Glaucoma knowledge in a black community in Toronto
Jin YP1,2,*, Miller G3, Lin K4, Trope GE1
1 Ophthalmology & Vision Sciences, University of Toronto, Toronto, ON, Canada;
2 Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada;
3 Department of Ophthalmology, The Ottawa Hospital, The University of Ottawa Eye Institute, Ottawa, ON, Canada;
4 Faculty of Arts and Science, University of Toronto, Toronto, ON, Canada
*Corresponding Author
Jin YP,
Department of Ophthalmology and Vision Sciences,
University of Toronto ,Toronto, Ontario,
Canada M5T 3A9
Tel: 416-978-7938, Fax: 416-978-4590
E-mail: Yaping.Jin@utoronto.ca
Article Type: Research Article
Received: August 08, 2014; Accepted: August 20, 2014; Published: August 22, 2014
Citation: Jin YP, Miller G, Lin K, Trope GE. (2014). Glaucoma knowledge in a black community in Toronto, Int J Ophthalmol Eye Res, 2(5), 59-64. doi: dx.doi.org/10.19070/2332-290X-1400011
Copyright: Jin YP© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Black people are at high risk of glaucoma. Routine eye exams are the only way of identifying early glaucoma for treatment and blindness prevention. Public education on glaucoma risk factors and detection may be an important public health strategy to encourage those at high risk to have their eyes checked.
Purpose: To evaluate glaucoma knowledge (including presentation, risk factors and detection) and associated socio-demographic factors
in a black community in Toronto to aid the development of future public education programs.
Materials and Methods: Questionnaire surveys from 5 black people centered churches or organizations.
Results: The mean age of participants (n=201) was 48.7 years. Most participants reported glaucoma can cause blindness (88.6%) and run
in families (76.0%). However, only few participants (4%) correctly reported glaucoma affects peripheral vision. Over 1 in 4 participants (26.7%) reported incorrectly glaucoma always causes eye symptoms. Less than half of the participants knew black people are at higher risk of glaucoma (48.7%) and glaucoma most likely affects people 40 years or older (46.2%).
A history of parents or siblings with glaucoma was not associated with better knowledge of three established glaucoma risk factors (40 years or over, African origin and positive family history). Participants 40 years or older did not have greater knowledge than those under 40 that older people are at higher risk of developing glaucoma (prevalence ratio (PR)=0.90, 95% confidence interval (CI) 0.63-1.26). Participants with and without postsecondary education equally reported that eye examinations are the only way to identify glaucoma (PR=1.02,95% CI 0.72-1.46). Poverty was associated with lower levels of knowledge of the aforementioned three glaucoma risk factors and that glaucoma is identified through eye examinations.
Conclusion: Glaucoma knowledge in Toronto’s black community is inadequate. Education about glaucoma presentation, risk factors and
detection should be prioritized in this high-risk group.
2.Introduction
3.Materials and Methods
3.1.Statistical analysis
5.Results
6.Discussion
7.Conclusions
7.Acknowledgements
8.Financial support
9.References
Keywords
African Origin; Family History; Glaucoma Knowledge; Socio-Demographics; Toronto.
