Can Spectral-Domain Optical Coherence Tomography Findings Forecast Visual Outcome in the Case of Macular Edema?
Shah M*, Shah S, Upadhyay P, Kalyani P, Ritu P
Drashti Netralaya, Dahod, Gujarat, India.
*Corresponding Author
Mehul A. Shah MD,
Drashti Netralaya, Nr. GIDC,
Chakalia Road, Dahod-389151,
Gujarat, India.
Tel: 00-91-2673-645364
Fax: 00-91-2673-221232
E-mail: omtrust@rediffmail.com
Article Type: Case report
Received: September 12, 2014; Accepted: October 25, 2014; Published: October 28, 2014
Citation: Shah M, Shah S, Upadhyay P, Kalyani P, Ritu P (2014). Can spectral-domain optical coherence tomography findings forecast visualoutcome in the case of macular edema?. Int J Ophthalmol Eye Res. 02(7),77-81. doi: dx.doi.org/10.19070/2332-290X-1400014
Copyright: Shah MA© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: To evaluate the relationship between visual outcome and the photoreceptor inner segment/outer segment (IS/
OS) layer status in patients with macular edema of any etiology.
Design: Cross-sectional study
Patients with macular edema of any etiology and who did not present with a disrupted IS/OS line were enrolled.
We obtained simultaneous visual acuity and optical coherence tomography (OCT) of patients with macular edema using a spectral-domain (SD) OCT system. The device recorded retinal thickness on tomography. SD OCT was recorded repeatedly in patients before and after treatment with an anti-vascular endothelial growth factor agent or triamcinolone, and the central thickness, IS, and OS were measured. The IS/OS ratio was calculated, and the data were analyzed statistically. We also reviewed the OCT scans to determine the type of macular edema, i.e., cystoid macular edema or diffuse macular edema (absence of any cysts).
Results: Forty-eight patients (48 eyes: 21 male and 27 female; median age, 58.50 ± 10.8 years) with macular edema were enrolled.
Twenty-seven eyes had cystoid macular edema, and 10 eyes had diffuse macular edema. The median central subfield thickness was 462 ± 150.3 μm. The IS/OS layer was observed in all 48 eyes, and the IS/OS ratio was calculated.
Eight (16.7%), 11 (22.9%), and 29 (60.4%) eyes had venous tributary occlusion, post-cataract cystoid macular edema, and diabetic macular edema, respectively.
There was a significant difference between pre- and post-treatment vision (p = 0.001, Table 2). When we compared the pre and post treatment IS, OS, and IS/OS ratio with t test (p = 0.000 with 95% CI).
The presenting vision differed significantly according to the IS/OS ratio (p = 0.010, Table 3).
Conclusion: This study demonstrated that the IS/OS ratio is not significantly correlated with final visual acuity following treatment for macular edema.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Macular Edema; SD OCT; IS/OS; Determinants of Visual Outcome in Macular Edema.
Introduction
Macular edema is a complication of many ocular conditions and currently affects an estimated 8% to 10% of the 23.6 million diabetics in the U.S. [1] Because the prevalence of diabetes is expected to grow to more than 300 million cases worldwide by 2025, [2] the prevalence of macular edema is also expected to increase substantially.
The development of macular edema is initiated by hyper-permeability of the retinal vasculature, allowing extracellular fluid to accumulate in the retina. Ischemic dysfunction of the neuroglia cells due to macular edema results in visual disturbance.[3] Therapeutic strategies such as treatment with an anti-vascular endothelial growth factor drug, [4] steroids, [5] or laser photocoagulation, [6] have been used to control macular edema. However, complete resolution of the condition is not always possible, and a better understanding of the pathophysiology of macular edema is necessary.
