A Systematic Review of Invasive Fungal Infection Treatment With Voriconazole And Caspofungin Among Chinese Population
Feng S1, Long Y2, Tan SC3*, Chen C4
1 Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Science & Peking Union Medical College, Tianjin, China.
2 Peking Union Medical College Hospital, Beijing, China.
3 IMS Health, Asia Pacific, Singapore.
4 IMS Health, Beijing, China.
*Corresponding Author
Seng Chuen Tan,
Health Economics & Outcomes Research, IMS Health Asia Pacific,
8 Cross Street, #21-01/02/03, PWC Building,
Singapore 048424.
E-mail: sctan@sg.imshealth.com
Article Type : Review Article
Received: September 18, 2015; Accepted: October 19, 2015; Published: October 23, 2015
Citation: Feng S, Long Y, Tan SC, Chen C (2015) A Systematic Review of Invasive Fungal Infection Treatment With Voriconazole And Caspofungin Among Chinese Population. Int J Microbiol Adv Immunol. 03(3), 65-69. doi: dx.doi.org/10.19070/2329-9967-1500012
Copyright: Chuen S© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium,provided the original author and source are credited.
Abstract
Background: Voriconazole has been available in China for 10 years. In this time, there has been clinical studies published on the Chinese population.
Objective: This study aimed to conduct a systematic review for both English and Chinese literature on the clinical efficacy and safety of voriconazole versus caspofungin in treating Chinese patients with invasive fungal infection (IFI).
Methods: Both English and Chinese terms of “voriconazole” and “infection” were searched accordingly for clinical studies conducted on populations in China, Taiwan, Hong Kong and Macau in several databases. Identified abstracts were filtered independently by two researchers to select eligible studies. A third researcher was consulted for any disagreement. Jadad scale and modified Newcastle-Ottawa tool were used to assess the study quality of the selected studies.
Results: Two RCTs and 10 retrospective observational studies were included in the systematic review. Conflicting trends were reported on effective treatment rate in the RCTs. 8 observational studies demonstrated that voriconazole had similar or higher effective treatment rate than caspofungin. In terms of mortality, a lower rate was generally observed among patients treated with voriconazole than those who were treated with caspofungin (0 to 26% vs. 14.3 to 50%) in 5 of the 6 studies that reported mortality rates.
Conclusion: The trend of higher effective treatment rates and lower mortality rates of voriconazole compared to caspofungin were observed among Chinese patients with IFI. However, given the small sample size, low study quality, different definitions of efficacy and presence of varied underlying comorbidities in the reviewed studies, the results need to be interpreted with caution.
2.Background
3.Methods
4.Results
4.1 Study Design and Population
4.2 Efficacy
4.3 Safety
5.Quality assessment
6.Discussion
7.Conclusion
9.Conflict of Interest Statement
8.Acknowledgement
10.References
keywords
Invasive Fungal Infection; China; Voriconazole; Caspofungin; Systematic Literature Review.
Background
Invasive fungal infection (IFI) contributes to morbidity and mortality among patients with acute leukemia and patients undergoing allogeneic hematopoietic stem cell transplant (HSCT) [1]. Furthermore, as the infection is caused by a broad spectrum of opportunistic pathogens, IFIs increase rapidly along with the growing immunocompromised population among debilitated and critically ill medical, surgical and intensive care units (ICU) patients with prolonged hospital stays [2]. Aspergillus and Candida are the most frequent molds of IFI among HSCT receipts and also in the critical care setting nosocomial fungal infection [3].
Voriconazole is recommended by the US treatment guidelines as the primary treatment of invasive aspergillosis and candidiasis [4, 5]. According to the guideline, voriconazole shows efficacy for both invasive pulmonary and extrapulmonary aspergillosis [5]. Voriconazole was reported to be the most frequently administered agent and followed by caspofungin in treating IFI patients by physicians in the United States [3].
However, a review of the safety and efficacy of voriconazole among Chinese IFI population has not been undertaken since voriconazole was launched 10 years ago. Therefore, this study aimed to conduct a systematic review of both English and Chinese literature on the clinical efficacy and safety of voriconazole versus caspofungin in treatment of IFI among Chinese population.
