Medical Rehabilitation in Natural Disasters in the Asia-Pacific Region: The Way Forward
Khan F1,2,3,4*, Amatya B1,4, Rathore FA4,5, Galea MP1,2,4
1 Department of Rehabilitation Medicine, Royal Melbourne Hospital, Parkville, Victoria, Australia.
2 Department of Medicine (Royal Melbourne Hospital), The University of Melbourne, Parkville, Victoria, Australia.
3 School of Public Health and Preventive Medicine, Monash University, Victoria, Australia.
4 Committee for Rehabilitation Disaster Relief (CRDR), International Society of Physical and Rehabilitation Medicine (ISPRM), Geneva, Switzerland.
5 Department of Rehabilitation Medicine, CMH Lahore Medical College, University of Health Sciences, Lahore, Pakistan.
*Corresponding Author
Fary Khan
Department of Rehabilitation Medicine,
Royal Melbourne Hospital, 34-54 Poplar Road Parkville,
Melbourne VIC 3052, Australia.
Tel: +61 3 83872146
Fax: +61 3 83872222
E-mail: fary.khan@mh.org.au
Received: November 06, 2015; Accepted: December 04, 2015; Published: December 07, 2015
Citation: Khan F, Amatya B, Rathore FA, Galea MP (2015) Medical Rehabilitation in Natural Disasters in the Asia-Pacific Region: The Way Forward. Int J Natural Disaster Health Secur, 2(2), 6-12. doi: dx.doi.org/10.19070/2572-7540-150002
Copyright: Khan F© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium,provided the original author and source are credited.
Abstract
The Asia-Pacific is the most disaster-prone region in the world, with over 40% of the world's disasters occurring here in the past decade. This region has geo-political and socio-economic diversity which increases vulnerability to natural and other disasters. With increasing frequency of natural disasters, there is greater focus on the role of rehabilitation in disaster response and management. Early rehabilitation and preventative care in disaster survivors has the potential to minimize complications, optimize early recovery and reduce the economic burden. This article presents an overview of medical rehabilitation status in natural disaster settings in the Asia-Pacific region. It highlights the role of medical rehabilitation in disaster response and management, potential challenges faced by the countries in the region and key initial perspectives which need consideration for future disaster planning. Rehabilitation and long-term management of disaster survivors requires diverse forms of multi-sectorial partnerships, strategic collaboration, provision of service developments, research and knowledge transfer.
2.Introduction
3.Key Regional Initiatives in Disaster Management
4.Medical Rehabilitation in Disaster Settings
5.Physical Medicine and Rehabilitation professionals challenges in disaster settings
6.Identified Gaps for Action
6.1.Collaboration and governance
6.2.Building capacity in rehabilitation (including regional capacity)
6.3.Person-centred multidisciplinary care
6.4.Improve communication (information gathering, sharing and disseminating)
6.5.Increase public awareness and active participation/inclusion of disaster survivors/family/community partners
6.6.Strengthen evidence-based information, Education and access to information
6.7.Strengthen community-based rehabilitation
7.Summary
8.Acknowledgements
9.References
Keywords
Natural Disaster; Rehabilitation; Disability; Disaster Response; Outcome.
Introduction
A disaster is ‘a serious disruption of functioning of society, which poses a significant, widespread threat to human life, health, property or the environment, whether arising from accident, nature or human activity, whether developing suddenly or as a result of long-term processes, but excluding armed conflict’ [1]. Based on the aetiology, disasters can be classified into: a ‘man-made’(war, conflict etc.) or ‘natural’ [2]. A ‘natural disaster' is 'a situation or event caused by nature, which overwhelms local capacity, necessitating a request to a national or international level for external assistance; an unforeseen and often sudden event that causes great damage, destruction and human suffering' [3]. Natural disasters can be: Geophysical (earthquake, volcano, dry mass movement); Meteorological (storms); Hydrological (flood, wet mass movement); Climatological (extreme Temperature, drought, wildfire/bushfire); and Biological (epidemic, insect infestation, animal stampede)[3].