Recent advances in optical coherence tomography (OCT) technology, including the development of high-resolution spectraldomain (SD) OCT, have facilitated the visualization of outer retinal changes that may be important indicators of the functional integrity of the visual pathway. The disruption of the junction between the inner segment/outer segment (IS/OS) layers of photoreceptors and the external limiting membrane has been shown to be a factor in retinal dysfunction.[7-12] Initial studies of retinal vein occlusion demonstrated that the disruption of the IS/OS junction is highly correlated with decreased visual acuity (VA)[7] and visual outcome.[8] Subsequent studies have demonstrated similar associations between IS/OS status and visual acuity in age-related macular degeneration [9] and diabetic macular edema (DME).[11,12] These studies of DME have relied on VA, which is a clinically useful, global measure of macular function. However, VA may poorly reflect focal changes in retinal function and structures in more localized diseases (Figure 1).
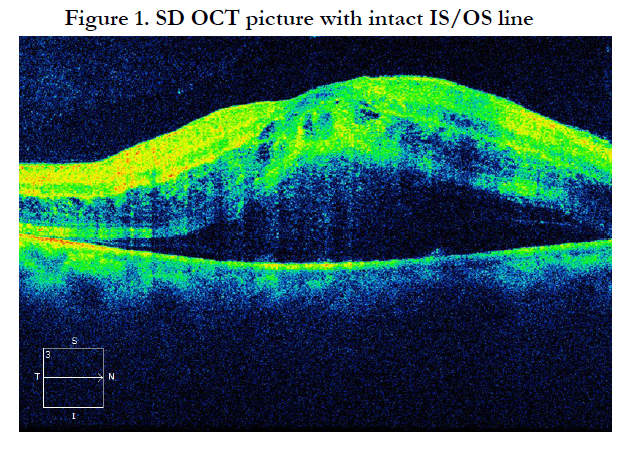
Figure 1. SD OCT picture with intact IS/OS line
Hatef et al.[14] demonstrated a strong relationship between macular sensitivity and point thickness in macular edema, whereas Sepah et al. [15] illustrated similar findings in eyes with uveitic macular edema. In another recent study, [10] the integrity of the photoreceptor layer was shown to be an important determinant of the effect of macular thickness on VA in patients with DME. Visual acuity was correlated with parafoveal thickness in patients who had an intact photoreceptor layer, whereas VA was not associated with parafoveal thickness in patients who had a disrupted photoreceptor layer. It is not known whether the presence or absence of the IS/OS layer affects the relationship between point sensitivity and point thickness. [14] (Fugure 2)
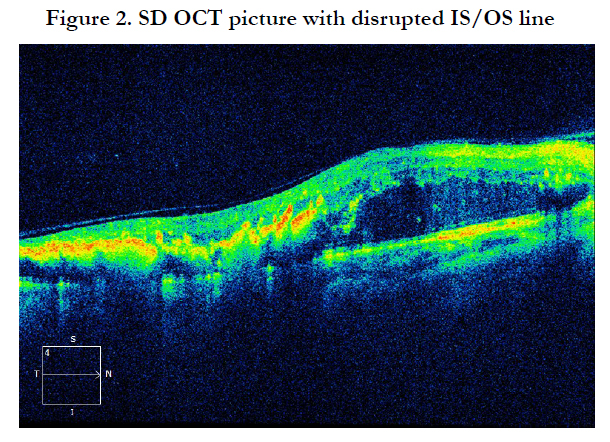
Figure 2. SD OCT picture with disrupted IS/OS line
In this study, we assessed the association between the visual outcome and the IS/OS ratio in cases of macular edema with a nondisrupted photoreceptor layer.
Materials and Methods
We performed a cross-sectional study of adult patients diagnosed with macular edema managed at Drashti Netralaya, Dahod, Gujarat, India. Our research followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board/ Ethics Committee. Informed consent was obtained from all participating subjects.
Inclusion criteria were a diagnosis of macular edema confirmed by a retina specialist using contact lens biomicroscopy and OCT and findings indicating clinically significant macular edema with an intact IS/OS line, increased central point thickness, and the presence of fluid. Leakage observed by fluorescein angiography was assessed to support the diagnosis of macular edema. Only OCT scans with signal strength greater than 6/10 were included in the study. Patients who had received focal or grid laser therapy that produced scarring in the area were excluded because we believe that extensive laser treatment may artificially disrupt the IS/OS junction. Study data collected at the time of the imaging visit included best-corrected VA measured using the Early Treatment Diabetic Retinopathy Study chart and any prior treatments for macular edema. We also collected demographic data, including age, gender, and race, from the patients’ medical records. We treated the patients with ranibizumab or triamcinolone, or with no treatment according to pathology.
