Sub-Tenon Versus Peribulbar Anesthesia In Phacoemulsification A Comparitive Study
Shahid E1*, Afaq A2, Juzar UT3, Ansari Z4, Sharif Ul Hasan K5
1* Senior Registrar Ophthalmology, Abbassi Shaheed Hospital, Karachi, Pakistan.
2 Associate Professor Ophthalmology, Baqai Medical University, Karachi, Pakistan.
3 Senior Registrar Ophthalmology, Baqai Medical University, Karachi, Pakistan.
4 Associate Professor Ophthalmology, Baqai Medical University, Karachi, Pakistan.
5 Professor Emeritus & Chairman, Department Of Ophthalmology, Baqai Medical University, Karachi, Pakistan.
*Corresponding Author
Dr. Erum Shahid,
Senior Registrar Ophthalmology,
Abbassi Shaheed Hospital,
Karachi, Pakistan.
Tel: 0321-2958058
E-mail: drerum007@yahoo.com
Article Type: Research Article
Received: July 06, 2013; Accepted: August 16, 2013; Published: September 03, 2013
Citation: Shahid E, et al. (2013). Sub-Tenon Versus Peribulbar Anesthesia in Phacoemulsification a Comparative Study, Int J Ophthalmol Eye Res, 01(01), 09-13.doi: dx.doi.org/10.19070/2332-290X-130002
Copyright: Shahid E© 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: The purpose is to compare the effectiveness of Sub-Tenon’s anaesthesia versus Peribulbar anaesthesia for intraoperative analgesia and ocular akinesia during phacoemulsification surgery.
Material And Method: This analytic study consisted of 100 patients with simple random sampling, 50 patients in each group. Patients in group A had phacoemulsification under subtenon anaesthesia and patients in group B had the same surgery under peribulbar anaesthesia. Their eye movements and pain during surgery were documented and analyzed .Pearson Chi square test was used to determine the statistical significance.
Results: In the group A (Subtenon group) there are 35 (70%) males and in group B (peribulbar group) there were 26 (52%) males. The age range of the patients was between 50-70 years.
Pain during surgery in group A is 3 (24%) whereas in group B it is 28 (56%).Eye movements during the procedure of subtenon anesthesia in group A is 13 (26%) whereas eye movements during peribulbar anesthesia in group B is 22 (44%).Chi-square test is used between the eye movements and pain of group A and group B. There p values are less than 0.005 which are significant.
Conclusion: Sub-Tenon anaesthesia gains our full recommendation for prospective benefits and elimination of potential fatal hazards like globe perforation, retrobulbar hemorrhage, sub arachnoid injection, imposed by using sharp needle blocks. It calms patient’s fear of sharp needles which raises the anxiety levels even prior to surgery. This technique also provides almost immediate progressive surgery.
2.Materials and Methods
3.Results
4.Discussion
5.Conclusion
6.References
Introduction
The commonest ophthalmic surgical procedure being performed worldwide is cataract surgery and preferred anaesthetic technique for it is under local anaesthesia. The provision of ophthalmic regional anaesthesia for cataract surgery varies globally. These may be chosen not to eliminate eye movements. Akinetic and non-akinetic methods, both are widely used. Beside this, patient’s comfort, safety and low complication rates are essentials for local anaesthesia [1].
Retro bulbar anaesthesia was the anaesthesia of choice for extracapsular cataract extraction as well as for phacoemulsification for decades [2]. This was associated with rare but real complications such as globe perforation, brain stem anaesthesia, postoperative strabismus, hemorrhage and optic nerve injury. This has led to get this procedure replaced with peribulbar anaesthesia [2].
Topical and subconjunctival anaesthesia are also used which are apparently less traumatic, relatively safe and effective techniques. However they do not provide adequate akinesia and these techniques can only be safely performed on selected co-operative patients. Recent reports amongst ophthalmic surgeons suggest that the use of Sub-Tenon’s block has become common. It has been suggested that it has a more acceptable risk profile than traditional ophthalmic anesthesia techniques [3].
