Intravitreal Bevacizumab Followed by Ranibizumab for Neovascular Age Related Macular Degeneratıon
Yuksel N1*, Ozdek S2, Gurelık G2, Hasanreısoglu B2
1 Department of Ophthalmology, Ankara Ataturk Training and Research Hospital, Ankara, Turkey.
2 Department of Ophthalmology, Gazi University Medical Faculty, Ankara, Turkey.
*Corresponding Author
Nilay Yuksel,
Akpinar Mah. 858. Cad. Gunes Apt. No: 8/2,
Ankara, Turkey.
Tel: +90532-782 10 68; Fax: +90312-2213202
E-mail: ozturk.nilay@gmail.com
Article Type: Research Article
Received: June 13, 2014; Accepted: June 28, 2014; Published: June 30, 2014
Citation: Yuksel N, Ozdek S, Gurelık G, Hasanreısoglu B. (2014). Intravitreal Bevacizumab Followed by Ranibizumab for Neovascular Age Related Macular Degeneratıon, Int J Ophthalmol Eye Res, 2(3), 34-38.doi: dx.doi.org/10.19070/2332-290X-140007
Copyright: Yuksel N© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: To compare the outcomes after switching from intravitreal bevacizumab (IVB) to intravitreal ranibizumab (IVR) in patients
with neovascular age related macular degeneration (ARMD).
Material and Methods: A retrospective review of patients with neovascular ARMD, who were switched from treatment with Pro Re Nata (PRN) IVB to PRN IVR, was conducted in a university clinic. IVB (1.25 mg/0.05 ml) and IVR (0.5 mg/0.05 ml) were used. Retreatment criteria were defined based on an activity scoring (AS) system developed in our clinic. An AS was calculated for each lesion at each visit. AS results and the number of injections before and after switching treatment to IVR were compared.
Results: 32 eyes of 31 patients with neovascular ARMD were included in the study. The mean follow-up period was 12.3±4.7 months. The mean duration of IVB treatment was 8.1±3.1 months followed by 4.2±1.6 months with IVR. At the beginning of the study the mean AS was 8.9, (Visual Acuity) VA : 0.99 logMAR, and Central Foveal Thickness (CFT): 312.7±81.1μ. A month after the last IVB injection, AS became 5.1, VA: 0.69 logMAR, and CFT: 210.4±80.4μ (p<0.05). Likewise, a month after the last IVR injection, AS, VA and CFT were 5.8, 0.78 logMAR, and 199.9±60.9μ, respectively. Comparison of post-injection results of IVB and IVR treatments did not reveal a statistically significant difference. Mean injection rates per patient while receiving IVB and IVR treatments were 0.46/month and 0.44/month, respectively (p>0.05).
Conclusions: This study shows that the improvement in AS, CFT, and VA, achieved with the PRN IVB treatment, seems to be maintained
after switching to IVR.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Acknowledgements
7.References
Keywords
Activity Scoring; Age Related Macular Degeneration; Bevacizumab; Ranibizumab.
Introduction
Presently, two vascular endothelial growth factor (VEGF) inhibitors are widely used for the treatment of neovascular agerelated macular degeneration (ARMD): bevacizumab (Avastin; Genentech, South San Francisco, CA) and ranibizumab (Lucentis; Genentech, South San Francisco, CA). Both bevacizumab and ranibizumab are derived from the same murine monoclonal antibody against VEGF-A and bind to the same site of VEGFA, thereby neautralizing all known biologically active forms of VEGF.[1,2]
Bevacizumab is a recombinant humanized monoclonal antibody that was the first anti-VEGF drug to be approved in 2004 by the Food and Drug Administration (FDA) for the intravenous treatment of metastatic colorectal cancer.[1] A study in which bevacizumab was used intravenously for the treatment of neovascular ARMD reported promising optical coherence tomography (OCT) and visual acuity results.[3] The first report of intravitreal bevacizumab (IVB) administration for neovascular ARMD was published in 2005.[4] Encouraging results for its efficacy and safety, and its low cost and worldwide availability made it a popular choice for the treatment of many ocular disorders, including neovascular ARMD.
Ranibizumab is a recombinant humanized antibody fragment that binds and inhibits the action of VEGF-A. Ranibizumab was approved for the treatment of neovascular ARMD by the FDA in 2006 after Phase III randomized and controlled clinical trials, known as MARINA and ANCHOR, proved its safety and efficacy.[5,6]
Once ranibizumab became an on-label drug, many medicare patients who were undergoing treament with bevacizumab were switched to ranibizumab. In this study, the outcomes of patients transitioned from bevacizumab to ranibizumab for the treatment of neovascular ARMD were evaluated.
