Seroprevalence of Toxoplasma gondii Infection among Pregnant Women in the Ashanti Region of Ghana
Sefah-Boakye J1*, Frimpong E. H2, Dompreh A3, Turpin, A. C4
1 School of Graduate Studies, Department of Clinical Microbiology, School of Medical Sciences, College of Health Sciences, KNUST, Kumasi, Ghana.
2 Professor of Clinical Microbiology, Department of Clinical Microbiology, School of Medical Sciences, College of Health Sciences, KNUST, Kumasi, Ghana.
3 Head of Serology/Virology, Komfo Anokye Teaching Hospital, Kumasi, Ghana.
4 Professor and Head of Obstetrics and Gynaecology, School of Medical Sciences, College of Health Sciences, KNUST, Kumasi, Ghana.
*Corresponding Author
Sefah-Boakye, Justine
School of Graduate Studies, Department of Clinical Microbiology, School of Medical Sciences, College of Health Sciences, KNUST, Kumasi, Ghana.
Tel: 233(243)419217
Email: sefahboakye86@yahoo.com
Article Type: Research article
Recieved: April 13, 2016; Accepted: May 18, 2016; Published: May 24, 2016
Citation: Sefah-Boakye J, Frimpong E. H, Dompreh A, Turpin, A.C (2016) Seroprevalence of Toxoplasma gondii Infection among Pregnant Women in the Ashanti Region Of Ghana. Int J Microbiol Adv Immunol. 04(1), 70-74.
dx.doi.org/10.19070/2329-9967-1600013
Copyright: Sefah-Boakye J© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Toxoplasma gondii infection is a zoonotic protozoan infection that affects warm-blooded animals, including humans. Congenital toxoplasmosis occurs when unborn and developing foetus becomes infected with T. gondii through the placenta in utero. The study sought to determine the seroprevalence of T. gondii infection among pregnant women seeking antenatal care at the Manhyia District Hospital, Kumasi. Signed or thumb printed consent form, structured questionnaires, as well as, about 3mls of venous blood was taken from 110 pregnant women for the study. Analysis of blood sera using commercial ELISA kit (Teco Diagnostics, 1268 N, Lakeview Ave., Anaheim, CA 92807, USA) showed that, 71.8% (79/110) were seropositive for T. gondii IgG antibodies whiles 39.1% (43/110) were seropositive for T. gondii IgM antibodies. A total of 30 representing 27.3% of the pregnant women were seropositive for both T. gondii IgG and IgM antibodies. Again, 44.5% (49/110) was reported for pregnant women with only T. gondii IgG antibodies and 11.8% (13/110) for only T. gondii IgM antibodies. The overall seroprevalence of toxoplasma IgG and IgM antibodies for the study was 83.6% (92/110).
It is recommended that screening of pregnant women for toxoplasmosis be done during routine antenatal laboratory test. Again, it is recommended that, a study to determine the risk factors for T. gondii infection among pregnant women in the Ashanti region of Ghana be done.
2.Introduction
3.Materials and Methods
3.1 Subjects and Sample collection
3.2 Inclusion/Exclusion Criteria
4.Results
5.Discussion
5.Conclusion
7.References
keywords
ELISA Test; Coccidians; Congenital Toxoplasmosis; Zoonotic Protozoans.
Introduction
Toxoplasma gondii infection is a protozoan infection that affects warm-blooded animals, including humans [1]. It is a zoonotic infection caused by T. gondii, an obligate intracellular protozoan of cats that infects humans and other mammals, including birds as intermediate hosts. T. gondii belongs to subphylum Apicomplexa, Class Sporozoa and exists in three main forms. These forms are [2].
- The oocysts, which are the infective form and release sporozoites
- Trophozoites/tachyzoites, which are the asexual form responsible for cell invasion and are crescent shaped. They are seen during acute stage of infection and invades all types of mammalian cells, except non-nucleated red blood cells (RBCs).
- Types of mammalian cells, except non-nucleated red blood cells (RBCs).
- The tissue cyst/Bradyzoites, which are made up of intracellular trophozoites and develop within cytoplasm of host cell.