The Asia-Pacific is the most disaster-prone region in the world, with over 40% of the world's disasters occurring in this region in the past decade. These include earthquakes, cyclones, landslides/ floods, drought and bush-fires [4]. According to United Nation (UN) Economic and Social Commission for Asia and Pacific (ESCAP) report, of the 3,979 disasters that occurred globally between 2005 and 2014, over 1,625 occurred in this region, resulting in half a million fatalities (almost 60% of the total global deaths related to disasters) [5]. These disasters affected over 1.4 billion people and constitute 80% of those affected globally [5]. The economic losses resulting from these is estimated at US $523 billion [5]. In 2014 alone, more than half of the world’s 226 natural disasters occurred in the Asia-Pacific region, with over $60 billion worth of economic damage [6]. It is projected that by the year 2030, the region could average $160 billion per year of annual economic losses [5]. Hydrological disasters (floods/ storms) are common in the region, and result in higher economic damage relative to human toll. A list of major disasters that occurred in the Asia-Pacific region between 2000 to 2015 are listed in Table 1[7].
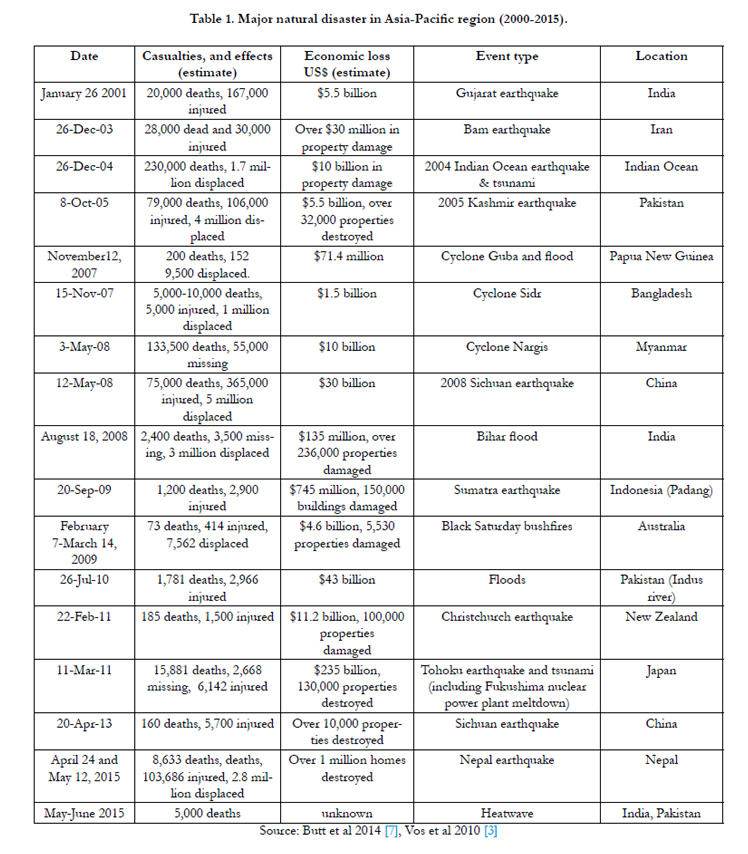

Table 1. Major natural disaster in Asia-Pacific region (2000-2015).
The Centre for Research on the Epidemiology of Disasters (CRED), predicts that natural disasters will escalate every year worldwide, and the Asia-Pacific region remains the most susceptible to these in the future [8]. The region has the highest disaster risk potential as the world’s two most seismically active fault lines cross many countries in this region [5, 9]; it has three major ocean basins and many areas lie along major typhoon tracks [5]. Further, the region is more prone to hydrological disasters due to climate change-related events (such as rising seas, increasing drought, rainfall etc.). The region, therefore, experiences some of the world's worst natural hazards such as earthquakes, volcanic eruptions, cyclones and monsoons [9].
The Asia-Pacific region is amongst the most diverse in the worldgeographically, economically and politically [10]. The remarkable geographical diversity ranges from tiny island nations in the Pacific (such as Kiribati, Vanuatu), to populous countries like China and India [11]. Many countries in the region are also affected by man-made disasters (such as war, conflict etc.). Economically, the region has vast diversity, ranging from economic superpowers (such as Japan, China, Australia) to the world’s poorest countries (such as Bangladesh, Nepal etc.). The region accounts for more than 60% of the world’s poverty-stricken people with over 770 million people living on less than $1.25 a day [5, 12]. These people are most vulnerable to the catastrophes as they live in more exposed areas, have weak livelihoods and fewer resources. Further, the region has many of the world's megacities with over 8 million people (such as Mumbai, Beijing, Manila), with exposure of a large population to hazard risk. [7]. Natural disasters potentially can have serious economic implications and can derail both national and individual household economies, which are already over strained and weak in most low-economic countries [4]. Further, weak governance can impede any disaster risk reduction and effective management. According to the Asian Development Bank, the region’s economic progress will be undermined by the rising number of disasters [12].