The IS/OS junction was defined as the hyper-reflective line between the inner and outer segments of the photoreceptors, just above the hyper-reflective line representing the retinal pigment epithelium and just below the hyper-reflective line representing the external limiting membrane. The IS/OS junction status was either present or absent. The IS and OS were measured for all eyes with an intact junction. When the initial grader was unable to accurately determine whether the IS/OS junction was disrupted at a particular point, a second expert grader was consulted, and the presence or absence of the IS/OS junction was determined by consensus. The Spectral OCT/SLO software automatically calculated retinal thickness, defined as the distance between the inner limiting membrane and the retinal pigment epithelium.[16] We calculated the IS, the OS, and the IS/OS ratio.
The data were analyzed using bivariate analysis with t-tests, including robust variance estimates for clustering within eyes to compare the main study variables at points with IS/OS ratio versus VA. In addition, the association between the IS/OS ratio and post-treatment VA was analyzed.
Results
Forty-eight patients with macular edema (48 eyes; 21 males and 27females; median age, 58.50 ± 10.8 years; Table 1) were enrolled. Twenty-seven eyes had cystoid macular edema, and 10 eyes had diffuse macular edema. The median central subfield thickness was 462 ± 150.3 μm. The IS/OS layer was observed in all 48 eyes, and the IS/OS ratio was calculated.
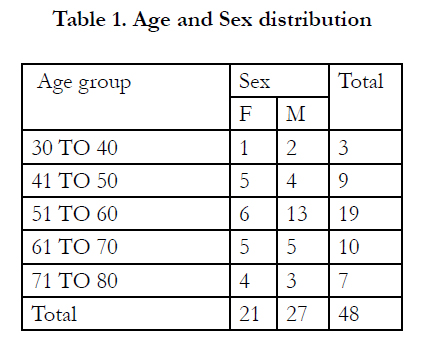

Table 1. Age and Sex distribution
Eight (16.7%), 11 (22.9%), and 29 (60.4%) eyes had venous tributary occlusion, post-cataract cystoid macular edema, and DME, respectively.
There was a significant difference between pre- and post-treatment vision (p = 0.001, Table 2). The presenting vision differed significantly according to the IS/OS ratio (p = 0.010, Table 3), but we did not observe any significant difference according to etiology. (p = 0.589, Table 4).
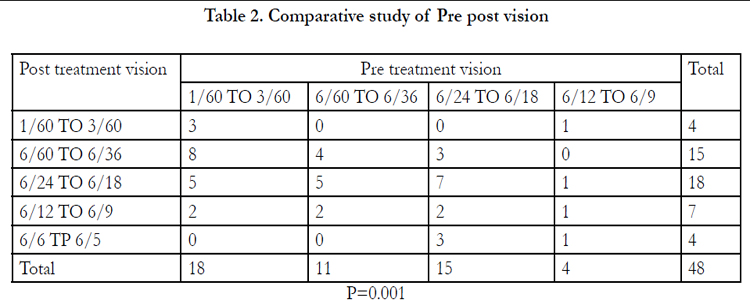