The tissue cyst and oocysts are the main forms of the parasite that are involved in its transmission.
Infection of T. gondii is high in areas with hot, low altitudes and humid climatic conditions [3]. Human infection of toxoplasmosis occurs through.
- Ingestion of tissue cysts in poorly cooked meat
- Ingestion of food or water contaminated with mature oocysts faeco-orally
- Transplacental (vertical) transmission from mother to foetus in utero
- Although rare, needlestick injury, organ transplantation and blood transfusion from seropositive donors.
Toxoplasmosis is estimated to affect nearly a third of the global population [4,5]. Again, it has been estimated that between 30% and 65% of the global population are infected with toxoplasmosis [4].
Congenital toxoplasmosis occurs when unborn and developing foetus becomes infected with T. gondii through the placenta in utero. Maternal-fetal transmission of T. gondii occurs between one and four months after placenta has been colonized by tachyzoites [6,7]. Congenital toxoplasmosis has adverse health consequences on pregnancies and newborns [8,9]. The risk of congenital infection from acute T. gondii infection in pregnancies ranges between 20% and 50% when strict treatment regimens are not adhered [7,10,11].
T.gondii hardly causes infections except when acquired congenitally [2]. Consequences such chorioretinitis, hydrocephalus, microcephalus, intracranial calcification, encephalitis and convulsions are commonly related to T. gondii infection in pregnancies. Intrauterine growth restrictions and intrauterine foetal death are some common signs of in utero infection of T.gondii in severe cases [7,11].
Development of toxoplasmosis takes place after infection with T. gondii parasites congenitally or ingestion of contaminated tissue cysts in infected meat or sporulated oocysts in food or water contaminated with cat’s faeces [12]. During the incubation period of 5 to 18 days, the host cell becomes engaged and finally gets destroyed as a result of active multiplication by cell division of T. gondii [13].
A more severe form of congenital toxoplasmosis involves infection of the retina and causes chorioretinitis which is characterized by vision impairment [7,11]. When the brain is involved in congenital toxoplasmosis, mostly in immunosuppressed patients, necrotic abscess of the brain may occur [7,11].
In Ghana, prevalence studies on toxoplasmosis have been concentrated at the Greater Accra region. A seroprevalence of 76.0% of toxoplasma antibodies was reported among pregnant women attending prenatal clinic at the Mamprobi Clinic, Accra [14]. Similarly, the overall seroprevalence of T. gondii IgG, IgA and IgM antibodies in the Greater Accra region was estimated as 92.5% [15]. Again, T. gondii IgG antibodies of 73.6% against 76.1% for T. gondii IgM antibodies were estimated in the Greater Accra region of Ghana [15]. In Ghana, 32.7% seroprevalence of T. gondii IgG antibodies against 29.7% for T. gondii IgM antibodies has been reported in the Greater Accra region [4]. Moreover, an overall seroprevalence of T. gondii antibodies is estimated as 49.7% in the Greater Accra region [4]. A T. gondii IgG antibody of 37.6% against 0.0% for T. gondii IgM antibodies has been estimated in the Greater Accra region [16]. The main objective of the study was to determine the seroprevalence of T. gondii infection among pregnant women seeking antenatal care (ANC) at the Manhyia District Hospital, Kumasi in the Ashanti Region of Ghana.
Materials and Method
The study was undertaken at the Manhyia District Hospital because it constantly records high ANC attendance of at least 30 daily. The study involved randomly recruiting 110 pregnant women aged between 15 and 40 years and attending the ANC clinic. About 3mls of venous whole blood was drawn aseptically from each enrolled pregnant woman into serum separator tubes. It was then centrifuged at 1000 rpm for 10 minutes and blood sera separated into labeled cryotubes and stored at -20°C until use. Again, questionnaires and signed or thumb printed consent forms were received from recruited pregnant women. Quantitative determination of the levels of T. gondii IgG and IgM antibodies in participant’s serum was determined using commercial ELISA kit (Teco Diagnostics, 1268 N, Lakeview Ave., Anaheim, CA 92807, USA) in accordance with manufacturer’s procedure.
Study participants had to meet the inclusion criteria to be included in the study.