Methods
This manuscript adhered to systematic review guidelines published by the Cochrane Collaboration [6] and the UK’s National Institute for Health and Clinical Excellence (NICE) [7]. NICE has a rigorous and clearly specified approach to systematic reviews and the standard is generally considered sufficient by other country heath technology assessment agencies.
The methodology of this study followed the established practice
and comprised a series of core stages:
• Definition of scope and agreement of search terms;
• Implementation of searches and abstract reviews to inform included papers;
• Quality assessment and data extraction.
The scope of search was defined with relevant interventions (voriconazole and caspofungin), population (IFI patients), clinical outcomes measurement (treatment effective rate) and study design (randomized control trial (RCT) and observational study (OS)).
Our searches covered both English and Chinese/Taiwanese databases, i.e. Medline, Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), Wanfang, VIP, Airiti Library and PerioPath. Given that voriconazole was launched in 2005 in China, we restricted our searches to a period from five years before the launch to the date of the current study i.e. from 2000 to November 2014. English terms, “voriconazole”, “infection” and population terms (i.e. “Chinese”, “Taiwanese”, “China”, “Taiwan”, “Hong Kong”, or “Macau”) were searched in title, abstract and key words to identify relevant studies in Medline and Cochrane. Chinese terms of “voriconazole” and “infection ” were employed in the three Chinese databases namely CNKI, Wanfang and VIP. Both Chinese and English search terms were used for Airiti library and Periopath. The language of searched studies was limited to English and Chinese. Given that IFI is a broad disease term that some published studies might be specific to certain fungal infections under IFI, we used the search terms ‘infection’, ‘voriconazole’ and ‘caspofungin’ in order not to miss any relevant studies in our searches. Each abstract identified in the search was reviewed independently by 2 researchers. After irrelevant abstracts were filtered out, full text manuscript was further reviewed to determine the eligibility of a study for inclusion. Editorials notes, comments, letters, case reports, studies not on efficacy and safety of variconazole and caspofugin, such as pharmacokinetics, pathology, epidemiological and economic evaluation, were excluded. Studies investigating voriconazole or caspofungin alone, instead of both of them, were also excluded.
Manuscripts that met the inclusion and exclusion criteria above were retained and reviewed to extract the reported efficacy and safety endpoints for voriconazole and caspofungin respectively. Study identifiers, subject demographics, study design including total sample size, sample size in each arm, length of follow-up and numerical results for each study endpoint were also extracted. A third researcher was involved when there was disagreement in either the abstract filtration or manuscript review phases.
The Jadad scale was employed for assessment of methodological quality of the included RCTs on their study design, proportion of randomization, status and method of double-blinding, and loss of follow-up [8]. The study quality was considered high if the Jadad score was higher than 2; otherwise the study quality was considered low. Modified Newcastle-Ottawa scale was employed for assessing the quality of the included observational studies [9,10]. The assessment covered areas such as the study subject selection and comparability. The original Newcastle-Ottawa scale is a general tool and is neither disease nor treatment specific. We thus modified the scale to be applicable for the clinical studies of IFI.
Results
A total of 12 studies were eligible and included for full-text manuscript review. Among 298 identified articles, 162 duplicates were removed. Another 116 and 8 articles were discarded for different reasons during abstract filtration and full-text manuscript review phases, respectively (Figure 1).
