was assessed also by the Kolmogorov- Smirnov normality test. The other relationships were analyzed using Pearson correlation [1,3].
The study adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained before data collection from the adults or guardians as long as subjects fell under the defined study criteria.
Results
There were measured data that are important in optometric and ophthalmologic practice to evaluate anterior eye as: age, gender, objective refraction–sphere and cylinder with axis, subjective refraction– sphere and cylinder with axis, the steepest meridian with axis, the flattest meridian with axis, astigmatic difference–as the difference between the flattest and the steepest meridians, corneal power, corneal mean eccentricity, also eccentricity in 10°and 30°, corneal diameter (HVID) measured white-to-white. The values were also marked for each eye to compare the possible differences between eyes. Values of vision function we didn´t need for this type of study.
From a large amounts of data, here are chosen only the results that showed statistically significant (p<0.05) differences between right and left eye and between the genders. Found variations are in: the steepest meridian, the axis of the steepest meridian, corneal astigmatism, astigmatic difference and corneal diameter (HVID).
There were found differences between right and left anterior eye parameters as follows: the steepest meridian curvature average in all groups (n=1354) is 7.65 mm±0.27 mm (min. 6.67 mm; max. 8.71 mm; median 7.66 mm). In side difference between genders are values of right eyes: females 7.62 mm±0.27 mm (min. 6.67 mm; max. 8.44 mm; median 7.62 mm), males 7.70 mm±0.26 mm (min. 6.98 mm; max. 8.62 mm; median 7.71 mm). Left anterior surface has these values: females 7.62 mm±0.28 mm (min. 6.88 mm; max. 8.71 mm; median 7.61 mm) and males 7.69 mm±0.28 mm (min. 6.69 mm; max. 8.52 mm; median 7.70 mm), p value is p=.0000, (Table 1).


Table 1. Parsing table of descriptive statistics, differences of lateral eyes of the men and women and the values of the radii of curvature of the steepest meridian (mm) in the list of dependent variables are CHD). Kruskal-Wallis ANOVA based on the ranking; The steepest meridian r1 (mm), independent (group) variable Lateral differences, Kruskal-Wallis test: H (3, N=1354) =27,76636; p =,0000.
The other parameter is axis of the steepest meridian, in the whole group are values like this: 89.85°±38.18° (min. 0°; max. 180°; median 90°). The side difference is then: females right eyes84.58°±34.73° (min. 0°; max. 180°; median 95°), males right eyes89.43°±43.64° (min. 0°; max. 180°; median 105°). Values of left eyes are as follows: females 94.65°±34.58° (min. 1°; max. 180°; median 103°), males 91.09°±41.08° (min. 0°; max. 180°; median 107°), value of p=.0011 (Table 2).
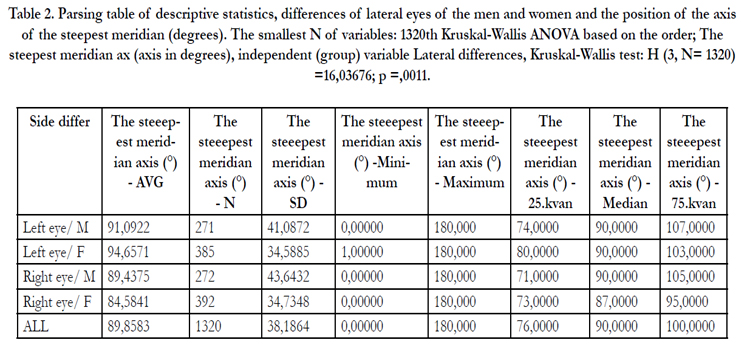
Table 2. Parsing table of descriptive statistics, differences of lateral eyes of the men and women and the position of the axis of the steepest meridian (degrees). The smallest N of variables: 1320th Kruskal-Wallis ANOVA based on the order; The steepest meridian ax (axis in degrees), independent (group) variable Lateral differences, Kruskal-Wallis test: H (3, N= 1320) =16,03676; p =,0011.