Inclusion Criteria
Pregnant women aged between 15 and 40 years and attending the ANC clinic at the Manhyia District Hospital, Kumasi were enrolled for the study. Again, pregnant women enrolled were certified to be medically fit by the Specialist Obstetrician and Gynaecologist, including having haemoglobin (Hb) concentration of at least 12.0 g/dl. Additionally, pregnant women were included in the study upon signing/thumb printing the consent form for the study.
Exclusion Criteria
- Pregnant women who failed to sign/thumb print the consent form were excluded from the study
- Pregnant women with Hb less than 12.0 g/dl were not considered for the study.
- Pregnant women who were deemed medically unfit based on medical history and assessment were not considered for the study.
Scientific Program for Social Sciences (SPSS, Version 16) software and Microsoft Excel was used to analyze data from the study.
Results
Out of the 110 pregnant women enrolled for the study, 63.6% (70/110) were aged between 21 and 30 years with 30.0 % (33/110) between 31 and 40 years. Again, 85.5% (94/110) and 13.6% (15/110) were within the third and second trimesters of pregnancy respectively. None of the 110 (0.0 %) pregnant women enrolled for the study had ever been screened for toxoplasmosis.
ELISA conducted for T. gondii IgG antibodies indicated 79 were seropositive. This represented 71.8% with 28.2% (31/110) seronegative for T. gondii IgG antibodies. From the 110 pregnant women enrolled, 43 representing 39.1% were ELISA T. gondii IgM antibodies seropositive with 60.9% (67/110) seronegative for Anti-T. gondii IgM. Both T. gondii IgG and IgM antibodies were present in 27.3% (30/110) of pregnant women enrolled. More so, 44.5% (49/110) and 11.8% (13/110) were reported for pregnant women with only T. gondii IgG and IgM antibodies respectively. The overall seroprevalence for the study was 83.6% (92/110) (Table 1).
From the 79 seropositives for ELISA T. gondii IgG antibodies, 64.6% (51/79) were aged between 21 and 30 years. Additionally, 3.8% (3/79) were between 15 and 20 years with 31.6% (25/79) aged between 31 and 40 years. The highest seroprevalence of T. gondii IgG antibodies was between the ages of 21 and 30 years. It was also observed that 96.2% (76/79) were between the ages of 21 and 40 years. The highest seroprevalence of T. gondii IgM antibodies of 55.8% (24/43) was between the ages of 21 and 30 with 95.3% (41/43) aged between 21 and 40 years (Table 2).
The study showed that, 87.3% (69/79) of the seropositives were in their third trimester of pregnancy with 11.4% (9/79) and 1.3% (1/79) in their second and first trimesters of gestation respectively. A total of 78 of the seropositives representing 98.7% were either in their second or third trimester of pregnancy. Anti-T. gondii IgM was present in 79.1% (34/43) of the pregnant women in their third trimester. Moreover, 20.9% (9/43) and 0.0% (0/43) of the seropositive T. gondii IgM antibodies were in their second and first trimesters of gestation respectively. All (100%) seropositive pregnant women were either in their second or third trimester of pregnancy (Table 3).
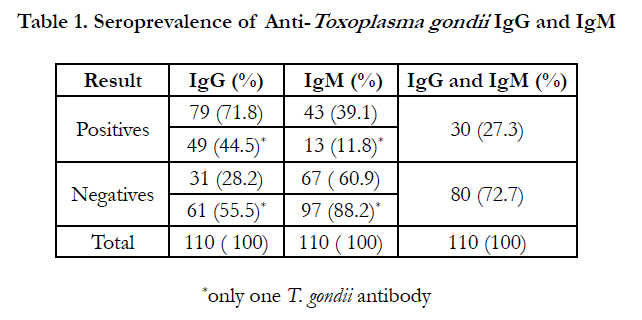

Table 1. Seroprevalence of Anti-Toxoplasma gondii IgG and IgM
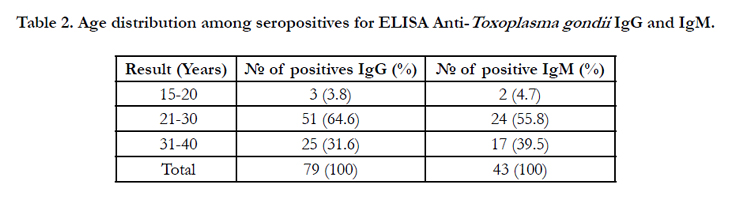
Table 2. Age distribution among seropositives for ELISA Anti-Toxoplasma gondii IgG and IgM.