Introduction
Numerous studies have reported that black people are at higher risk of primary open-angle glaucoma (referred to as glaucoma in this study) than white people. For example, the Baltimore Eye Survey reported that the age-adjusted prevalence rates of glaucoma was four to five times higher in blacks than whites. [1] In the Salisbury Eye Evaluation Glaucoma Study, the prevalence of glaucoma among persons aged 75 years and older was 23.2% in blacks compared to 9.4% in whites.[2] Furthermore, studies in the USA and Barbados report that blindness rates due to glaucoma are higher in blacks than in whites and that glaucoma is the leading cause of blindness amongst black people.[3-4] In Canada, an ecologic study showed that higher blindness registration rates were associated with areas that had a higher percentage of the population who were black.[5]
Glaucoma usually has no noticeable symptoms until the later stages of the disease.[6-7] Early detection and treatment are the only known methods of preventing blindness from glaucoma. In North America, more than half of the glaucoma patients are diagnosed at routine eye examinations.[8,9] In Canada, amongst those with newly diagnosed glaucoma, half have moderate or advanced disease upon first diagnosis.[10] Routine screening for glaucoma at the population level however is not recommended due to low cost effectiveness.[11-12] Identifying, or incentivizing, high risk groups to have an eye examination produces higher yield.[12] Consequently, public education on glaucoma risk factors and detection may be an important public health strategy to encourage those at high risk to have their eyes checked. In a study from Canada, Noertjojo and associates stated that an informed public is more likely to undertake disease prevention activities.[13] In Australia, those with better knowledge of common eye diseases were reported to be more likely under the care of an eye care professional.[14] A targeted educational strategy may be particularly important for black people - an established high-risk group for glaucoma. However, the first stage in developing any educational program is to understand the base level of disease knowledge in the targeted group. A search of the literature revealed a paucity of information on glaucoma awareness and knowledge amongst black people, though studies have reported relevant data on whites, Chinese and Indians.[14-20]
The purpose of this study was to evaluate glaucoma awareness and the level of knowledge of glaucoma presentation, risk factors, detection methods, and associated socio-demographic factors in a black community in Toronto, Canada.
Materials and Methods
Self-identified black people, aged 30 years or older, residing in Toronto, participating in social activities organized by five community groups (see Acknowledgements) were orally invited by one of us (GM) to complete a self-administered questionnaire. The questionnaire was completed on site, or taken home and returned completed to the confidentially sealed “drop box”.
There are no validated questionnaires on glaucoma awareness and knowledge. We therefore developed a new questionnaire based on questions used in prior published studies.[14-21] The questionnaire included 4 questions on common eye disease awareness (defined as having heard of glaucoma, cataracts, retinopathy and macular degeneration) and 12 specific questions on glaucoma knowledge (see Appendix 1). In addition, the survey questionnaire included 21 questions on socio-demographics, and 5 questions on eye care utilization. The questionnaire was tested in a pilot study before use in the main study. The study protocol was approved by the Research Ethics Board at the University of Toronto.
A correct or incorrect answer to each of the 12 questions on glaucoma knowledge was reported as a separate proportion. In addition, a summarized glaucoma score, with one point assigned for each correct answer, and zero point for each incorrect or “Don’t know” answer, was used to measure general understanding of glaucoma knowledge. This score ranged from 0 to 12, with higher scores indicating better understanding of glaucoma. The mean scores in two categorized socio-demographic groups were statistically tested using a Student t test.
We paid particular attention to questions concerning 3 established glaucoma risk factors (aged 40 or over, African ancestry and positive family history) and glaucoma detection (i.e. glaucoma identified via eye examinations). Answers to these 4 questions were linked to detailed socio-demographic factors through univariate and multivariate analyses. Differences in proportions for each of these 4 questions across different socio-demographic groups were statistically tested by Chi square test, or Fisher’s exact test if data were too sparse. The prevalence ratios (PR) which were derived from log-Poisson regression models were used to assess the association between each of the 4 selected glaucoma knowledge questions and associated socio-demographic factors, due to the common occurrence of the study outcome.[22-23]
Results
In all, 249 questionnaires were filled out. Thirty-one questionnaires contained missing information on age and 17 questionnaires were from persons aged 16-29 years. These were excluded, leaving 201 questionnaires for analysis.
The mean age of the participants was 48.7 years (SD 12.7 years). The majority were females (76.1%), immigrants (86.6%) and university or college educated individuals (78.1%).
About one in five participants (19.0%) were using eye drops. A similar proportion of participants (22.2%) reported parents with glaucoma. Siblings with glaucoma were reported in 11.3% of the participants. About 1/3 of people (30.2%) responded "Yes" to the question "Have any of your blood relatives become blind in one or both eyes (include even if no longer living)?"