Despite progress in surveillance and early warning systems and evacuations, the Asia-Pacific region is still largely unprepared for its response to mega-disasters [4]. This requires improved regional information exchange, strengthened regional cooperation for effective post-disaster management and joint coordination to address cross-border disasters [4, 6, 8]. The Asia-Pacific region's poor population remain vulnerable and exposed to disasters, and have borne the brunt of these cataclysms.
Key Regional Initiatives in Disaster Management
In recent years, there have been improvements in international and regional collaboration; and management capacities in disaster management. There is increased attention on disaster prevention and preparedness, especially early warning systems, early evacuation (for hydrological disasters) and awareness. In 1947, the UN established the Economic and Social Commission for Asia and the Pacific (ESCAP) as an intergovernmental forum for all countries in the region (53 members, 9 associates), covering over 60% of the world’s population (4.1 billion people). In 2004, ‘The Hyogo Framework for Action’ (Kobe), was adopted after the Indian Ocean tsunami, aimed at reducing disaster-related losses, both of human, and social, economic and environmental assets. The UN General Assembly (September 2005), implemented this framework through the International Strategy for Disaster Reduction in Asia to enhance regional co-operation. Although, ‘The Hyogo Framework’ provides a strong foundation for governments to take on a greater role at all levels, it is based on voluntary commitment and is limited in its capacity to move certain actions forward [4]. Currently, leaders and decision-makers across the region are preparing to finalize a new global framework for disaster risk reduction to replace the Hyogo Framework [4].
In the wake of Cyclone Nargis (Myanmar 2008), the Association of Southeast Asian Nations (ASEAN) Humanitarian Task Force was established, which effectively led the coordination and distribution of aid to victims. The ASEAN Agreement on Disaster Management and Emergency Response 2010–2015 (AADMER) was ratified by ten member states, and in 2009, issued a statement on disaster management to enhance regional preparedness for natural disasters. The Pacific Platform for Disaster Risk Management (PPDRM) Framework for Action 2010–2015 was adopted in August 2010, to enhance disaster risk management in Pacific countries. In 2011, the Indian Ocean Tsunami Warning and Mitigation System was established. Currently, most countries in the region have some form of legal and regulatory framework as well as institutional structures for managing disaster risk [4]. However, there are still major disparities and gaps amongst the member countries and those with high disaster risks tend to have low coping capacity [5]. Many countries have already introduced disaster resistance building codes, however, due to poverty and lack of regulatory and meaningful enforcement, much of the infrastructure is yet to meet optimal standards.
Medical Rehabilitation in Disaster Settings
Due to advances in response, rescue and field management, emergency/ surgical and medical care (including infection control) in many disasters, there has been authoritative transition worldwide from high mortality to a significant increase in morbidity rates [13]. The disaster victims are surviving at relatively higher rates, however, many have a range of long-term severe physical and psychological injuries which impact their quality of life. Further, those with pre-existing disabilities and additional co-morbidities are at risk of higher mortality and further morbidities as a result of a natural disaster [14]. These people require integrated interdisciplinary care from the acute phase of disaster management to sub-acute care (in hospital and/or community) to enable their previous level of function and reintegration into the community [15]. This highlights medical and non-medical rehabilitation (rehabilitation services, infrastructure, buildings etc.) as integral to comprehensive disaster management [2, 15, 16, 17].
Medical rehabilitation is ‘a set of measures that assist individuals who experience (or are likely to experience) disability to achieve and maintain optimal physical, sensory, intellectual, psychological and social functioning in interaction with their environment’ [17]. Primary goals of medical rehabilitation include management of acute injury, optimization of functional capabilities (including physical, cognitive, neuropsychological function) and social reintegration [14]. Rehabilitation in disaster setting includes: assessment of injury patterns, needs and resource requirements (including long-term); establishment of patient triage, discharge, referral, and tracking systems; collaboration with other healthcare service providers; coordination with emergency response systems, host health system and government managers; and data collection, management and analysis [13, 14]. Long-term rehabilitation planning is critical for community recovery where services should be accessible, and include general health maintenance [2, 14]. The treating team includes physical and rehabilitation medicine (PRM) physicians, nurses and allied health professionals.