The advent of small, stepped, and self-sealing corneal incisions leads to very little manipulation and this allowed the use of Sub-Tenon’s anaesthesia and topical anesthesia [4].
The purpose of this study was to compare the effectiveness of Sub-Tenon’s anaesthesia versus Peribulbar anaesthesia for intraoperative analgesia and ocular akinesia during phacoemulsification surgery of cataract.
Materials and Methods
The study was conducted at the department of Ophthalmology, Baqai Medical University, Karachi. It was a prospective analytic study. The duration of the study was two years from March 2009 to June 2011.
A total number of 100 patients with simple random sampling were enrolled in the study. 50 patients were randomly assigned to subtenon’s anesthesia (Group A) and 50 patients to the peribulbar anesthesia (Group B).All the cases underwent phacoemulsification with nonfoldable posterior chamber intraocular lens implantation through a 5.5 mm limbal incision, by the same surgeon.
All the patients with uncomplicated senile cataracts, over the age of 50 years, with either gender were included in the study. Patients with secondary cataracts, congenital cataracts, previous history of retinal detachment surgery, strabismus surgery, ocular trauma, orbital infections and not willing to be a part of the study were excluded from the study.
No additional oral sedation or analgesia was used in any of the cases. Written informed consent was obtained from the patients. All the local anaesthetic injections were given by the same surgeon.
After standard aseptic preparation, subtenon anaesthesia was performed by instilling a few drops of proparacaine 1% in the conjunctival sac. An eyelid speculum was inserted at this point to improve access. The patient was asked to look upward and outward to expose the infero-nasal quadrant. A small tent of conjunctiva was raised with a pair of fine non-toothed forceps (Moorfields) approximately 5-10 mm from the limbus. A small incision was made in the tented conjunctiva with blunt Westcott (spring) scissors, the closed scissors were introduced through the aperture created and a tunnel was fashioned to the bare sclera by blunt dissection through Tenon’s capsule. A curved blunt cannula of 23 gauge was then inserted with the syringe of the anaesthetic solution attached and guided along the contour of the globe. The cannula was advanced posterior to the equator of the globe and 1.5 ml of the anaesthetic solution was infiltrated. The anaesthetic solution diffuses backward to the intraconal space leading to the paralysis of long and short posterior ciliary nerves. It also blocks the ciliary ganglion.
Normally little resistance is found to injection. If resistance is felt, withdrawal and re-insertion of the cannula using gentle pressure of the tip against the globe to ensure entry into the correct tissue plane will help. Slight proptosis of the eyeball is normal after a correctly sited injection. There may be slight leakage of the solution from the tunneled point of entry of the cannula into the conjunctiva. Should ballooning of the conjunctiva occur, the solution might be in the incorrect tissue plane.
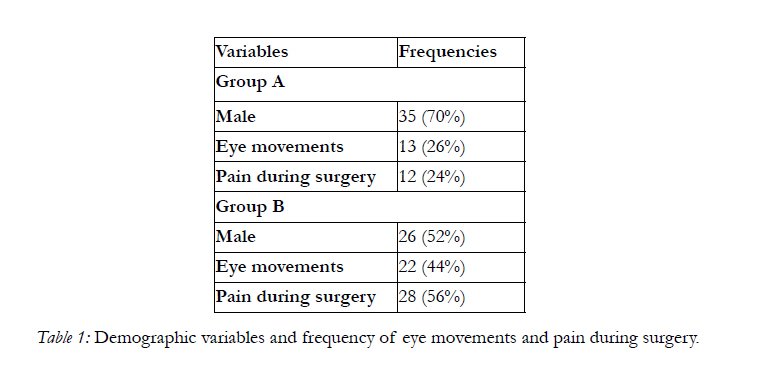

Table 1: Demographic variables and frequency of eye movements and pain during surgery.