Over 90% of the participants reported having heard about glaucoma and cataracts, which was significantly higher than the awareness for diabetic retinopathy and macular degeneration (Figure 1). Among those who had heard of glaucoma, the main source of information was through relatives/friends and eye doctors (Figure2). The usual media source for information was TV and the least common was radio (Figure 2).
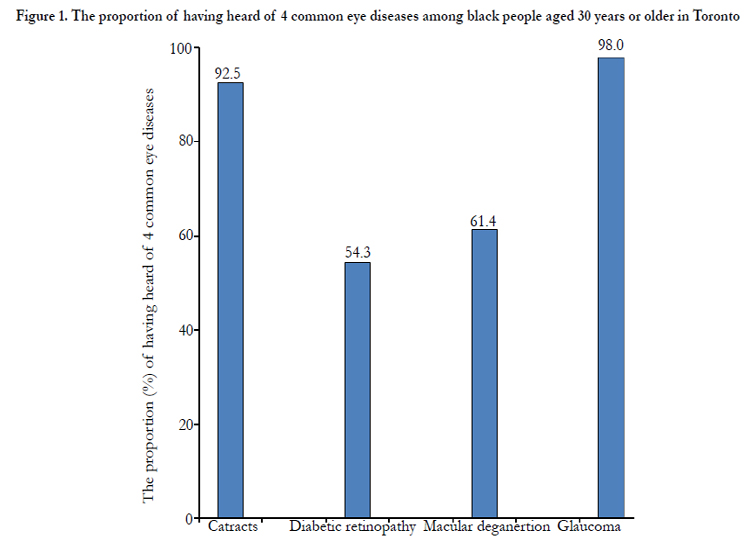
Figure 1. The proportion of having heard of 4 common eye diseases among black people aged 30 years or older in Toronto
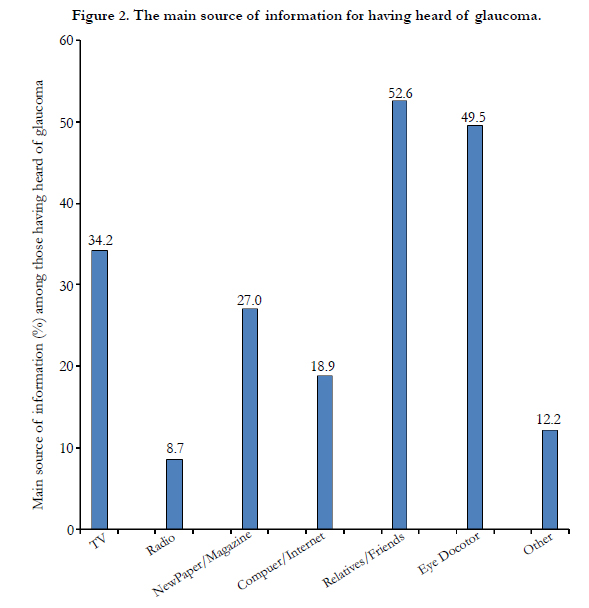
Figure 2. The main source of information for having heard of glaucoma.
Table 1 shows the 12 tested questions on glaucoma knowledge and the percentage answered correctly for each question. The majority of participants reported knowing that glaucoma causes blindness (88.6%) and runs in families (76.0%, Table 1). However, 11% of the participants did not believe or did not know that glaucoma causes blindness. Nearly 1/4 (24.0%) of the respondents reported not knowing glaucoma runs in family. Only 4% of the participants correctly recognized that glaucoma affects peripheral vision (Table 1). One in four participants (26.7%) reported glaucoma always causes eye symptoms such as eye pain.