Materials and Methods
The study followed the tenets of the Declaration of Helsinki and had the approval of the Institutional Research Board. Written informed consent was obtained from each participant.
The medical records of patients with neovascular ARMD, who first underwent treatment with Pro Re Nata (PRN) IVB and later with PRN IVR, were reviewed retrospectively from May 2006 to June 2009 at the Ophthalmology Department of the Medical Faculty of Gazi University.
At the beginning of the study, a month after the last IVB treatment, and a month after the transition to IVR treatment, bestcorrected visual acuity (BCVA, logMAR), applanation tonometry, slit-lamp evaluation, dilated biomicroscopic fundus examination, fundus fluorescein angiography (FFA), and central foveal thickness (CFT) measurement using optical coherence tomography (OCT, Humphrey model 3000 (Zeiss-Humphrey Instruments,San Leandro, CA)) were performed.
Re-treatment criteria were defined based on an activity scoring system, including 5 parameters (Table 1), which was developed at our clinic.
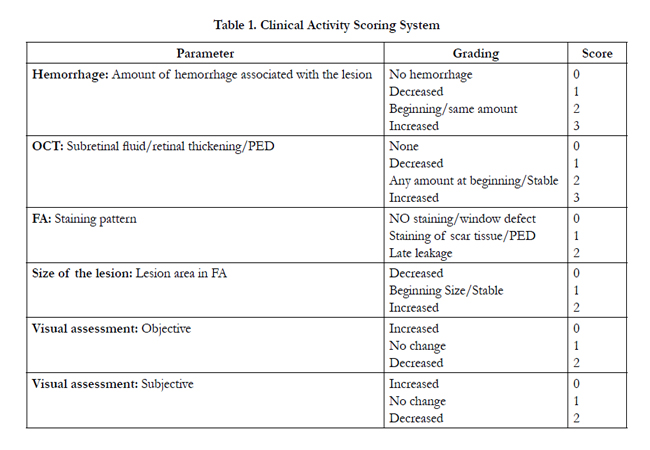

Table 1. Clinical Activity Scoring System
1. OCT: After pupil dilatation, six consecutive 6-mm-long scans containing 128 axial profiles (A-scans) at equally spaced angular orientations in a radial spoke pattern centered on the fovea (known as Fast Macular Thickness Protocol) were obtained for each eye. Using Retinal Thickness Mapping Software, the mean retinal thickness value, which was measured in the central disc with a diameter of 1000μm in the center of the macula, was used as central foveal thickness (CFT).The fluid pattern (subretinal / intraretinal diffuse / cystoid /pigment epithelial detachment - PED) was also noted. Only CFT was used as an activity parameter in AS, and a change in this by at least 10% in the negative or positive direction was considered a significant decrease or increase. The amount of fluid at the beginning was scored as “2”. It was scored as “0” if there had been no fluid, “1” if there had been a decrease, and “3” if there had been an increase (in CFT).
2. Amount of hemorrhage: The amount of hemorrhage associated with the lesion (in ophthalmoscopy, colored fundus photography or FA) was noted, and if there had been any at the beginning, it was scored as “2”. If there had been no hemorrhage it was scored as “0”. If hemorrhage had decreased it was scored as “1”, if it had remained the same it was scored as “2”, and if it had increased it was scored as “3”.
3. FA staining pattern: No staining or window defect (0), staining of scar tissue or PED (1) and late leakage (2) were noted.
4. The area of the lesion (mm2): This was measured in FA and the baseline area (or no change) was scored as “1”, an increase by at least 10% (of the original area) as “2” and a decrease by at least 10% as “0”.
5. Visual assessment: Objective visual acuity was measured and noted as a baseline and scored as “1”. If there had been a decrease in vision (any line loss) it was scored as “2”, and any increase in vision (any line gain) scored as “0”. The patient was also enquired regarding how he felt about any change in his vision, noted as subjective vision, which was scored as “0” if he felt better, “2” if he felt worse, and “1” if he did not feel any change (baseline).
At the end of the assessment, the numbers obtained were summed and an activity score was calculated for each lesion at each visit. AS results and the number of injections before and after switching the treatment to IVR were compared.