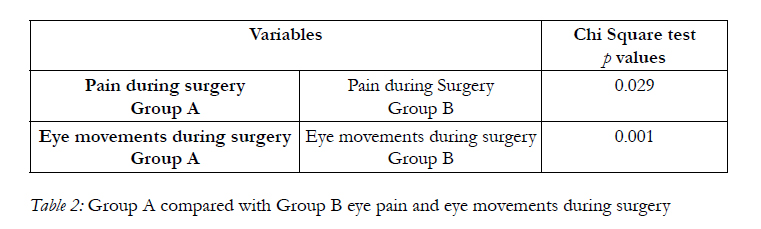
Table 2: Group A compared with Group B eye pain and eye movements during surgery.
Peribulbar anesthesia was performed after all aseptic measures, using a sharp needle (3/4 inch long). The needle was introduced in the lateral 1/3 of the orbit inferiorly just above the orbital rim. A total of 3 ml of the anesthetic solution was infiltrated.
Both techniques were evaluated in terms of ocular movements during surgery and patient’s pain perception during the surgical procedure. These measures were assessed by an observer. The observer filled a chart: no movement and movement. Postoperative pain chart was devised to assess patient’s pain perception during the surgical procedure. Patients were interviewed in the recovery soon after completing the surgical procedure. Pain was graded as: pain and no pain. Data was entered and analyzed on SPSS version 21.Each anaesthesia technique was tabulated with pain and eye movement. Chi square test was used to determine the statistical significance.
Results
Our study included 100 patients, 50 patients received subtenon and 50 patients received peribulbar local anaesthesia for phacoemulsification surgery respectively. In the group A (Subtenon group) there are 35 (70%) males and 15 (30%) females. In the group B (Peribulbar group) there were 26 (52%) males and 24 (48%) females (Table 1). The age range of the patients was between 50-70 years.
Pain during surgery in group A is 12 (24%) whereas in group B it is 28 (56%) shown in table 1.Eye movements during the procedure of subtenon anaesthesia in group A is 13 (26%) whereas eye movements during peribulbar anaesthesia in group B is 22 (44%). Chisquare test is used between the eye movements and pain of group A and group B. There p values are less than 0.005 which are considered to be significant.
Discussion
Cataract removal has become faster, safer, and less traumatic. The need for akinesia and anesthesia has significantly declined. A wide variety of anaesthesia options are available for cataract surgery [5].
The retrobulbar and peribulbar blocks can be hazardous as the anaesthetic solution is blindly infiltrated into the orbit through a sharp needle. Globe perforation, retrobulbar haemorrhage, optic nerve damage and injection of the anaesthetic solution into the subarachnoid space all have been reported. The peribulbar block is relatively safe but serious complications have also been reported [2, 6, 7].The Subconjunctival anaesthesia is an effective and safer alternative; however, this technique provides no akinesia [8]. Topical anaesthesia has gained wide popularity particularly with the advent of phacoemulsification [9]. However it does not provide akinesia. Complete lack of akinesia can pose significant difficulty when dealing with uncooperative patients or the delay in surgical time due to intraoperative complications.
The technique of Sub tenon’s anaesthesia was first described by Turnbull in 1884 [10]. Ripart and colleagues have popularized this block [11].In our study we used the inferio-nasal quadrant for access to the sub tenon’s space. Access to all other quadrants have been reported and are essentially similar in principle, such as superotemporal by Fukasaku and Marron [12]. We used the infero-nasal quadrant because of the ease of access to this quadrant.