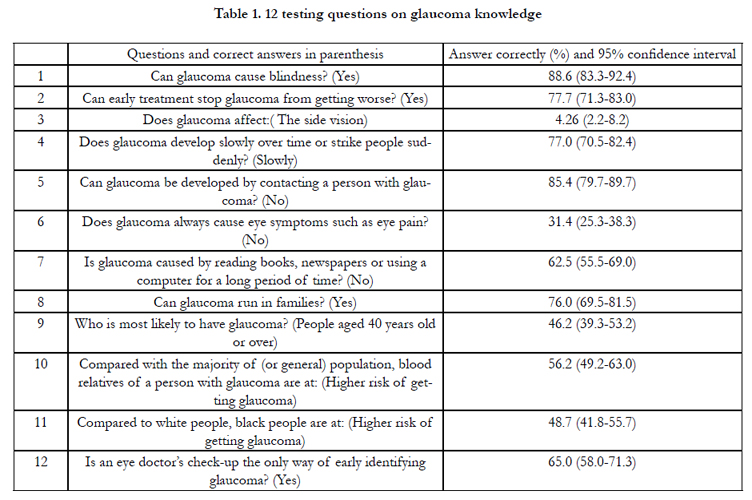

Table 1. 12 testing questions on glaucoma knowledge
Less than half of the participants reported that black people were at higher risk of glaucoma (48.7%) and glaucoma affects people 40 years or older (46.2%) (Table 1). Slightly over half (56%) of the participants reported that blood relatives of a person with glaucoma are at higher risk of developing glaucoma. Around 2/3 of the participants (65%) stated correctly that an eye doctor's check-up is the only way of identifying early glaucoma.
The mean glaucoma knowledge score was 7.07 (SD 2.62) out of a full score of 12. There were no significant differences on the average glaucoma score between socio-demographic groups, including age (under vs over 40 years of age, p=0.35), gender (men vs women, p=0.60), education (with vs without postsecondary education, p=0.39), parents having glaucoma (p=0.13), or those currently using eye drops (p=0.43).
Participants with a university or college education have increased knowledge regarding advanced age as a risk factor for glaucoma (PR=1.82, Table 2, p<0.05) in univariate analysis. However, this educated group did not have improved knowledge that blood relatives are at an increased risk of glaucoma (PR=0.94, Table 2, p>0.05) and that eye examinations are the only way of early identifying glaucoma (PR=0.98, Table 2, p>0.05). In multivariate analysis, having a postsecondary education was not associated with correctly answering any of the four selected glaucoma questions (Table 2).
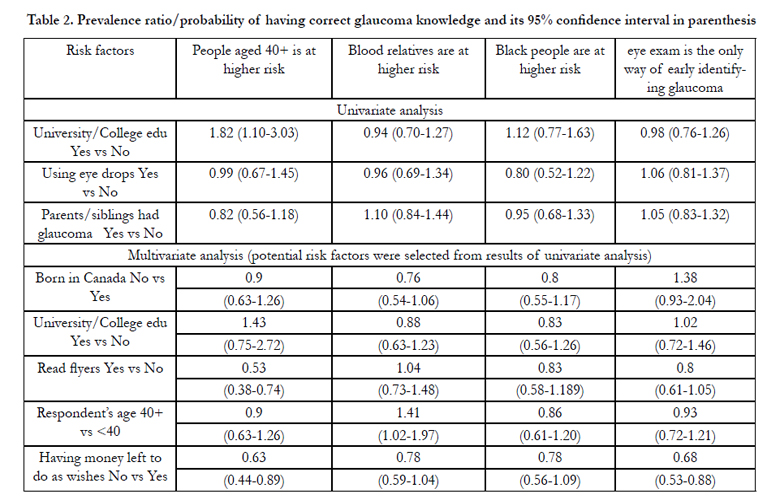
Table 2. Prevalence ratio/probability of having correct glaucoma knowledge and its 95% confidence interval in parenthesis
Current use of eye drops or having parents or siblings with glaucoma was not associated with improved knowledge regarding glaucoma risk factors and detection (Table 2). Participants aged 40 or over had improved knowledge about blood relatives and their increased risk of developing glaucoma (PR=1.41, Table 2, p<0.05). However, they did not know that older people are at higher risk of developing glaucoma (PR=0.90, Table 2, p>0.05).