Table 2. Comparative study of Pre post vision
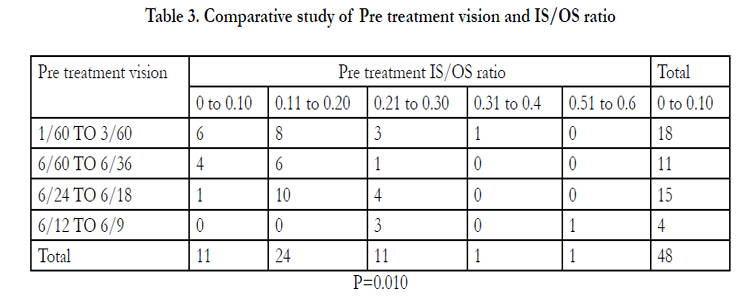
Table 3. Comparative study of Pre treatment vision and IS/OS ratio
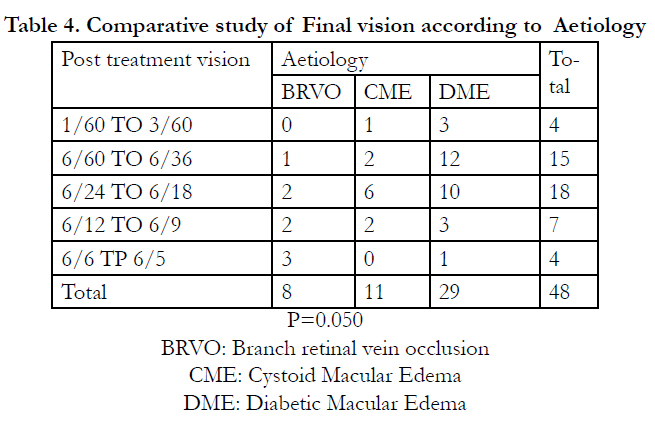
Table 4. Comparative study of Final vision according to Aetiology
When we compared pre- and post-treatment IS, OS, and IS/OS ratio values with t-test (p = 0.000 95% CI Table 5).
When we compared the pre-treatment vision, IS, and IS/OS ratio, we observed a significant difference (p = 0.047, 0.010, Table 5).
When we compared the final VA, the IS, OS, and IS/OS ratio did not show a significant difference (p = 0.371, 0.235, 0.133, Table 5).
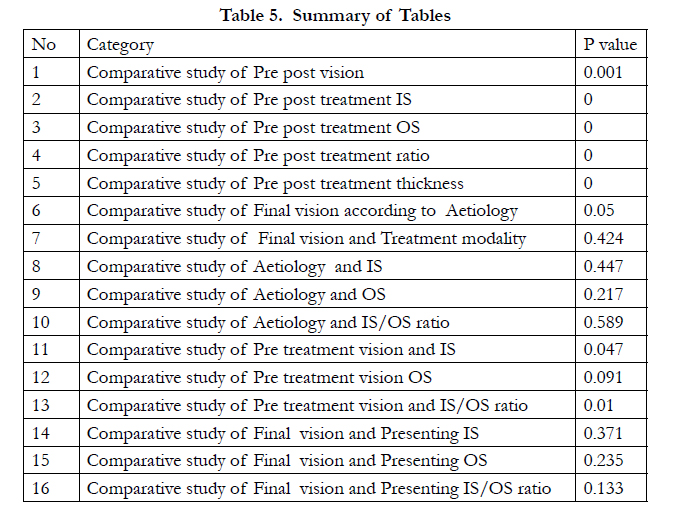
Table 5. Summary of Tables
Discussion
In this study, we used a novel approach to analyze the IS/OS ratio and examined the relationship between the IS/OS ratio and VA in patients with macular edema and an intact IS/OS line. Our study suggests that an intact IS/OS junction in macular edema is a predictor of good VA. Prior studies have shown that disruption of the IS/OS junction is a factor in retinal dysfunction [11,12]
To our knowledge, this is the first report investigating the relationship between the IS/OS ratio and VA. Our findings suggest that the integrity of the local photoreceptor layer, as indicated by the IS/OS ratio, is a strong predictor of local visual function throughout the retina.
Recent studies have suggested that the IS/OS status is a good prognostic indicator for DME therapy. One study [18] showed that patients with an intact IS/OS layer tended to respond better to triamcinolone treatment. Another recent study reported that the IS/OS status was a good predictor of visual outcome in patients treated with pars plana vitrectomy. [19] Although we agree that patients with IS/OS disruption may have reduced VA, our results suggest that in patients with macular edema, retinal thickness remains an important predictor of visual function, independent of IS/OS status. Therefore, in edematous patients, the clinician should strive to reduce macular edema regardless of the IS/OS status.