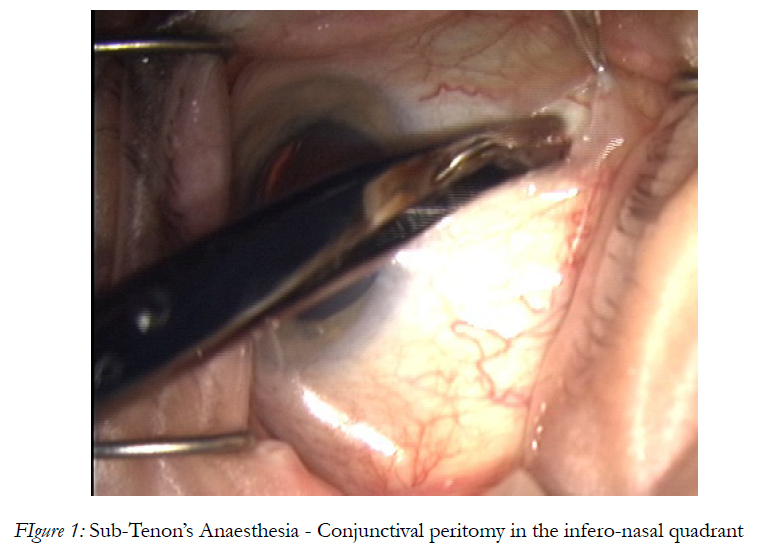
Figure 1: Sub-Tenon’s Anaesthesia - Conjunctival peritomy in the infero-nasal quadrant
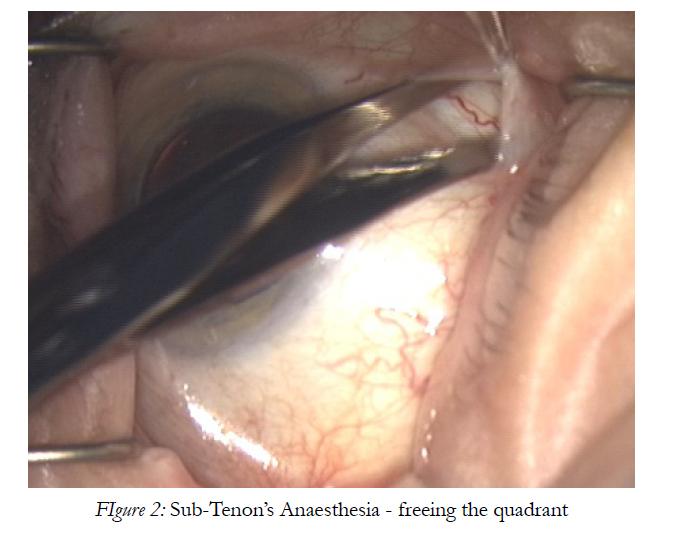
Figure 2: Sub-Tenon’s Anaesthesia - freeing the quadrant.
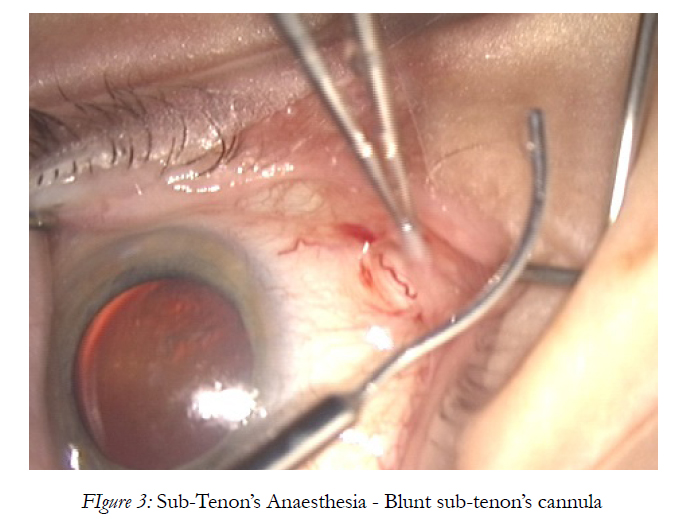
Figure 3: Sub-Tenon’s Anaesthesia - Blunt sub-tenon’s cannula
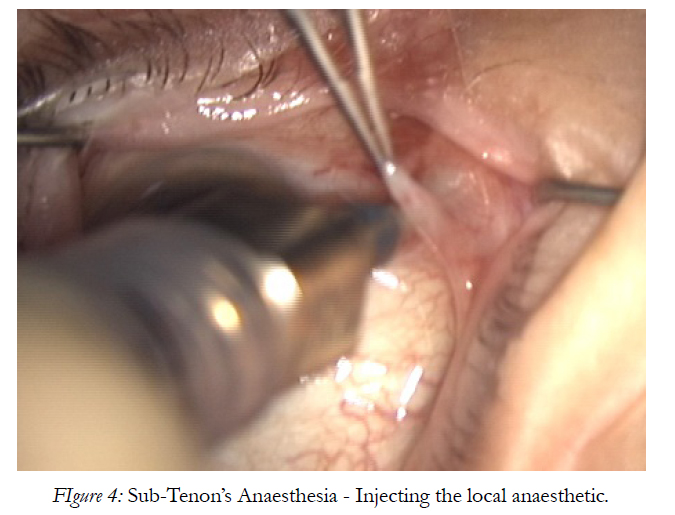
Figure 4: Sub-Tenon’s Anaesthesia - Injecting the local anaesthetic.