Lack of money after all expenses are paid (i.e. poverty) is a risk factor for reduced glaucoma knowledge (Table 2). For example, compared to those with available funds, the poor, i.e. those without money “to do as they wish”, had a nearly 40% lower probability of knowing that age 40 years or above is a risk factor for developing glaucoma (PR=0.63, Table 2).
More than half of the participants (57%) reported not seeing an eye doctor (optometrist or ophthalmologist) in the past year. Major reasons were "I see well, therefore not necessary" (24.4%) and "Eye examination is expensive and can't afford to pay" (16.5%). Transportation (0.9%) and language (0%) problems were not reported as barriers to seeing an eye doctor.
Of those who visited an eye doctor in the past year, major reasons for having had such a visit included an eye check-up paid by OHIP (Ontario Health Insurance Plan) (29%) or by other health insurance plan (12%), need for new glasses (22%) and vision problems (14%).
A large proportion of the participants (37%) did not know that OHIP covers eye examinations once a year for residents younger than 20 years and older than 64 years. Nearly all participants (99.4%) preferred to receive health care information in English. Many participants (73.7%) read flyers delivered to a mailbox.
Discussion
Our results suggest that black people in Toronto are well aware of glaucoma (98%), know that it causes blindness (88.6%) and runs in families (76.0%). However, average knowledge regarding glaucoma presentation, risk factors and detection methods seems inadequate. Only a few participants (4%) reported glaucoma affects peripheral vision. Over 1/4 of the participants (26.7%) incorrectly reported glaucoma produces eye symptoms. With regards to the three established glaucoma risk factors, over half of the participants did not know that being of African descent places them at a higher risk of contracting the disease. Similarly, over half of the participants did not know that increased age (40 years or older) is a major risk factor for the disease. Surprisingly a family history of glaucoma in parents or siblings did not increase participants' awareness that they are at increased risk of developing glaucoma. This lack of glaucoma knowledge from a high-risk community is disturbing and suggests that educational efforts need to be focused on this high-risk group.
Studies on awareness and knowledge of glaucoma have been reported in other ethnic groups. In Hong Kong, glaucoma awareness was reported at 78.4%, but only 10.3% of the participants could describe the symptoms correctly.[18] In India, three glaucoma studies reported awareness rates of 0.27%, 2.4% and 13.3% - the lowest awareness rates documented in the literature to date. [19-21] In the USA, a telephone survey (n=368) reported that over 80% of respondents knew that glaucoma causes blindness, but approximately two-thirds of the sample could not identify even one risk factor.[15] In Australia, glaucoma awareness ranges from 79% to 93%.[14,16] The Australian studies also reported that high levels of education are associated with increased levels f glaucoma awareness and knowledge. In Germany, a face-toface interview revealed that 75% of the respondents (n=2742) had heard of glaucoma and that 25% of the respondents thought all people of different ages had an equal risk of developing glaucoma.[17] In Canada, a study of 33 family practitioners' patients in British Columbia reported that 41% of the participants (n=882) were familiar with glaucoma and that women and people with higher educational attainment were significantly more likely to report familiarity with the disease.[13] In an online survey (n=800) by the CNIB (Canadian National Institute for the Blind) in 2009, 70% of the respondents incorrectly reported that glaucoma has associated symptoms, with a third associating the disease with pain or a change in how their eyes feel.[24] In this study, we surprisingly report the highest level of glaucoma awareness documented to date (98%). These varied results may be explained in part by different study populations, different study periods and different study methods.