We found that the presence of cysts along with edema (cystoid macular edema) results in decreased VA, similar to findings in other studies. [10,20] The presence of cysts was significantly associated with retinal thickness and tended to be associated with increased IS/OS disruption. Our model revealed that the presence of cysts was associated with decreased functioning in macular edema, independent of their effects on retinal thickness and IS/OS disruption. Cysts, which usually occur in the inner nuclear layer or outer plexiform layer, [21,22] have been hypothesized to act by disrupting bipolar or ganglion cells. [10] Our findings, that cysts have an effect independent of their effects on retinal thickness and photoreceptor disruption, support this hypothesis.
A disrupted IS/OS line is an established determinant for poor visual outcome in case of DME. [23-25] We wanted to study how vision is affected when the IS/OS line is undisrupted.
Disruption of the IS/OS junction is associated with a significant 3.28-dB decrease in retinal sensitivity, after adjusting for confounding variables. In addition, we found that IS/OS disruption results in a weaker thickness-sensitivity association at retinal points thinner than 300 μm. However, we also found that IS/OS disruption has no effect on the relationship between thickness and sensitivity at points thicker than 300 μm and that the external limiting membrane (a close correlate of the IS/OS junction) [9] at the fovea results in a decreased VA measured by standard testing. [23]
When the retinal thickness was <300 μm, the thickness-sensitivity relationship was weaker with a disrupted IS/OS layer than with an intact IS/OS layer. This suggests that when the IS/OS layer is disrupted in retinas thinned by atrophic degeneration, retinal thickness is no longer a strong predictor of visual function, although thickness remains an important predictor of visual function when the IS/OS layer is disrupted at points thicker than 300 μm. [23] Therefore, in edematous retinas, thickness tends to have an effect independent of photoreceptor disruption. This finding may lend credence to the standard approach of today's retina specialists to maximize resolution of edema in patients with macular edema. [23]
Kim and Shin reported that IS/OS line disruption is an important determinant of vision following treatment for venous occlusion. [24] Hood concluded that the inner segment ellipsoid band, previously termed the IS/OS line, is of clinical significance, favoring better visual outcome in any macular edema. [25] Shin found a similar relationship in DME. [18] Landa et al. reported that the integrity of the IS/OS line has a significant relationship to visual outcome in cases of age-related macular degeneration, [16] and Aizawa described a similar relationship in retinitis pigmentosa. [26] We are not aware of any study reporting the relationship between the IS/OS ratio and visual outcome.
The present study has several limitations. First, the study sample was relatively small. In addition, there was possibility of residual confounding in our analysis. We did not have data to control or model for duration, severity, prior treatments, and any concurrent ophthalmologic conditions. Finally, because this was a cross-sectional study, it is difficult to establish temporality of the exposure (IS/OS ratio) and the outcome (visual acuity).
Conclusion
The absence of the IS/OS layer has a significant impact on vision in patients with macular edema. The present results show that retinal thickness is an important predictor of retinal function in edematous macula when the IS/OS layer is not disrupted. The IS/OS ratio may differ significantly on presentation, but the final vision outcome is not significantly associated with the integrity of the IS/OS layer.
References
- Chen E , Looman M , Laouri M. (2010) Burden of illness of diabetic macular edema: literature review. Curr Med Res Opin 26:1587–1597.
- Sjostrand J , Popovic Z , Conradi N , Marshall J. (1999) Morphometric study of the displacement of retinal ganglion cells subserving cones within the human fovea .Graefes Arch Clin Exp Ophthalmol 237:1014–1023.
- Antonetti DA , Barber AJ , Bronson SK. (2006) JDRF Diabetic Retinopathy Center Group Diabetic retinopathy: seeing beyond glucose-induced microvascular disease . Diabetes 55:2401–2411.
- Elman MJ , Aiello LP , Beck RW. (2010) Diabetic Retinopathy Clinical Research Network Randomized trial evaluating ranibizumab plus prompt ordeferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 117:1064–1077.