The next parameter was found in the difference between the flattest and the steepest meridians–the size of astigmatic difference of two main meridians. In all groups are those results: avg. value is 0.13 mm±0.10 mm (min. 0.0 mm; max. 0.99 mm; median 0.11 mm). The side difference between eyes are as follows: females right eyes 0.14 mm±0.11 mm (min. 0.0 mm; max. 0.93 mm; median 0.19 mm), males 0.11 mm±0.08 mm (min. 0.0 mm; max. 0.69 mm; median 0.14 mm). Left eyes has these values: females 0.14 mm±0.10 mm (min. 0.0 mm; max. 0.75 mm; median 0.18 mm) and males 0.12 mm±0.10 mm (min. 0.0 mm; max. 0.99 mm; median 0.16 mm), p value is p=. 0000 (Table 3).
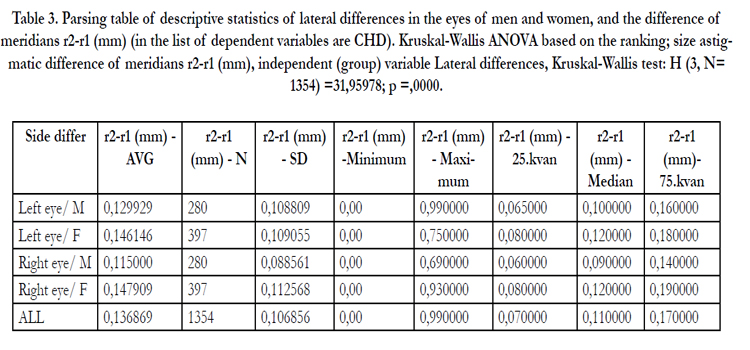
Table 3. Parsing table of descriptive statistics of lateral differences in the eyes of men and women, and the difference of meridians r2-r1 (mm) (in the list of dependent variables are CHD). Kruskal-Wallis ANOVA based on the ranking; size astigmatic difference of meridians r2-r1 (mm), independent (group) variable Lateral differences, Kruskal-Wallis test: H (3, N=1354) =31,95978; p =,0000.
Another parameter with differences was in corneal astigmatism. In all groups are following values: -0.75 D±0.60 D (min. 0.0 D; max. -5.99 D; median -0.60 D). Females right eyes -0.81 D±0.64 D (min. 0.0 D; max. -5.30 D; median -0.68 D), males -0.63 D±0.47 D (min. 0.0 D; max. -0.78 D; median -0.52 D) and left eyes are at females -0.79 D±0.60 D (min. 0.0 D; max. -0.99 D; median -0.68 D), males -0.71 D±0.63 D (min. 0.0 D; max. -5.99 D; median -0.54 D), the p value was p=.0000 (Table 4).
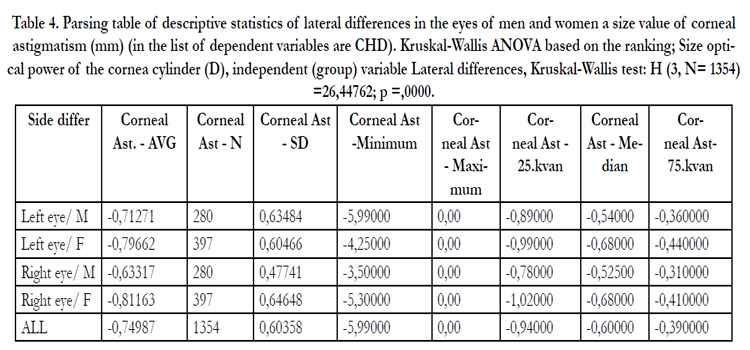
Table 4. Parsing table of descriptive statistics of lateral differences in the eyes of men and women a size value of corneal astigmatism (mm) (in the list of dependent variables are CHD). Kruskal-Wallis ANOVA based on the ranking; Size optical power of the cornea cylinder (D), independent (group) variable Lateral differences, Kruskal-Wallis test: H (3, N= 1354)=26,44762; p =,0000.
The last parameter where we found differences was corneal diameter (HVID), in all groups we measured 12.01 mm±0.35 mm (min. 10.69 mm; max. 13.27 mm; median 12.00 mm). Females right eyes were 11.96 mm±0.35 mm (min. 11.04 mm; max. 13.27 mm; median 11.96 mm), males 12.07±0.34 mm (min. 11.13 mm; max. 13.02 mm; median 12.08 mm). Left eyes has these values– females 11.96 mm±0.35 mm (min. 10.69 mm; max. 13.18 mm; median 11.98 mm), males 12.08 mm±0.35 mm (min. 11.12 mm; max. 13.27 mm; median 12.09 mm), p value is p=.0000 (Table 5).