One contributing factor to the high level of glaucoma awareness in this study may be the high level of education of the participants: 78% of the participants in our study vs 49.9% of black Torontonians possess university or college education (p<0.0001).[25] High levels of education are associated with high levels of glaucoma awareness.[14,16,17] This constitutes one of the study limitations. However, it is well-known that highly-educated people are more likely to participate in health surveys and researches.[26-27] In addition, participants currently using eye drops and those with a positive family history of glaucoma and blindness were possibly more motivated to participate in the survey. This may also contribute to the high level of awareness and constitute another study limitation. As a result, our study sample may not be representative of the general black community in Toronto. Obtaining a random sample to generate population estimates is desirable but is a challenge issue faced by all studies, particularly when attempting to assess ethnic minorities.[28-30] To overcome potential issues related to the study sample, we surveyed 5 different black organizations to increase sample variations. Despite this effort, the sample is biased towards well-educated. This underscores the difficulties in obtaining a random sample in population-based research. On the other hand, our results from a well-educated sample revealed the level of glaucoma knowledge, such as peripheral visual field loss, was low, suggesting that our findings are conservative. Furthermore, since participants who were currently using eye drops and those who had a family history of glaucoma did not report improved glaucoma knowledge, we recommend these highly motivated participants should also be included in future educational endeavours, although financially disadvantaged individuals are clearly the most important group to target.
Strengths of this study include the fact that this is the first glaucoma awareness and knowledge study in a black community - a high-risk group for glaucoma. Secondly, our questionnaire focused specifically on glaucoma and its presentation, risk factors and methods of detection.
To prevent avoidable blindness, Noertjojo and associates called for a population-based approach to eye health education rather than a clinic-based approach.[13] They also recommended that innovative educational programmes for non-European-Canadian communities be created. We echo their views and recommend TV, newspapers, magazines, internet and flyers as the primary means of mass communication. Radio seems to be the least useful dissemination tool in Toronto, although in the UK, radio has been reported to be the most effective way to improve glaucoma awareness in an Indian community.[31]
Conclusions
The level of glaucoma awareness seems to be high amongst Toronto’s black community but knowledge regarding risk factors and the detection methods is low. Considering the high prevalence in the black community, education about glaucoma’s presentation, risk factors and detection methods should be prioritized as part of an educational campaign, especially amongst those less financially well-off.
Acknowledgements
The authors would like to thank the following 5 organizations for their support in distributing the questionnaire: Markham African Caribbean Association, Black Health Alliance, Jamaican Canadian Association, Rhema Christian Ministries, and Jambana festival. In particular we would like to thank Markham African Caribbean Association for conducting the pilot study which made the main study possible.
We also would like to thank Mr. Shudong Li for his help on data cleaning and analysis.
Financial support
This study was supported by the Glaucoma Research Society of Canada and the Dean's Fund, University of Toronto.
References
- Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, et al. (1991) Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA 266(3):369-74.
- Friedman DS, Jampel HD, Muñoz B, West SK (2006) The prevalence of open-angle glaucoma among blacks and whites 73 years and older: the Salisbury Eye Evaluation Glaucoma Study. Arch Ophthalmol 124(11):1625-30.
- Wilensky JT, Gandhi N, Pan T (1978) Racial influences in open-angle glaucoma. Ann Ophthalmol 10(10):1398-402.
- Hyman L, Wu SY, Connell AM, Schachat A, Nemesure B, et al. (2001) Prevalence and causes of visual impairment in The Barbados Eye Study. Ophthalmology 108(10):1751-6.
- Sit AJ, Chipman M, Trope GE. (2004) Blindness registrations and socioeconomic factors in Canada: an ecologic study. Ophthalmic Epidemiol 11(3):199-211.
- American Academy of Ophthalmology. (1996) Preferred practive pattern of primary open angle glaucoma. American Academy of Ophthalmology, San Fracisco.
- European Glaucoma Society. (1998) Terminology and guidlines for European Glaucoma Society. Dogma Srl, Savona, Italy.
- Quigley HA, Jampel HD (2003) How are glaucoma patients identified? J Glaucoma 12(6):451-5.
- Buys YM, Gaspo G, Kwok K (2012) Referral source, symptoms and disease severity at initial diagnosis of ocular hypertension or open-angle glaucoma in a mixture of specialized and comprehensive practices. Can J Ophthalmol 47:217-22.
- Buys YM, Harasymowycz P, Gaspo R, Kwok K, Hutnik CM, et al. (2012) Comparison of newly diagnosed ocular hypertension and open-angle glaucoma:ocular variables, risk factors, and disease severity. J Ophthalmol 2012:757106.