As aforementioned, natural disasters can cause complex disabilities, which are costly to treat and have socioeconomic implications due to increased demand for long-term health care, social and vocational services, and caregiver burden [2, 14]. There is strong consensus that medical rehabilitation in any humanitarian disaster should be initiated in the immediate emergency response phase, and as disaster transitions away, it should continue in the community over a longer-term to restore function and enhance participation of survivors, affected directly or indirectly in the disaster [15, 18]. There is evidence suggesting early involvement of rehabilitation in disaster setting, reduces disability post-operative complications and improves participation (quality of life) [2, 13, 14]. The WHO advocates that “rehabilitation is one of the core functions of trauma care systems in regular healthcare and as such, Foreign Medical Teams (FMT) should have specific plans for the provision of rehabilitation services to their patients post sudden-onset disasters” [19]. This aligns with the vision and objectives of the WHO Global Disability Action Plan 2014-2021 and the implementation of United Nations Convention on the Rights of Persons with Disability (CRPD)[20, 21].
Despite significant improvements in the coordination and organization of acute care services in emergency responses worldwide, this has not extended to include rehabilitation services [13]. Acute medical response in disaster settings focuses on saving lives and acute injuries get much of the attention, while rehabilitative needs are often neglected [2, 14, 22]. In many Asia-Pacific countries, disaster response plans and rehabilitation services are generally inadequate or absent [6]. There is a lack of access to appropriate services in many countries, where fragmented healthcare systems are compromised by lack of financial and political support [4, 5]. During disasters, often the existing local rehabilitation resources can be damaged and/or disrupted and can be quickly overwhelmed with an influx of injury/disease and require international humanitarian assistance [23] To date, there is no documentation of inclusion of the rehabilitation professionals in the emergency-response staffing configuration in any disasters in the Asia-Pacific region. The need for overall rehabilitation services in these countries during disasters is not well defined in terms of type, intensity and settings. On many occasions, rehabilitation services are integrated with other health services in public hospital systems, where there are no services for specific and complex disaster-related disabilities, such as spinal cord injury (SCI) [24]. Further, there is lack of disability-disaggregated data within general statistics for disaster zones [23].
Improving or restoring physical and psychosocial abilities is a key issue in rehabilitation of disaster victims, and rehabilitation approaches should include a spectrum of treatments and interventions [13, 14]. The role of the PRM physician is critical in disaster settings to coordinate the post-disaster rehabilitation needs and management of victims [13]. Earlier experiences in disaster zones have raised awareness and need for inclusion of rehabilitation in response and planning for humanitarian catastrophes [18, 25]. Studies evaluating the effectiveness of rehabilitation intervention following a natural disaster are scarce [2, 13]. A few studies have investigated a variety of medical rehabilitation interventions for natural disaster survivors, which range from comprehensive multidisciplinary rehabilitation to community educational programs [2]. The overall, findings from these studies suggest that postdisaster rehabilitation was effective in reducing disability, improving participation and quality of life [2] (Table 2). Further, other studies have demonstrated that involvement of PMR physicians in the disaster zone resulted in positive and better clinical outcomes, reduced lengths of hospital stay and fewer complications [24, 26].