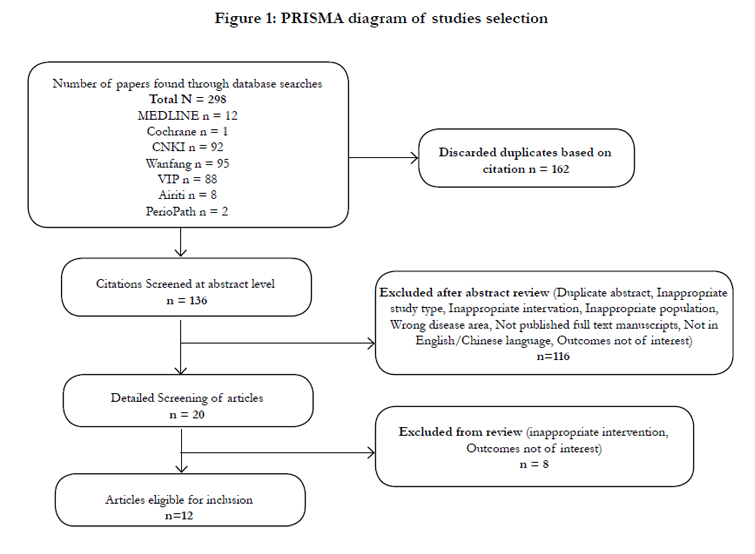
Figure 1: PRISMA diagram of studies selection
Among the 12 identified articles of IFI among Chinese population, 2 were RCTs comparing voriconazole and caspofungin on efficacy and safety. The remaining 10 were observational studies with both voriconazole with caspofungin included as study arms. Table 1 lists the key results from the selected manuscripts.
Efficacy definitions recommended in different local guidance documents were used in 7 of these 12 studies. The definitions stated in the “Clinical Research Guideline of Antibacterial Agents” issued by the Ministry of Health of People’s Republic of China [11] were used in 5 of the studies [12-16] and the 2 studies [13, 14] referred to the definitions recommended in the “Therapeutic Evaluation Standard of Invasive Fungal Disease” issued by Chinese Invasive Fungal Infection Working Group (CIFIWG) [15]. The other 5 studies did not specify clearly the efficacy definitions used [16]. In MoH guidelines, an effective treatment is defined for outcomes ‘cured’ and ‘markedly improvement’. For simplicity of comparison across the studies, we considered outcomes of ‘complete response’ and ‘partial response’ stated in guidance issued by CIFIWG for the definition of an effective treatment in studies that reported these efficacy outcomes.
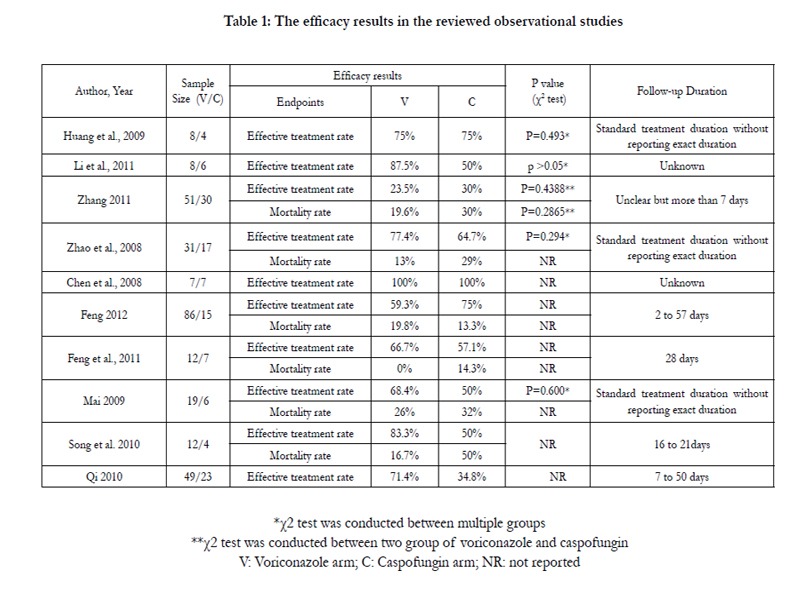

Table 1: The efficacy results in the reviewed observational studies
Study subjects with confirmed IFI diagnosis were investigated in the two RCTs with total sample size of 82 and 200. A follow-up period of 7 days was reported in Fu et al. (2014) [20]. No study duration was mentioned in Wu et al. (2014) [21].