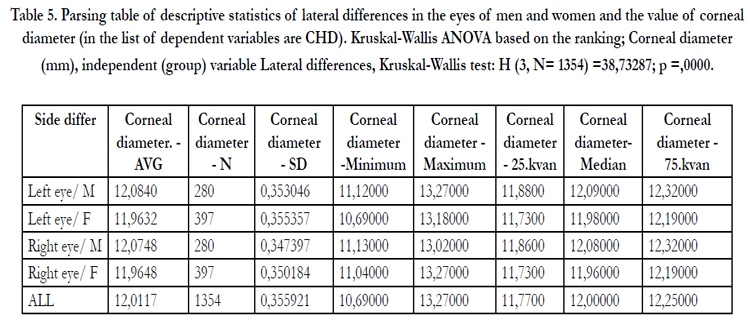
Table 5. Parsing table of descriptive statistics of lateral differences in the eyes of men and women and the value of corneal diameter (in the list of dependent variables are CHD). Kruskal-Wallis ANOVA based on the ranking; Corneal diameter (mm), independent (group) variable Lateral differences, Kruskal-Wallis test: H (3, N= 1354) =38,73287; p =,0000.
Discussion
The main benefit of aspheric surfaces in general is a precise optical imaging and limitations of spherical and chromatic aberration errors which is primarily important to increase the visual impact performance. This is most obvious especially in technology and construction of corrective appliances, such as spectacle lenses and contact lenses with aspheric surface.
Most sophisticated methods, e.g. aberrometry still has a significant position in the assessment of refractive errors and their correction methods. The current software equipment of new measuring instruments calculates automatically the spherical aberration of the anterior surface of cornea. Higher-order aberrations are errors in the optical imaging that cannot be corrected without the available tools. The aim in clinical practice is achieving the highest possible results in a solution or cataract refractive surgery to reduce or completely eliminate these aberrations and improve visual function. If after surgery the signification of these defects in perception appear as halo effects, haze and glare are then very distracting.
To anatomical differences of corneal surfaces and their differences emphasis must be placed because a lot of distributors produce only “unifit” shaped soft contact lenses which can be sometimes contraindication for proper fitting [1,3].
In this study we also demonstrated high repeatability for the anterior corneal curvature for the flattest, steepest and peripheral meridians of the corneal curvatures.
In case of selecting appropriate parameters of contact lenses are undoubtedly assessing topographic maps of the anterior surface of cornea determination of the flattest and the steepest meridian, respectively values of eccentricity. Its course varies depending on the corneal shape [1,4].
Knowledge of production technology, materials, water content, oxygen permeability, refractive index, modulus, wettability, surface quality, the stability of the lens in an environment prone to fouling, biocompatibility and ease of handling for the client are the criteria for recommending suitable corrective contact lenses as a corrective aids.
Free availability of these products on the market especially the unregulated internet boom can damage vision of the wearer seriously and permanently. Appellations on the distributing companies are misguided. The main drawback is the possible complications caused by poor or no education of patients especially in the area of disinfection and proper hygiene when handling contact lenses [2,4].
Conclusion
Regular visits at eye care practitioners and proper care of contact lenses are then success while wearing these corrective aids. According to the medical indication and the status of the client can then be chosen from various types of corrective aids. There are mainly spectacles and contact lenses. The results taken from the measurements then easily and clearly interpreted as to discuss with the client. Any client´s request is needed professionally evaluate, recommend follow other specialists examinations which can prevent potentially serious ocular complications and diseases. The study shows that in optometric practice is also important to pay attention not only to functional but also individual anatomical parameters of corneal surface.
References
- GONZALEZ-MEIJOME JM, VILLA-COLLAR C, MONTES-MICO R, GOMES A. (2007) Asphericity of the anterior human cornea with different coneal diameters. Journal of Cataract and Refractive Surgery 3: 465.
- BENEŠ P. (2012) Čes a slov. Oftal 1: 48
- EFRON N. (2010) Contact lens practice (Butterworth HeinemannElsevier) www.thevisioncareinstitute.com/sites/default/files/content/common/EFRON%20Grading%20Scale%20US%20INSERT.pdf.
- BENEŠ, Pavel. (2011) Důkladná dezinfekce a správná péče o kontaktní čočky. Česká oční optika 3:80-84.