Different cannulaes are available for the sub-tenon’s block. The specially designed cannulae are made of either metal or plastic. The metal cannulae vary in gauge, length, curvature and position of the end holes. A plastic intra venous cannula can also be used [13]. We employed the readily available metallic cannula.
Passage of local anaesthetic agent during sub-tenon’s injection has been studied using ultrasound [14] and magnetic resonance imaging techniques [15]. The injection of anaesthetic agent into the sub-tenon’s space opens the space circumferentially giving a characteristic “T-sign”. It diffuses into intraconal and extraconal spaces, resulting in anaesthesia and akinesia of the globe and eyelids [14, 15].
The aim of local anaesthesia is essential to achieve as low a level of discomfort during surgery as possible. Administration of the local anaesthetic will inevitably be associated with some discomfort. Premedication or sedation of patients does not add any benefit however preoperative explanation of the procedure, good surface anaesthesia, gentle technique and re assurance are considered good practice and may reduce the discomfort and anxiety during the operation [16].
Many studies have compared subtenon with peribulbar anaesthesia including Ripart j [17], Budd JM [18], Parkar T [19] , Briggs MC [20] and Ashok kumar ophthalmology international update [21] .All these studies have demonstrated Sub-Tenon’s anesthesia to be more effective as compared to the peribulbar block in terms of both ocular akinesia and analgesia.
In our study, 24% of patients in group A had pain, as compared to 56% patients in group B. The results of our study are similar to the above mentioned studies regarding the effect on pain.The effectiveness of subtenon anaesthesia regarding akinesia was also found to be superior in our study. The results are comparable to the above studies.
The volume of the anaesthetic solution for the subtenon block varies widely. It can range between 1-11 ml [22] but 3-5 ml is generally used [23] .Larger volumes are required for deep akinesia [24] .We used only 1.5 ml of the anaesthetic solution. The rationale behind using less volume of anaesthetic solution was that deep akinesia is not an absolute pre-requisite for phacoemulsification surgery and it does not cause intra- operative difficulties [25] .Globe can be stabilized with the phacoemulsification probe and also by the second instrument through the other port. We were absolutely comfortable with the presence of moderate ocular movements during the procedure. If these movements are undesirable, anaesthesia or akinesia can be supplemented by injecting more solution.
Sub conjunctival hemorrhages and conjunctival ballooning (chemosis) are common after subtenon block. These do not impede the procedure. Hemorrhages can be controlled by cauterizing the peritomy site at the start of the block and chemosis decreases as the experience of the surgeon increases with this technique [23, 26].
Conclusion
Sub-Tenon anaesthesia gains our full recommendation for prospective benefits and elimination of potential fatal hazards like globe perforation, retrobulbar hemorrhage, sub arachnoid injection of the anaesthetic solution, imposed by using sharp needle blocks. It calms patient’s fear of sharp needles which raises the anxiety levels even prior to surgery. This technique also provides almost immediate progressive surgery.
References
- Leaming DV. Practice styles and preferences of ASCRS members—2003 survey. J Cataract Refract Surg 2004;30:892-900.
- Davis DB, Mandel MR. Efficacy and complication rate of peribulbar blocks; A prospective multicenter study. J Cataract Refract Surg 1994;20;327-37.