A total of 10 observational studies compared monotherapy of voriconazole with caspofungin among Chinese IFI population. Among the 10 observational studies, a sample size ranging from 30 to 300 patients were reported, comparing the efficacy and safety of voriconazole, caspofungin and other antifungal agents. Three of these studies did not report any dosing or regimen information of the antifungal agents received by the patients [17, 22]. Dosing regimens of some but not all the studied antifungal agents were reported in Mai (2009) [16]. Only 5 studies reported a study duration that ranged from 2 days to greater than 50 days [13, 15, 18, 22]. Although the primary disease of investigation was IFI for these identified studies, study populations in 7 studies were reported to have underlying hematological malignancies including leukemia and multiple myeloma [12-14, 16, 17, 20, 21]. The study populations in the other 5 studies were reported to have other comorbidities including COPD, tumor, diabetes and pulmonary infection. Adult patients were the study subject in all studies except for Song et al., 2010 [13] which investigated the antifungal treatments in children with leukemia [15, 18, 22]. Among all 12 studies, 7 reported pulmonary fungal infection [15, 16, 18, 21] while 3 studies reported mixed infection sites [12-14]. Two studies did not mention any information on the site of infection [17, 20].
Compared to patients treated with caspofungin, a higher effective treatment rate was reported for patients treated voriconazole (90% vs. 80%) in Fu et al (2014) [20]. In contrast, a lower treatment rate was reported in the RCT by Wu et al (2014) [21] for patients treated with voriconazole, although the difference was small (71.4% vs. 74.1%). None of these RCTs reported a mortality rate. The Fu et al (2014) [20] study did not state the definition of ‘effective treatment’ used as the efficacy endpoint.
A higher effective treatment rate was reported for patients treated with voriconazole than caspofungin (66.7 to 87.5% vs. 34.8 to 64.7%) in 6 of the 10 observational studies [13-17,22]. Same rates were reported in two studies (75% vs. 75% and 100% vs. 100%) [12]. Lower rates in 2 studies (23.5% vs. 33.3% and 59.3% vs. 75%) [18].
In terms of mortality, a lower rate was observed among patients treated with voriconazole than those who were treated with caspofungin (0 to 26% vs. 14.3 to 50%) in the studies that reported mortality rates. The exception was Feng et al. (2012), which reported a mortality rate of 19.8% vs. 13.3% for voriconazole and caspofungin, respectively.
Only one RCT reported the proportion of patients who experienced adverse events such as liver function abnormalities, renal or urinary abnormalities and visual hallucination [21]. Lower rates were observed for renal or urinary abnormalities (18% vs. 22%) and visual hallucination (7% vs. 11%) in voriconazole arms compared to caspofungin arms. A total of 7 patients who were treated with voriconazole (n=28) experienced liver function abnormalities, but none was reported for those who were treated with caspofungin (n=27) [21].
Among 10 observational studies, 3 reported overall adverse event rates, ranging from 5% to 21% in voriconazole arms and 3% to 13% in caspofungin arms [15, 18]. All of these 10 studies reported similar key adverse events experienced by the patients. Five studies reported liver function abnormalities (3% to 17%) among patients treated with voriconazole [12, 14-16, 18]. Similar hypokalemia rates of 23% to 26% [12, 14, 16] and visual hallucination rates of 5% to 10% [13, 14, 16] were reported for patients treated with voriconazole across the 3 of the 10 observational studies. None of the three types of adverse events was reported for patients treated with caspofungin. Inconsistent gastrointestinal related adverse event rates were observed (8% vs. 0%; 7% vs. 15%; 16% vs. 17%) for voriconazole arms compared to caspofungin arms in 4 studies [12,14, 16, 18].
Quality assessment
By Jadad scoring standard, both the RCTs were given with a score of 1, indicating poor study quality [20, 21]. There was no or insufficient description of randomization, blinding and dropouts in these two studies. Nor did the studies report withdrawal or dropouts.
Based on the modified Newcastle-Ottawa scale, the average score of the 10 cohort based observational studies was 7. Most of these observational studies (8/10) did not conduct study group comparability assessment. Only 2 studies illustrated or analyzed any possible impact of other factors on the study results of efficacy or safety of treatments [17, 18]. Incomparable study design and unclear or no reporting on loss or withdrawal during follow-up were the main issues found in study quality assessment across a number of studies [12, 15, 22].