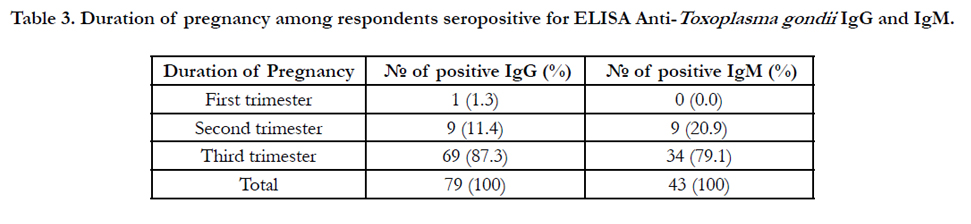
Table 3. Duration of pregnancy among respondents seropositive for ELISA Anti-Toxoplasma gondii IgG and IgM. IgG and IgM.
Discussion
Congenital toxoplasmosis poses risk to pregnancies and newborns and hence, remains an issue of public health concern [4,5]. In determining the seroprevalence of T. gondii infection among pregnant women attending ANC clinic at the Manhyia District hospital, it was observed that the seroprevalence of T. gondii IgG antibodies was 71.8% (79/110), which indicates a past exposure to T. gondii. This value of 71.8% is similar to a study in the Greater Accra region (Accra) which estimated a seroprevalence of anti-T. gondii IgG as 73.6% [15]. However, the seroprevalence of T. gondii IgG antibodies for the current study is lower than 81.1% reported by a study in the Southwestern and Central Ethiopia respectively [17,18]. In Nigeria, a study reported a lower seroprevalence of T. gondii IgG antibodies as 40.8% [19]. Again, a study reported lower seroprevalence of anti-T. gondii IgG of 32.7% and 37.6% respectively compared to the current study [4,16].
Similarly, 39.1% (43/110) was observed for T. gondii IgM antibodies. The significance of the seropositive T. gondii IgM antibodies indicates a recent exposure to T. gondii. The seroprevalence of T. gondii IgM antibodies of the current study is higher compared to 29.7% and 0.0% reported in the Greater Accra region (Accra) respectively [4,16]. However, a study in Accra reported the seroprevalence of anti-T. gondii IgM of 76.1% which is higher [15].
IgG immunoglobulins is a marker of chronic (old) infection and shows that an individual has been previously infected with infection (toxoplasmosis) whereas IgM immunoglobulin, a marker of acute (recent) infection, is used in determining the time of infection. The higher seroprevalence of T. gondii IgG antibodies as obtained from the study is comparable to a study which sought to show that, IgG are the most abundant immunoglobulin that are secreted in the body [20]. The presence of high levels of anti-T. gondii IgG in the body merely indicated past exposure to T. gondii. However, that does not distinguish recent infection from past infection of toxoplasmosis. The more seronegative anti-T. gondii IgM with a corresponding high seropositive anti-T. gondii IgG shows T. gondii infection of at least six months earlier. This is because IgM immunoglobulins appear much earlier following an infection than IgG immunoglobulins and disappear faster relative to IgG antibodies following recovery. This means IgM immunoglobulins are detected earlier during acquired primary infection. However, the titers of IgM immunoglobulins decrease and become negative within some few months. These assertions are consistent with a reported study [21].
From the study it was also observed that, 27.3% (30/110) tested seropositive to both T. gondii IgG and IgM antibodies. This is because some seropositive anti-T. gondii IgM titers, although some disappear, may reactivate during the chronic stage of the infection and hence test seropositive for anti-T. gondii IgG.