All intravitreal injections were made using a standard protocol and established guidelines. Following topical anesthesia with proparacaine, the eyelids and eyelashes were scrubbed with povidone- iodine (10%). After placement of the sterile lid speculum, povidone-iodine (5%) drops were applied over the ocular surface. Using a sterile 1-ml tuberculin syringe with a 30-gauge needle, either 1.25 mg/0.05 ml bevacizumab or 0.5 mg/0.05 ml ranibizumab was injected into the vitreous cavity through the pars plana, approximately 3-4 mm posterior to the superotemporal limbus. A topical fluoroquinolone antibiotic was used thrice a day for five days after the injection.
Power analysis was performed to justify the number of patients enrolled in the study. Data were statistically analyzed using SPSS 16.0 software. The Paired Samples t-test was used to compare IVB and IVR treatments. Statistical significance was defined as p<0.05.
Results
32 eyes of 31 patients (12 women and 19 men) with neovascular ARMD were included in the study. The mean age of the patients was 73.2 ± 10.2. The mean follow-up period was 12.3 ± 4.7 months, and the mean duration of IVB treatment 8.1 ± 3.1 months, followed by 4.2 ± 1.6 months of IVR treatment.
At the beginning of the study, the mean AS was 8.9, VA: 0.99 logMAR, and CFT: 312.7 ± 81.1. A month after the last IVB injection, AS became 5.1 (p = 0.031), VA: 0.69 logMAR (p = 0.029), and CFT: 210.4 ± 80.4μ (p = 0.028). A month after the last IVR injection, AS was 5.8, VA was 0.78 logMAR, and CFT was 199.92 ± 60.9μ. (Figure 1-2-3)
Comparison of post-injection results of IVB and IVR treatments did not reveal any statistically significant difference. Mean injection rates per patient while receiving IVB and IVR treatments were 0.46/month and 0.44/month, respectively (p=0.098).
AS, VA and CFT results were compared after IVB and IVR treatments and no statistically significant differences were determined (p = 0.135, p = 0.097, and p = 0.118, respectively).
No major ocular side-effects, such as endophthalmitis or retinal detachment, were noted. In addition, there were no cases of adverse systemic events, such as myocardial or cerebral infarction, or treatment-emerged hypertension; and no patient died during the follow-up period.
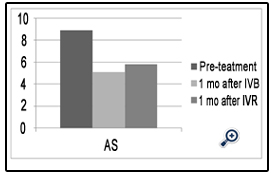
Figure 1. Changes in VA over the treatment period.
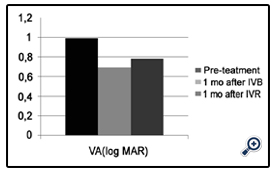
Figure 2. Changes in CFT over the treatment period.
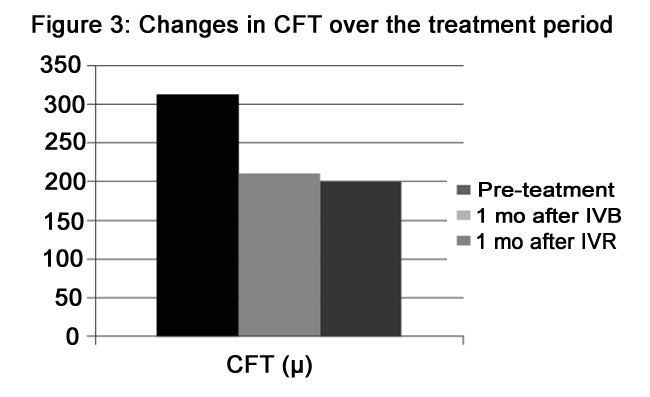
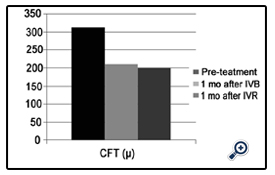
Figure 3. Changes in CFT over the treatment period.
Discussion
Currently, many clinicians are puzzled by the scientific challenges and economic problems associated with these drugs. Numerous retrospective and prospective studies continue to question the outcomes of eye treatments using IVB and IVR.