- Screening for Glaucoma: Recommendation Statement. U.S. Preventive Services Task Force. (2013) http://laico.org/v2020resource/files/screening_glaucoma.pdf
- Comparative Effectiveness of Screening for Glaucoma. American Academy of Ophthalmology and the American Glaucoma Society Joint Comments.(2013) http://www.aao.org/outofcs/wre/AAO-AGS_screening_comment.pdf
- Noertjojo K, Maberley D, Bassett K, Courtright P (2006) Awareness of eye diseases and risk factors: identifying needs for health education and promotion in Canada. Can J Ophthalmol 41(5):617-23.
- Livingston PM, McCarty CA, Taylor HR (1998) Knowledge, attitudes, and self care practices associated with age related eye disease in Australia. Br J Ophthalmol 82(7):780-5.
- Michielutte R, Diseker RA, Stafford CL, Carr P (1984) Knowledge of diabetes and glaucoma in a rural North Carolina community. J Community Health 9(4):269-84.
- Attebo K, Mitchell P, Cumming R, Smith W (1997) Knowledge and beliefs about common eye diseases. Aust N Z J Ophthalmol 25(4):283-7.
- Pfeiffer N, Krieglstein GK, Wellek S (2002) Knowledge about glaucoma in the unselected population: a German survey. J Glaucoma 11(5):458-63.
- Lau JT, Lee V, Fan D, Lau M, Michon J (2002) Knowledge about cataract, glaucoma, and age related macular degeneration in the Hong Kong Chinese population. Br J Ophthalmol 86(10):1080-4.
- Krishnaiah S, Kovai V, Srinivas M, Shamanna BR, Rao GN,et al. (2005) Awareness of glaucoma in the rural population of Southern India. Indian J Ophthalmol 53(3):205-8.
- Dandona R, Dandona L, John RK, McCarty CA, Rao GN (2001) Awareness of eye diseases in an urban population in southern India. Bull World Health Organ 79(2):96-102.
- Sathyamangalam RV, Paul PG, George R, Baskaran M, Hemamalini A, et al. (2009) Determinants of glaucoma awareness and knowledge in urban Chennai. Indian J Ophthalmol. 57(5):355-60.
- Zou G (2004) A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol 159(7):702-6.
- Barros AJ, Hirakata VN (2003) Alternatives for logistic regression in crosssectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 3:21.
- Eye-opening survey finds Canadians lack critical knowledge about glaucoma.(2013) Ahttp://www.canadafreepress.com/index.php/articles-health/9256.
- Census of Canada: individual public use microdata file. (2006) http://sda.chass.utoronto.ca/sdaweb/html/canpumf.htm.
- Anraku A, Jin YP, Butty Z, Jinapriya D, Alasbali T, et al. (2011) The Toronto epidemiology glaucoma survey: a pilot study. Can J Ophthalmol 46(4):352-7.
- Ontario health survey puts millions of people under the microscope. (2013) http://www.theglobeandmail.com/life/health-and-fitness/ontario-health-survey-puts-millions-of-people-under-the-microscope/article1214221/.
- Okazaki S, Sue S (1995) Methodlolgical issues in assessment research with ethnic minorities. Psychological Assessment 7(3):367-75.
- Vickers T, Craig G, Atkin K. (2012) Research with black and minority ethnic people using social care services. http://www.lse.ac.uk/lsehealthandsocialcare/pdf/sscr_methods_review_11_web.pdf
- Heim D, MacAskill S. ( 2013) Black and Minority Ethnic Health in Greater Glasgow: A Comparative Report on the Health and Well-Being of African & Caribbean, Chinese, Indian and Pakistani People and the General Population. http://library.nhsgg.org.uk/mediaAssets/library/nhsgg_report_bme_health_and_wellbeing_summary.pdf.
- Baker H, Murdoch IE. (2008) Can a public health intervention improve awareness and health-seeking behaviour for glaucoma?. Br J Ophthalmol 92(12):1671-5.