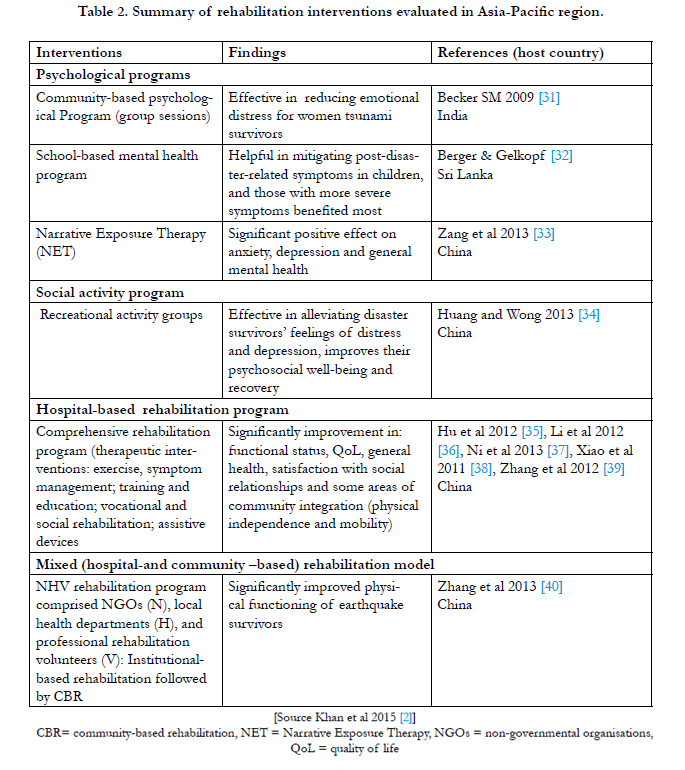
Table 2. Summary of rehabilitation interventions evaluated in Asia-Pacific region.
Physical Medicine and Rehabilitation professionals challenges in disaster settings
The many challenges for rehabilitation professionals during disaster settings in the Asia-Pacific region include [2, 13, 14, 22, 27]:
- Rehabilitation infrastructure/services are not fully developed, or existing host healthcare infrastructure disrupted or destroyed due to unprecedented volume of are disaster victims
- Rehabilitation services are mainly hospital-based and overwhelmed requiring make-shift centres
- Discharge from the healthcare facilities into community is difficult due to lack of appropriate, accessible housing, adding pressure to an overstretched healthcare infrastructure
- Lack of coordination with and amongst disaster management organisations (including FMTs), which are predominantly deployed in the acute phase; and with national and international non-governmental organisations (NGOs)
- Many FMTs do not include rehabilitation physicians or their inclusion is restricted to the intermediate and longer-term settings only
- Lack of skilled human resources locally (e.g., PRM physicians), which limits access to skilled multidisciplinary care
- Hospital-orientated units are unable to serve longer-term needs of disabled people with residual functional and psychological disabilities
- Inadequate community rehabilitation resources and facilities
- Limited psychological support and cognitive rehabilitation for those with post-traumatic stress disorders (PTSD)
- Lack of relevant and purposeful reporting and tools to review services provided to those affected by disaster and improve humanitarian coordination for long-term care planning
- Deployment to affected areas is complicated by damaged and/or disrupted infrastructure (as roads, transport, communications etc.)
- Cultural beliefs of people affected about disability and the disaster itself may limit potential impact of rehabilitative services.
Identified Gaps for Action
With increasing frequency of natural disasters in the Asia-Pacific region, there is greater focus on the role of rehabilitation in disaster management. Many disaster survivors, such as those with traumatic brain injuries (TBI), SCI etc. are vulnerable populations requiring long-term planning for service delivery and rehabilitation [24]. Early aggressive rehabilitation and preventative care in these survivors has the potential to minimize complications,facilitate early recovery and reduce the economic burden [13, 14]. Specifically, there are some key initial perspectives which need consideration for future disaster planning, listed below:
The establishment of a national disaster response healthcare organisation is recommended for a leadership role to coordinate and provide cooperative effort, and to enhance capacity of national and international health care organisations (and FMTs), for effective management and preparedness in disaster settings. These should include inter-disciplinary and inter-sectoral partnershipsfor disaster management, preparedness, emergency response and longer-term planning. Allnational and international representative organisations (including NGOs) should be stakeholders and participate, contribute to planning, monitoring and evaluation of disaster management agenda and processes, including rehabilitation. The governing body (and stakeholders) should build up the system by enhancing capacities of healthcare institutions, individuals and communities in the care process. For example, in Australia, the the federal Department of Health established the Australian Medical Assistance Teams (AusMAT), which is a comprehensive management system capable of responding to disaster both nationally and internationally [28]. The AusMAT comprises multi-disciplinary teams of doctors, nurses, paramedics, pharmacists, fire-fighters (logisticians), allied health and environmental health staff [28].