Both ranibizumab and bevacizumab bind VEGF at the same position; however, they differ in their size, affinity for VEGF, speed of clearance from the eye, and cost.[7]
One of the pharmaceutical industry-independent head-to-head randomized controlled studies, A Comparison of AMD Treatment Trials: Ranibizumab-Bevacizumab Trial (CATT), reported results for a year in May 2011 and for two years in July 2012.[8,9] At the end of one and two years bevacizumab and ranibizumab were found to have had similar effects on visual acuity, with the dosing regimen being the same. Both drugs reduced retinal and subretinal fluid effectively. The CATT results support the continued and widespread use of IVB as an effective, low-cost alternative to IVR.
A similar study entitled A Randomized Controlled Trial of Alternative Treatments to Inhibit VEGF in Age-Related Choroidal Neovascularization (IVAN) reported results for a year in July 2012 and concluded that both drugs had equivalent effects on visual function.[10] Ranibizumab, and monthly treatment, resulted in significantly better morphologic outcomes.
The first study on treatment switching evaluated patients who had at least three IVB treatments before switching to IVR treatment, and concluded that there were no apparent differences in visual acuity outcomes or injection rates.[1] The investigators of the study found the average injection rate for the two drugs to be 0.66/month. In our study, mean injection rates per patient while receiving IVB and IVR treatments were 0.46/month and 0.44/ month, respectively; and this difference was also not statistically significant.
Another study similar to ours compared patients who had been treated three times or more with IVB every 6 weeks initially, and then as needed before being switched to IVR every 4 weeks until they were clinically stable; the IVR treatment was continued on an "as needed” basis.[11] The results revealed significant improvements in VA and CFT in patients who had been initially treated with IVB. Besides, a further significant improvement in VA and reduction in CFT were seen in these patients after they had been switched to IVR. Both the studies are similar in respect of absence of i) patient or physician preference, ii) lack of response to one of the medications and iii) Inability on the part of patients to pay. This allowed for patients to be used as their own controls, avoiding physician selection bias.
Another treatment switching study showed that switching from bevacizumab to ranibizumab results in a transient decrease of visual acuity and an increase of retinal thickness, causing a transient “instability” in the eye.[12] The final visual acuity and retinal thickness after IVR were better than those after IVB in their study.
A major difference between our study and those of Kent et al and Karagiannis et al, is in the treatment frequency. The former started with a monthly treatment regimen and then switched to an “as-needed regimen”, while the latter compared only monthly regimens. We compared PRNs protocol for IVB and IVR treatments.
There are reports in the scientific literature that provide no evidence of either of these drugs being superior to the other. In all these reports,separate patient groups, treated only with IVB or IVR, were compared.
Landa et al, Gamulescu et al and Fong et al reported that there is no significant difference in the efficacies of IVB and IVR.[13-15] Subramanian et al reported outcomes for a year for a prospective study that failed to show any difference in visual and anatomic results between the two treatments. But, patients in the IVB group received a statistically significant greater number of injections than those in the IVR group.[16] These investigators suggested that a possible reason for this may have been a tachyphylactic response due to different treatment doses for the two drugs. But, according to Schmucker et al, the bevacizumab molecule is about three times as large as ranibizumab and may remain in the eye longer, allowing for less frequent injections.[17]
Biswas et al compared IVB with IVR head-to-head as two groups. [18] The changes in the means of BCVA and CFT were compared and they concluded that IVB and IVR are equally safe and effective when administered monthly as injections thrice and then as needed. The mean number of injections required in their study in the IVB group (4.3) was less than the number required in the IVR group (5.6).
On the other hand, Chang et al reported a significantly better short-term effectiveness with IVR than IVB as measured by OCT. [19] We suggest that the present study is unique as it allows for comparisons to be made between two different drugs on the basis of responses elicited by them from the same patient. Besides, retreatment decisions were based on objective criteria, supportedby a clinical activity scoring system. In many studies, the chief criteria on which decisions to treat or re-treat ARMD are based are fluorescein leakage, the angiographic appearance of the lesion and OCT. However, the concordance between OCT and FA is not always a reliable indicator [20], and other parameters may have to be considered to decide on the need for re-treatment. Some of these parameters may be i) presence of subretinal hemorrhage associated with the lesion, ii) change in the size of the lesion and iii) visual acuity. Most clinicians rely on their experience and intuition to decide on new treatments using some of these parameters. AS is particularly desirable in standardizing re-treatment protocols as it is important not to over-treat eyes in order to avoid injectionand drug-related complications as well as the high costs of the treatment.
The main limitations of this study are its retrospective nature and a relatively small sample size; therefore, to provide a clear and reliable answer to the question of whether bevacizumab or ranibizumab is the better drug, prospective and randomized trials are needed. In addition, AS may be modified by the use of other tools like central field acuity perimetry for visual assesment to be more objective.