The high seropositive of both anti-T. gondii IgG and anti-T. gondii IgM of 87.3% (69/79) and 79.1% (34/43) respectively for pregnant women in their third trimester of gestation poses health risk to the pregnancies and newborns. This is because contraction of congenital toxoplasmosis prior to pregnancy is in most cases less fatal. This is attributed to the inability of the T. gondii to pass from the mother to the foetus in utero following establishment of immunity to the T. gondii infection. The condition may be fatal for pregnant women infected by T. gondii for the first time. This is because, as a result of lack of immunity, T. gondii may cross the placenta where they can infect the foetus. This may pose health risk to the foetus. It is for this reason that early diagnosis during pregnancy is most desirable so as to offer prompt management, including treatment. This may reduce the likelihood of placental transmission of T. gondii and eventually avoid risk to the foetus.
Furthermore, 44.5% (49/110) and 11.8% (13/110) were reported for pregnant women with only T. gondii IgG and IgM antibodies respectively. The overall seroprevalence for the study was 83.6% (92/110). The overall seroprevalence of T. gondii IgG and IgM antibodies of 83.6% is higher than the global seroprevalence of 46.1% and 49.7% in the Greater Accra region (Accra) [22,4]. However, the overall seroprevalence of the current study is similar to reported studies, which estimated the seroprevalence of latent T. gondii infection in Europe, Africa and Latin America as 75-90% and 92.5% in the Greater Accra region (Accra) [15,23].
The seroprevalence among the seropositives was observed to be 96.2% (76/79) and 95.3% (41/43) for pregnant women aged between 21 and 40 years for T. gondii IgG and IgM antibodies respectively. The results of the study suggest a general increase in seropositivity with age from between 15 and 20 years to 21 and 30 years for both T. gondii IgG and IgM antibodies. This result is consistent to a study which reported that, distribution of toxoplasmosis increases with age in women of child-bearing age [24,25]. There was however a decrease in seropositivity with age from between 21 and 30 years and between 31 and 40 years for both T. gondii IgG and IgM antibodies.
Conclusion
The study was to determine the seroprevalence of T. gondii infection among pregnant women seeking antenatal care at the Manhyia District Hospital. The study showed an overall seroprevalence of 83.6% among pregnant women. It was also established that 71.8% and 39.1% of the pregnant women had T. gondii IgG and IgM antibodies respectively present in their blood. Moreover, 27.3% of the pregnant women were seropositive for both T. gondii IgG and IgM antibodies. Again, 44.5% of the pregnant women were seropositive for only anti-T. gondii IgG against 11.8% for only anti-T. gondii IgM. Since risk factors for toxoplasmosis was not assessed and discussed for the study, it is recommended a further study to determine the risk factors for toxoplasmosis infection, especially among pregnant women in the Ashanti region be conducted. It is again recommended to policy stakeholders in healthcare delivery that, screening of pregnant women for toxoplasmosis be included in the diagnostic laboratory tests routinely done during antenatal
care.
References
- Ryan KJ, Ray CG (2004) Sherris Medical Microbiology. Medical Microbiology: An Introduction to Infectious Diseases. (4th edn),McGraw Hill, New York, USA. 723-727.
- Török E, Moran E, Cooke F (2013) Oxford Handbook of Infectious Diseases and Microbiology. Oxford University Press, USA. 567-570.
- Jones JL, Kruszon-Moran D, Wilson M (2003) Toxoplasma gondii infection in the United States, 1999-2000. Emerg Infect Dis 9(11): 1-5.
- Ayeh-Kumi PF, Opoku AG, Kwakye Nuako G, Dayie NTKD, Asmah RH, et al. (2010) Seroprevalence of toxoplasmosis among patients visiting the Korle-Bu Teaching Hospital, Accra, Ghana. Reviews in Infect; 1(3): 147-150.
- Montoya JG, Liesenfeld O (2004) Toxoplasmosis. Lancet 363(9425): 1965-1976.
- Dubey JP, Lindsay DS, Lappin MR (2009) Toxoplasmosis and other intestinal Coccidial infections in cats and dogs. Vet Clin North Am Small Anim Pract 39(6):1009–1034.
- Stray-Pedersen B (1993) Toxoplasmosis in pregnancy. Baillieres Clin Obstet Gynaecol 7(1):107–137.