Several countries in the Asia-Pacific region do not have adequate rehabilitation capacity in terms of human resources, services and funding. The regional member countries need to develop self-sustaining rehabilitation capacity (at various levels) and collaborate in capacity building to manage the after math and impact of disasters in the longer-term. The ASEAN collaboration can be much more effective. The International Society of Physical and Medical Rehabilitation established it’s Committee for Disaster Relief to enhance capacity building in medical rehabilitation with focus on the Asia- Pacific. Further, the WHO published the ‘Classification and Minimum Standards for Foreign Medical Teams in Sudden Onset Disasters’ in 2013 [19] which provides guiding principles and core standards for all FMTs, and recommends rehabilitation as a minimum standard. The ‘Emergency Medical Teams: Minimum Standards for Rehabilitation’ document (in draft) provides guidance and standards on rehabilitation requirements such as elements of rehabilitation service provision, workforce, quality assurance for patient management, equipment and consumables, accessibility, information management; research and development (personal communication with the publication team).
All survivors should be assessed with individualised care plans including rehabilitation [2, 13, 14]. The post-disaster MD team
may include: PMR physicians, treating medical/surgical and allied health personnel. Treatment goals should be non-discriminatory and aligned with UN Convention of the Rights of Persons with Disabilities[19].
Improvement in accessibility and overcoming information barriers are a priority in any disaster effort. Data should be collected by relevant services, with a‘lead’ governing agency facilitating and coordinating this information for dissemination, to relevant authorities for longer-term management in the community [14, 23]. Fostering understanding and learning from past experiences in disaster management through knowledge exchange and greater access to information/data is crucial for future capacity building and planning.
Personal preparedness and active participation of the survivors (and families) should be included in decision making and goal settings, which contribute to effective longer-term management. Disaster survivors should be empowered and educated to actively participate in, and contribute to, the development and monitoring of treatment plans, programs and actions.
Access to information and knowledge in post-disaster management can be fragmented and inequitable [29]. Timely dissemination of information enables active participation and contribution from treating teams. All stakeholders (and related organisations) with expertise should be considered for knowledge transfer and education. Multi-stakeholder partnerships should build and implement evidence-based disaster-management approaches for informed decisions and effective action. Regular data collection during disaster management enhances reporting and accountability for disaster survivors. These data can highlight clinical gaps in care so lessons may be learnt for future disaster management. Governments should collaborate with treating teams and community organisations to implement and define existing and new commitments.
Various initiatives should be in place to empower and strengthen community-based organisations for longer-term rehabilitation of disaster survivors (especially women, children, older and disabled persons) in the community. Inclusive risk reduction strategies prior to and after a disaster should reduce vulnerability, and mitigate the impact of disaster and further loss of life. Further, the government should assure the socio-economic security of individuals and communities, where possible.
Summary
The Asia-Pacific region remains highly vulnerable to frequent natural disasters. Disaster risk and disaster-related human sufferings are escalating due to the emerging effects of climate change, population growth, rapid urbanization, development patterns and growing poverty. The lessons from past disasters show that building longer-term management approaches (including rehabilitation) remain a key priority in any disaster-management plan. The longer-term health consequences and disability can be overwhelming for the survivors (their families), society and the health system. The year 2015 marks the end of the ‘Hyogo Framework for Action’, and the beginning of a new 15-year plan – the ‘Sendai Framework for Disaster Risk Reduction 2015-2030’, which sets up an agenda for all sectors of society for collaborative effort for successful future disaster planning and management [30].
Disaster management in a broader sense is consequently a burgeoning field in the developing world. At a national level, the capacity building approach needs to include the development of an integrated disaster risk management plan; emergency response management; inter-sectoral and interdisciplinary partnership amongst governmental, private, national and international sectors; increasing public awareness and involving the victims and their families in the management plan; longer-term care and rehabilitation of victims; and strengthening community-based rehabilitation. Longer-term management of disaster survivors requires diverse forms of multi-stakeholder partnerships (including governmental bodies, local health-care institutions, NGOs and civil society organizations) related to persons with disabilities, FMTs, community organisations and the private sector.
Effective future disaster management will depend on the capacity and willingness of countries and communities across the regionto embrace and disseminate effective methods of disaster risk governance and preparedness, and develop appropriate policies for a collaborative and coordinated management system. The challenge ahead is developed a comprehensive, targeted and integrated approach to disaster risk management and post-disaster management (including rehabilitation), stretching across sectors and jurisdictions and reaching vulnerable communities at risk.