In conclusion, this study shows that improvements in AS, CFT, and VA, achieved with the PRN IVB treatment, seems to be maintained after switching to IVR. Further, it also reveals that there is no significant difference in injection rates between the treatments.
Acknowledgements
None of the authors has conflict of interest with the submission. No financial support was received for this submission.
References
- Stepien KE, Rosenfeld PJ, Puliafito CA. (2009) Comparison of intravitreal bevacizumab followed by ranibizumab for the treatment of neovascular agerelated macular degeneration. Retina 29:1067-73.
- Steinbrook R. (2006) The price of sight-ranibizumab, bevacizumab, and the treatment of macular degeneration. N Engl J Med 355:1409-12.
- Moshfeghi AA, Rosenfeld PJ, Puliafito CA. (2006) Systemic bevacizumab (Avastin) therapy for neovascular age-related macular degeneration: twentyfour- week results of an uncontrolled open-label clinical study. Ophthalmology 113(11):2002.e1-e12.
- Rosenfeld PJ, Moshfeghi AA, Puliafito CA. (2005) Optical coherence tomography findings after an intravitreal injection of bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging 36:331-5.
- Brown DM, Kaiser PK, Michels M. ANCHOR Study Group. (2006) Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 355:1432-44.
- Kaiser PK, Brown DM, Zhang K. (2007) Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol 144:850-7.
- Stewart MW. (2007) Predicted biologic activity of intravitreal bevacizumab. Retina 27:1196-1200.
- Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, et al. (2011) Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med 364:1897-908
- Martin DF, Maguire MG, Fine SL. (2012) Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results.Ophthalmology. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group 119:1388-98.
- Chakravarthy U, Harding SP, Rogers C. (2012) Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: one-year findings from the IVAN randomized trial. Ophthalmology. IVAN Study Investigators 119:1399-411
- Kent JS, Iordanous Y, Mao A, Powell AM, Kent SS,et al. (2012) Comparison of outcomes after switching treatment from intravitreal bevacizumab to ranibizumab in neovascular age-related macular degeneration. Can J Ophthalmol 47:159-64.
- Karagiannis DA, Ladas ID, Parikakis E. (2009) Changing from bevacizumab to ranibizumab in age-related macular degeneration. Is it safe? Clin Interv Aging 4:457-61.
- Landa G, Amde W, Doshi V. (2009) Comparative Study of Intravitreal Bevacizumab (Avastin) versus Ranibizumab (Lucentis) in the Treatment of Neovascular Age-Related Macular Degeneration. Ophthalmologica 223:370-5.
- Gamulescu MA, Radeck V, Lustinger B, Fink B, Helbig H. (2010) Bevacizumab versus ranibizumab in the treatment of exudative age-related macular degeneration. Int Ophthalmol 30:261-6.
- Fong DS, Custis P, Howes J, Hsu JW. (2010) Intravitreal bevacizumab and ranibizumab for age-related macular degeneration a multicenter, retrospective study. Ophthalmology 117:298-302.
- Subramanian ML, Abedi G, Ness S. (2010) Bevacizumab vs ranibizumab for age-related macular degeneration: 1-year outcomes of a prospective, doublemasked randomised clinical trial. Eye (Lond) 24:1708-15.
- Schmucker C, Ehlken C, Hansen LL, Antes G, Agostini HT,et al. (2010) Intravitreal bevacizumab (Avastin) vs. ranibizumab (Lucentis) for the treatment of age-related macular degeneration: a systematic review. Curr Opin Ophthalmol 21:218-26.
- Biswas P, Sengupta S, Choudhary R, Home S, Paul A,et al. (2011) Comparative role of intravitreal ranibizumab versus bevacizumab in choroidal neovascular membrane in age-related macular degeneration. Indian J Ophthalmol 59:191-6.
- Chang TS, Kokame G, Casey R, Prenner J, Feiner L,et al. (2009) Short-term effectiveness of intravitreal bevacizumab versus ranibizumab injections for patients with neovascular age-related macular degeneration. Retina 29:1235- 41.
- Krebs I, Ansari-Shahrezaei S, Goll A, Binder S. (2008) Activity of neovascular lesions treated with bevacizumab: comparison between optical coherence tomography and fluorescein angiography. Graefes Arch Clin Exp Ophthalmol 246:811-5.