Discussion
In the past 10 years, a total of 12 clinical studies have been published investigating the effectiveness of voriconazole and caspofungin in managing IFI among the Chinese population. However, there were only 2 RCT studies and their quality was low based on the Jadad assessment tool. All the remaining identified studies were retrospective of observational studies with fairly good quality, as assessed by modified Newcastle-Ottawa scale.
At present, there is neither a randomized clinical trial nor metaanalysis directly comparing the efficacy of voriconazole to caspofungin in the international medical literature of Pubmed. However, voriconazole was reported to have similar therapy response but lower mortality rate compared with caspofungin in the treatment of invasive aspergillosis for patients with haematological malignancies in a recent retrospective study from USA [17]. Nevertheless, the IFI risk was lower in patients having voriconazole treatment than in patients having caspofungin treatment with respect to IFI prophylaxis in neutropenic patients with haematological malignancies in one mixed treatment comparison study [18].
In clinical practice, patients treated with voriconazole are closely monitored for adverse reactions such as visual disturbance and liver function abnormality. These reactions were commonly reported in clinical studies. However, those side effects were usually mild and transient [19]. Even though the risk elevation of liver enzymes and liver injury were higher in the treatment of voriconazole than caspofungin according to one meta- analysis, the elevation of liver enzymes was reversible and rarely led to discontinuation of voriconazole treatment [20].
Despite equal efficacy assumption was used in a number of economic evaluation analyses comparing voriconazole with caspofungin in invasive fungal infection treatment [21, 22], a trend of higher effective treatment rate was observed in the current review. However, only 5 of the studies reported a p-value or 95% confidence interval for these comparisons and none of them reported statistical significance [12,14, 16-18]. Similarly, a non-significant trend of lower mortality rate was observed among patients treated with voriconazole compared to those treated with caspofungin.
These comparisons should be interpreted with caution as there were a number of limitations of this review. First, the sample size of each study was relatively small and 4 studies had unclear follow-up duration [13, 15, 22]. Secondly, using the Jadad scale, the quality of the RCTs was low. In addition, the rather diverse study populations should be highlighted. Presence of different comorbidities or underlying conditions such as hematological malignancies, COPD, tumor, diabetes, pulmonary infection and etc., were reported in the included studies. Besides the infection sites, most of studies included in this review reported IFI as a single pulmonary lesion while a few claimed multiple infection sites. The use of different efficacy definitions utilized by different entities across these studies was another concern for deriving combined results from these studies. Besides, more studies could have been included in this review if a wider scope e.g. inclusion of studies on other antifungal was considered.
Given the above considerations, further meta-analysis is not recommend due to the small number of studies with each having a relatively small and diverse study sample. Based on our findings in quality assessments of the reviewed studies, we recommend better designed RCTs or observational studies of sufficient sample size to further investigate the efficacy and safety of these two and other antifungal agents in the context of local clinical practice of IFI in China.
Conclusion
A trend of higher effective treatment rates and lower mortality rates were observed for voriconazole compared to caspofungin in published clinical studies on Chinese patients with IFI. This result needs to be interpreted with caution, due to inconsistencies in sample demographics, efficacy definitions, reporting of results and small sample size.
Conflict of Interest Statement
Seng Chuen Tan and Can Chen are current employees of IMS Health which has received fund from Pfizer China for this study. All the other authors declare that they have no competing interests.
Acknowledgement
Funding of this study was provided by Pfizer China, and supported by Grants from the National Key Technology Support Program of China (2013BAIO1BO9) and the Key Program of Applied basic Research Foundation of Tianjin (14JCZDJC33000).
References
- Segal BH, Almyroudis NG, Battiwalla M, Herbrecht R, Perfect JR, et al. (2007) Prevention and early treatment of invasive fungal infection in patients with cancer and neutropenia and in stem cell transplant recipients in the era of newer broad-spectrum antifungal agents and diagnostic adjuncts. Clin Infect Dis 44(3): 402-409.