Acknowledgements
This review was supported from internal resources of the Rehabilitation Department, Royal Melbourne Hospital, Royal Park Campus, Melbourne, Australia. The authors are grateful toDrs Jim Gosney, Jan D. Reinhardt and the Committee on Rehabilitation Disaster Relief (CRDR), International Society of Physical and Rehabilitation Medicine (ISPRM), and Foreign Medical Team Working Group, World Health Organisation (WHO) for their support.
References
- ReliefWeb Project (2008) Glossary of humanitarian terms. Available from: www.reliefweb.int/glossaries
- Khan F, Amatya B, Gosney J, Rathore FA, Burkle FM Jr. (2015) Medical Rehabilitation in Natural Disasters: A Review. Arch Phys Med Rehabil 96(9): 1709-1727.
- Vos F, Rodriguez J, Below R, Guha-Sapir D (2010) Annual Disaster Statistical Review 2009: The Numbers and Trends. Centre for Research on the Epidemiology of Disasters (CRED), Brussels. 1-37.
- Brassard C, Giles DW, Howitt AM (2015) Natural Disaster Management in the Asia-Pacific: Policy and Governance, In: Disaster Risk Reduction: Methods, Approaches and Practices. Springer , Kyoto, Japan.
- Economic and Social Commission for Asia and the Pacific (ESCAP) (2015) Disasters Without Boarders: Regional Resilience for Sustainable Development. Asia-Pacific Disaster Report United Nations, Bangkok.
- Economic and Social Commission for Asia and the Pacific (ESCAP) (2015) Disasters in Asia Pacific: 2014 year in review. United Nations, Bangkok.
- Butt S, Hitoshi N, Nottage L (2014) Asia-Pacific Disaster Management. Comparative and Socio-legal Perspectives. Springer, Heidelberg.
- Economic and Social Commission for Asia and the Pacific (ESCAP) (2015) Economic and Social Survey of Asia and the Pacific. United Nations, Bangkok.
- International Council for Science (2008) Science plan on hazards and disasters: earthquakes, floods and landslides. ICSU Regional Office for Asia and Pacific, Kuala Lumpur, Malaysia.
- Simpson A, Cummins P, Dhu T, Griffin J, Schneider J (2008) Assessing natural disaster risk in the Asia-Pacific region. AusGeo News 90.
- Economic and Social Commission for Asia and the Pacific (ESCAP) (2014) ESCAP Annual Report. United Nations, Bangkok.
- Independent Evaluation Department (2012) ADB’s Response to Natural Disasters and Disaster Risks. Asian Development Bank (ADB).
- Reinhardt JD, Li J, Gosney J, Rathore FA, Haig AJ, et al. (2011) Disability and health-related rehabilitation in international disaster relief. Glob Health Action 4: 7191.
- Rathore FA, Gosney JE, Reinhardt JD, Haig AJ, Li J, et al. (2012) Medical rehabilitation after natural disasters: why, when, and how? Arch Phys Med Rehabil 93(10): 1875-1881.
- Gosney J, Reinhardt JD, Haig AJ, Li J (2011) Developing post-disaster physical rehabilitation: role of the World Health Organization Liaison Sub- Committee on Rehabilitation Disaster Relief of the International Society of Physical and Rehabilitation Medicine. J Rehabil Med 43(11): 965-968.
- Dhameja A (2008) Disaster rehabilitation: towards a new perspective. In: Disaster management handbook. CRC Press, FL, USA.
- World Health Organization (2011) World Report on Disability. WHO, Geneva, Switzerland.
- Landry MD, McGlynn M, Ng E, Andreoli A, Devji T, et al. (2010) Humanitarian response following the earthquake in Haiti: reflections on unprecedented need for rehabilitation. World Health Popul 12(1): 18-22.
- Norton I, von Schreeb J, Aitken P, Herard P, Lajolo C (2013) Classification and Minimum Standards for Foreign Medical Teams in Sudden Onset Disaster. WHO, Geneva.
- United Nations (2006) Convention on the Rights of Persons with Disabilities. www2.ohchr.org/english/law/disabilities-convention.htm.