- Dark A. Local anaesthesia for routine ocular surgery. Br J Anaesthesia 1999; 82: 153-4
- Crandall AS (2001) Anesthesia modalities for cataract surgery. Curr Opin Ophthalmol 12: 9-11.
- Manners TD, Burton RL. Randomised trial of topical versus sub- Tenon’s local anaesthesia for small-incision cataract surgery. Eye 1996; 10: 367-70.
- Hay A, Flynn H, Hoffman J. Needle penetration of the globe during retrobulbar and peribulbar injections. Ophthalmol 1991;98;1017-24
- Mount AM, Seward HC. Scleral perforation during peribulbar anaesthesia. Eye 1993;7;766-7.
- Redmond RM, Dallas NL. Extracapsular cataract extraction under local anaesthesia without retrobulbar anaesthesia. Br J Ophthalmol 1990;74:203-4
- Werthein M, Burton R. Immediately sequential phacoemulsification performed under topical anaesthesia as day case procedures. Br J Ophthalmol 2002;86:1356-8.
- Turnbull CS. The hydrochlorate of cocaine, a judicious opinion of its merits. Med Surg Rep 1884;29:628-29.
- Ripart J. Medial canthus single injection episclera l(subtenon anaesthesia): computed tomography imaging. Anaesth Analg 1998;87:42- 45.
- Fukasaku H, Marron JA. Sub-Tenon’s pinpoint anaesthesia. J Cataract Refract Surg 1994;20:468-471.
- Kumar CM, Dodds C. A disposable plastic sub-Tenon cannula. Anaesthesia 2001; 56:399-400.
- Winder S, Walker SB, Atta HR. Ultrasonic localization of anaesthetic fluid in sub-Tenon’s, peribulbar and retrobulbar techniques. J Cataract Refract Surg 1999; 25:56-59.
- Niemi-Murola L, Krootila K, Kivisaari R, et al. Localization of local anaesthesia solution by magnetic resonance imaging. Ophthalmology 2004; 111 :342-347.
- Guise PA. Sub-Tenon anesthesia; a prospective study of 6000 blocks. Anaesthsiology 2003; 98: 964-968
- Ripart J, Lefrant JY, Vivien B .Ophthalmic regional anaesthesia. Anaesthisiology 2000; 92: 1278-85.
- Budd JM, Brown JP, Thomas J, et al. A comparison of sub-Tenon’s with peribulbar anaesthesia in patients undergoing sequential bilateral cataract surgery. Anaesthesia 2009; 64: 19-22.
- Parker T, Gogate P, Deshpande M, et al. Comparison of sub-Tenon anaesthesia with peribulbar anaesthesia for manual small incision cataract surgery. Indian J Ophthalmol 2005; 53: 255-9.
- Briggs MC, Beck SA, Esakowite L. Subtenon’s vs peribulbar anaesthesia for cataract surgery. Eye 1997; 11: 639-43.
- Ashok Kumar P, Anwar Ali, Jehanzeb Durrani. Sub-Tenon’s vs peribulbar anaesthesia; Ophthalmology update 2010; .8: 19-23.
- Greenbaum S. Parabulbar anaesthesia. Am J Ophthalmol 1992; 114: 776.
- Roman SJ, Chong Sit DA, Boureau CM et al. Sub-Tenon’s anaesthesia: an efficient and safe technique. Br J Ophthalmol 1997; 81: 673-676.
- Tokuda Y, Oshika T, Amano S et al. Anaesthetic dose and analgesic effects of Sub-tenon’s anaesthesia. J Cataract Refract Surg 1999; 25:1250-1253.
- Tsuneoka H, Ohiki K, Taniuchi K. Tenon’s capsule anaesthesia for cataract surgery with IOL implantation. Eue J implant Ref Surg 1993; 5: 29-34.
- Kumar CM, Dodds C. Evaluation of Greenbaum sub-Tenon’s block. Br J Anaesth 2001; 87: 631–633.