- Delaloye J, Calandra T (2014) Invasive candidiasis as a cause of sepsis in the critically ill patient. Virulence 5(1): 161-169.
- Neofytos D, Horn D, Anaissie E, Steinbach W, Olyaei A, et al. (2009) Epidemiology and outcome of invasive fungal infection in adult hematopoietic stem cell transplant recipients: analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance registry. Clin Infect Dis 48(3): 265-273.
- Pappas PG, Kauffman CA, Andes D, Benjamin DK Jr, Calandra TF, et al. (2009) Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 48(5): 503-535.
- Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, et al. (2008) Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis 46(3): 327-360.
- Higgins JP, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]: The Cochrane Collaboration.
- National Institute for Health and Care Excellence (2013) NICE guide to the methods of technology appraisal.
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, et al. (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1): 1-12.
- Deeks JJ, Dinnes J, D'Amico R, Sowden AJ, Sakarovitch C, et al. (2003) Evaluating non-randomised intervention studies. Health Technol Assess 7(27): iii-x, 1-173.
- Higgins JP, Green S (2008) Cochrane handbook for systematic reviews of interventions (Vol. 5). Wiley-Blackwell, Chichester, England.
- Ministry of Health of People's Republic of China (1987) Clinical Research Guideline of Antibacterial Agents [Chinese]. Chin J Clin Pharmacol 3(2): 126-130.
- Huang BH, Li J, Liu JR, Gu JL (2009) The clinical features and risk factors for invasive fungal infection in multiple myeloma. China J Intern Med 48(12): 1026-1030.
- Li Y, Gao L, Wang LL, Wang QS, Li HH, et al. (2011) Clinical Characteristics and Efficacy of anti-Aspergillus Therapy in Patients with Hematological Malignancies and Invasive Aspergillosis. J Exp Hematol 19(5): 1289-1293.
- Zhang F (2011) A retrospective analysis of effect of voriconazole and caspofungin on invasive pulmonary aspergillosis. Shandong University, Master Thesis.
- Chinese invasive fungal infection work group (CIFIWG) (2010) Diagnostic criteria and treatment principles for patients of blood disease/ malignant tumors with invasive fungal infection (the third revision). China J Intern Med 49(5): 451-454.
- Fu L, Zhang T, Liu JM, Zheng YR (2014) Clinical analysis of malignant blood disease patients complicated with invasive fungal infections. China Tropical Medicine 14(2): 204-206.
- Raad II, Zakhem AE, Helou GE, Jiang Y, Kontoyiannis DP, et al. (2015) Clinical experience of the use of voriconazole, caspofungin or the combination in primary and salvage therapy of invasive aspergillosis in haematological malignancies. Int J Antimicrob Agents 45(3): 283-288.
- Pechlivanoglou P, Le HH, Daenen S, Snowden JA, Postma MJ (2014) Mixed treatment comparison of prophylaxis against invasive fungal infections in neutropenic patients receiving therapy for haematological malignancies: a systematic review. J Antimicrob Chemother 69(1): 1-11.
- Traunmüller F, Popovic M, Konz KH, Smolle-Jüttner FM, Joukhadar C (2011) Efficacy and safety of current drug therapies for invasive aspergillosis. Pharmacology 88(3-4): 213-224.
- Herbrecht R (2004) Voriconazole: therapeutic review of a new azole antifungal. Expert Rev Anti Infect Ther 2(4): 485-497.
- Domínguez-Gil A, Martín I, García Vargas M, Del Castillo A, Díaz S, et al. (2007) Economic evaluation of voriconazole versus caspofungin for the treatment of invasive aspergillosis in Spain. Clin Drug Investig 27(3): 197-205.
- Selleslag D, Vogelaers D, Marbaix S (2009) Economic evaluation of voriconazole versus caspofungin for the treatment of invasive aspergillosis in Belgium. Acta Clin Belg 64(5): 393-398.