- Garweg JG, Scherrer J, Wallon M, Kodjikian L, Peyron F (2005) Reactivation of ocular toxoplasmosis during pregnancy. BJOG: Int J Obstet Gynecol 112 (2):241–242.
- Liesenfeld O, Press C, Montoya JG, Gill R, Isaac-Renton JL, Hedman K (1997) False-positive results in Immunoglobulin M (IgM) Toxoplasma antibody tests and importance of confirmatory testing: the Platelia Toxo IgM test. J Clin Microbiol 35(1):174–178.
- Jones JL, Lopez A, Wilson M (2003) Congenital toxoplasmosis. Am Fam Physician 67(10): 2131–2138.
- Dunn D, Wallon M, Peyron F, Petersen E, Peckham C, Gilbert R (1999) Mother- to-child transmission of toxoplasmosis: risk estimates for clinical counselling. Lancet 353(9167):1829–1833.
- Baron S (1996) Medical Microbiology. (4th edn), University of Texas Medical, Galveston, Texas, USA.
- Dubey JP, Lindsay DS, Speer CA (1998) Structures of Toxoplasma gondii tachyzoites, bradyzoites and sporozoites and Biology and development of tissue cysts. Clin Microbiol Rev 11(2): 267-299.
- Anteson RK, Sekimoto S, Furukawa S, Takao Y, Nyanotor MA (1978b) Studies on toxoplasmosis in Ghana I. The prevalence of toxoplasmosis as measured by the haemagglutination (Eiken) test. Gh. Med. J 17:147-149
- Ayi I, Edu SAA, Appea-Kubi KA, Boamah D, Bosompem KM, Edoh D (2009) Sero-epidemiology of toxoplasmosis amongst pregnant women in the Greater Accra Region of Ghana. Gh. Med J 43(3): 107-114.
- Kwofie KD (2012) Risk of mother-to-child transmission of Toxoplasma gondii infection among pregnant women in the Greater Accra region. Kwame Nkrumah University of Science and Technology, Kumasi, Ghana. 34-39.
- Zemene E, Yewhalaw D, Abera S, Belay T, Samuel A, et al. (2012) Seroprevalence of Toxoplasma gondii and associated risk factors among pregnant women in Jimma town, Southwestern Ethiopia. BMC Infect Dis12:337.
- Gebremedhin EZ, Abebe AH, Tessema TS, Tullu KD, Medhin G, et al. (2013) Seroepidemiology of Toxoplasma gondii infection in women of childbearing age in Central Ethiopia. BMC Infect Dis 13: 101.
- Akinbami AA, Adewunmi AA, Rabiu KA, Wright KO, Dosunmu AO, et al. (2010) Seroprevalence of Toxoplasma gondii antibodies amongst pregnant women at the Lagos State University Teaching Hospital, Nigeria. Niger Postgrad Med J 17(2): 164—167.
- Selamawit D (2004) Immunology and Serology. Ethiopia Public Health Training Institute (EPHTI). Alemaya University, Ethiopia. 27-46.
- Hill D, Dubey JP (2002) Toxoplasma gondii: Transmission, diagnosis and prevention. Clin Microbiol Infect 8(10): 634–640.
- Jacquier P, Hohlfeld P, Vorkauf H, Zuber P (1995) Epidemiology of toxoplasmosis in Switzerland: national study of seroprevalence monitored in pregnant women 1990-1991. Schwez Med Wochenschr Suppl 65:29-38.
- Partisani M, Candolfi H, DeMautort E, Behencourt S, Lang JM (1991) Seroprevalence of latent Toxoplasma gondii infection in HIV-infected individuals and long-term follow-up of Toxoplasma seronegative subjects. Abstract WP2294. Seventh International Congress on AIDS.
- Nester EW, Anderson DG, Pearsall NN, Nester MT (2004) Microbiology: a human perspective. 4th edition. McGraw Hill, New York, USA. 755-757.
- Garcia JL, Navarro IT, Ogawa L, De Oliverra RC, Kobilika E (1999) Seroprevalence of human toxoplasmosis in rural zone of Jaguapita, Brazil. Rev panamez, Salud publ 6(3):157-163.