- Martidis A, Duker JS, Greenberg PB. (2002) Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology 109:920–927.
- Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report no. 4. Int Ophthalmol Clin.(1987) 27:265–272.
- Ota M, Tsujikawa A, Murakami T. (2007) Association between integrity of foveal photoreceptor layer and visual acuity in branch retinal vein occlusion.Br J Ophthalmol 91:1644–1649.
- Shin HJ, Chung H, Kim HC. (2011) Association between integrity of foveal photoreceptor layer and visual outcome in retinal vein occlusion [report online].Acta Ophthalmol 89:e35–e40.
- Oishi A, Hata M, Shimozono M. (2010) The significance of external limiting membrane status for visual acuity in age-related macular degeneration.Am J Ophthalmol 150:27–32.
- Murakami T, Nishijima K, Sakamoto A. (2011) Association of pathomorphology, photoreceptor status, and retinal thickness with visual acuity in diabetic retinopathy. Am J Ophthalmol 151:310–317.
- Maheshwary AS , Oster SF , Yuson RM. (2010) The association between percent disruption of the photoreceptor inner segment-outer segment junction and visual acuity in diabetic macular edema. Am J Ophthalmol 150:63–67.
- Otani T , Yamaguchi Y , Kishi S. (2010) Correlation between visual acuity and foveal microstructural changes in diabetic macular edema. Retina 30:774–780.
- Vujosevic S , Midena E , Pilotto E. (2006) Diabetic macular edema: correlation between microperimetry and optical coherence tomography findings. Invest Ophthalmol Vis Sci 47:3044–3051.
- Hatef E , Colantuoni E , Wang J. (2011) The relationship between macular sensitivity and retinal thickness in eyes with diabetic macular edema. Am J Ophthalmol 152:400–405.
- Sepah YJ , Hatef E , Colantuoni E. (2012) Macular sensitivity and fixation patterns in normal eyes and eyes with uveitis with and without macular edema. J Ophthalmic Inflamm Infect 2:65–73.
- Landa G, Rosen RB, Garcia PM , Seiple WH. (2010) Combined threedimensional spectral OCT/SLO topography and microperimetry: steps toward achieving functional spectral OCT/SLO. Ophthalmic Res 43:92–98.
- Panozzo G , Gusson E , Parolini B, Mercanti A. (2003) Role of OCT in the diagnosis and follow up of diabetic macular edema. Semin Ophthalmol 18:74–8.
- Shin HJ , Lee SH , Chung H , Kim HC. (2012) Association between photoreceptor integrity and visual outcome in diabetic macular edema. Graefes Arch Clin Exp Ophthalmol 250:61–70.
- Sakamoto A, Nishijima K, Kita M. (2009) Association between foveal photoreceptor status and visual acuity after resolution of diabetic macular edema by pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol 247:1325–1330.
- Soliman W, Hasler P, Sander B , Larsen M. (2012) Local retinal sensitivity in relation to specific retinopathy lesions in diabetic macular oedema. Acta Ophthalmol. 90:248–253.
- Tso MO. (1982) Pathology of cystoid macular edema. Ophthalmology 89:902–915.
- Yanoff M, Fine BS, Brucker AJ, Eagle RC. (1984) Pathology of human cystoid macular edema. Surv Ophthalmol. 28:505–511.
- Yohannan J, M. Bittencourt. (2013) Association of retinal sensitivity to integrity of photoreceptor inner/outer segment junction in patients with diabetic macular edema. Ophthalmology 120: 1254-61.
- Kim M, S. Y. Yu. (2012) Intravitreal ranibizumab for macular edema secondary to retinal vein occlusion.Ophthalmologica 227: 132-8.
- Hood D. C, X. Zhang. (2011) The inner segment/outer segment border seen on optical coherence tomography is less intense in patients with diminished cone function. Invest Ophthalmol Vis Sci 52: 9801-9.
- Aizawa S, Y. Mitamura. (2009) Correlation between visual function and photoreceptor inner/outer segment junction in patients with retinitis pigmentosa.Eye 23: 304-8.