- World Health Organization (2014) WHO global disability action plan 2014–2021: Better health for all people with disability. WHO, Geneva.
- Khan F, Amatya B, Mannan H, Burkle FM Jr, Galea MP (2015) Rehabilitation in Madagascar: Challenges in implementing the World Health Organization Disability Action Plan. J Rehabil Med 47(8): 688-696.
- Nickerson JW, Chackungal S, Knowlton L, McQueen K, Burkle FM (2012) Surgical care during humanitarian crises: a systematic review of published surgical caseload data from foreign medical teams. Prehosp Disaster Med 27(2): 184-189.
- Rathore MF, Rashid P, Butt AW, Malik AA, Gill ZA, et al. (2007) Epidemiology of spinal cord injuries in the 2005 Pakistan earthquake. Spinal Cord 45(10): 658-663.
- Landry MD, O'Connell C, Tardif G, Burns A (2010) Post-earthquake Haiti: the critical role for rehabilitation services following a humanitarian crisis. Disabil Rehabil 32(19): 1616-1618.
- Gosney JE Jr. (2010) Physical medicine and rehabilitation: critical role in disaster response. Disaster Med Public Health Prep 4(2): 110-112.
- Smith E, Wasiak J, Sen A, Archer F, Burkle FM Jr. (2009) Three decades of disasters: a review of disaster-specific literature from 1977-2009. Prehosp Disaster Med 24(4): 306-311.
- National Critical Care and Trauma Response Centre (2015) Australian Medical Assistance Teams (AUSMAT) www.nationaltraumacentre.nt.gov.au/what-we-do/disaster-management/ausmat.
- Olness K, Sinha M, Herran M, Cheren M, Srivieng P (2005) Training of Health Care Professionals on the Special Needs of Children in the Management of Disasters: Experience in Asia, Africa, and Latin America. Ambul Pediatr 5(4): 244-248.
- United Nations Office for Disaster Risk Reduction (2015) Sendai Framework for Disaster Risk Reduction 2015-2030. UNISDR, Geneva.
- Becker SM (2009) Psychosocial Care for Women Survivors of the Tsunami Disaster in India. Am J Public Health 99(4): 654-658.
- Berger R, Gelkopf M (2009) School-Based Intervention for the Treatment of Tsunami-Related Distress in Children: A Quasi-Randomized Controlled Trial. Psychother Psychosom 78(6): 364-371.
- Zang Y, Hunt N, Cox T (2013) A randomised controlled pilot study: the effectiveness of narrative exposure therapy with adult survivors of the Sichuan earthquake. BMC Psychiatry 13: 41.
- Huang Y,Wong H (2013) Effects of social group work with survivors of the Wenchuan earthquake in a transitional community. Health Soc Care Community 21(3): 327-337.
- Hu X, Zhang X, Gosney JE, Reinhardt JD, Chen S, et al. (2012) Analysis of functional status, quality of life and community integration in earthquake survivors with spinal cord injury at hospital discharge and one-year followup in the community. J Rehabil Med 44(3): 200-205.
- Li Y, Reinhardt JD, Gosney JE, Zhang X, Hu X, et al. (2012) Evaluation of functional outcomes of physical rehabilitation and medical complications in spinal cord injury victims of the Sichuan earthquake. J Rehabil Med 44(7): 534-540.
- Ni J, Reinhardt JD, Zhang X, Xiao M, Li L, et al. (2013) Dysfunction and post-traumatic stress disorder in fracture victims 50 months after the Sichuan earthquake. PLoS One 8(10): e77535.
- Xiao M, Li J, Zhang X, Zhao Z (2011) Factors affecting functional outcome of Sichuan-earthquake survivors with tibial shaft fractures: a follow-up study. J Rehabil Med 43(6): 515-520.
- Zhang X, Hu XR, Reinhardt JD, Zhu HJ, Gosney JE, et al. (2012) Functional outcomes and health-related quality of life in fracture victims 27 months after the Sichuan earthquake. J Rehabil Med 44(3): 206-209.
- Zhang X, Reinhardt JD, Gosney JE, Li J (2013) The NHV RehabilitationServices Program Improves Long-Term Physical Functioning in Survivors of the 2008 Sichuan Earthquake: a longitudinal quasi Experiment. PLoS One 8:e53995.





