Relationship between Presarcopenia and Trabecular Bone Score in HIV - Infected People
Briongos-Figuero LS1*, Palacios-Martín T1, Bachiller-Luque P1, de Luis D2, Pérez-Castrillón JL2
1 Internal Medicine Service, Rio Hortega University Hospital, Valladolid, Spain.
2 Endocrinology and Nutrition Service, University Hospital of Valladolid, Valladolid, Spain.
*Corresponding Author
Laisa Socorro Briongos-Figuero, MD, PhD
Internal Medicine Service, Rio Hortega University Hospital,
C/Dulzaina 2, 47012 Valladolid, Spain.
Tel: 0034983420400
E-mail: laisadoc@hotmail.com
Received: June 29, 2016; Accepted: August 02, 2016; Published: August 06, 2016
Citation: Briongos-Figuero LS, Palacios-Martín T, Bachiller-Luque P, de Luis D, Pérez-Castrillón JL (2016) Relationship between Presarcopenia and Trabecular Bone Score in HIV -Infected People. Int J AIDS Res. 3(6), 87-90.DOI : dx.doi.org/10.19070/2379-1586-1600018
Copyright: Briongos-Figuero LS© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: Antiretroviral therapy (ART) has transformed HIV-infection to a chronic disease. Nonetheless, since ART does not fully restore immune health, patients develop inflammation-associated complications considered the cornerstone in HIV-infection management. Osteoporosis is an important cause of morbidity in HIV-infected population and presarcopenia has emerged as important risk factor for osteoporosis. Trabecular bone score (TBS) is a novel method to evaluate bone microarchitecture. Our goal was to determine relationship between presarcopenia, osteoporosis and TBS in HIV- infected people.
Methods: We designed a case-control study including 32 HIV-outpatients satisfying eligibility and exclusion criteria and 16 healthy-controls from local “TBS healthy-cohort”. Densitometry studies were using a dual-energy X-ray absorptiometry (DXA). TBS was evaluated at DXA lumbar spine image using TBSiNsight®v2.1. Skeletal muscle mass index (SMI) was defined as (appendicular skeletal muscle mass)/height² (kg/m²). Presarcopenia was established as SMI <7.26 kg/m² for men and SMI <5.55 kg/m² for women.
Results: Presarcopenia prevalence was 31% and osteoporosis 12.5% in cases. HIV-cases have more prevalence of low TBS (44% vs 12.5%, p=0.031). Regarding HIV-infected group, poor correlation was found between TBS and presarcopenia (r:-0.174, p=0.342). Nevertheless, strong correlation was observed between TBS and lumbar spine bone mineral density (BMD) (r:0.590, p=0.001), and good correlations between TBS and femoral neck BMD (r:0.395, p=0.025) and TBS and total hip (r:0.365, p=0.040).
Conclusions: This is the first study that evaluates presarcopenia and TBS relationship in HIV-positive people and strong correlations between TBS and BMD were found in our population. Even so, further researches are needed to analyze this association.
2.Introduction
3.Methods
3.1 Selection of study participants
3.2 Measures
3.3 Ethics approval of research
3.4 Data Analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Sarcopenia; HIV; Bone Mineral Density; Muscle Mass; Fracture Risk.
Introduction
Life expectancy of HIV-infected people has increased markedly since the use of effective, potent antiretroviral therapy (ART). For now, many people are living longer and healthy live with HIV. But growing older with HIV also has an impact on developing an increasing number of noninfectious HIV-related comorbidities. Bone is one of the organs affected by HIV infection, such that a three-time greater prevalence of osteoporosis has been observed in the HIV-positive population compared with HIV-seronegative people independently of age and gender [1]. Multiple factors appear to be involved in bone loss, fracture risk and frailty in HIVinfected patients, including physical inactivity, low body weight, ART side effects, chronic T-cell immune activation and subsequent accelerated cellular senescence and HIV viral proteins itself [2-5]. T-cell activation have been associated with high production of receptor activator of nuclear factor-kappa-β ligand (RANKL) and pro-inflammatory cytokines, which promote osteoclast activity and bone turnover [2, 3, 6, 7].
Sarcopenia, defined as the loss of muscle mass and function associated with aging, and presarcopenia, characterized only by age-related low muscle mass, have emerged as an important risk factor for osteoporosis [8-12]. Both are considered to be major factors for functional limitations and motor dependency.
In addition, sarcopenia might also decrease bone strength by reducing mechanical loading to the skeleton. Dual-energy X-ray absorptiometry (DXA) is the preferred method to estimate muscle mass for research and clinical use [12].
Trabecular bone score (TBS) is a novel method to evaluate bone microarchitectural texture and predict fracture risk from the lumbar spine DXA image without the need for further imaging on expensive instrumentation [13].
Despite long-term survival in HIV-infected people and development of non-HIV associated comorbidities, little is known about some ageing associated issues that affect health in this population. In particular, the disorders that lead to abnormalities in bone metabolism and lean mass remain unclear. To our knowledge, no data are available on clinical utility of TBS in HIV-positive population. The aim of this study was to analyze the relationship among presarcopenia, bone health and trabecular bone score in HIV-infected people.
Methods
We conducted a case-control study between January and June 2015 at a tertiary referral hospital in Valladolid, Spain. Cases eligibility criteria were: 1/HIV-1 infected subject aged 30-60 years, receiving stable ART treatment and overfollow-up at our outpatient clinic; 2/undetectable (<20 copies/mL) HIV-1 RNA by quantitative method for at least 24 months with no more than 2 isolated “blips” (intermittent episodes of detectable low-level RNA viremia<400 copies/mL; 3/free of lipodystrophysyndrome and diabetes mellitus. Exclusion criteria included cancer,chronic febrileillness, acute medical disease, skeletal diseases or myopathies, kidney failure, digestive disorders (diarrhea for > 30 days or > three times/day), liver damage, prolonged immobilization and active bone therapies.
Sociodemographic and clinical information was obtained from digitalized medical records and included: age, sex, CD4 lymphocyte level (determined by flow cytometry using FACS Calibur (Becton-Dickinson, Frankin Lakes, New Jersey, USA)), viral load (determined by polymerase chain reaction-PCR-using the Ul trasensible Cobas-Amplicor (Roche, Pleasanton, California, USA)) and biochemical parameters in fasting conditions: total serum calcium (range 8-10 mg/dL), total serum phosphorus (range 3-4 mg/dL) and basal alkaline phosphataselevel (reference range 30-120 U/L).Body mass index (BMI) was calculated as total body weight in kg/height in m².
We enrolled 32 consecutive HIV- infected outpatients under follow-up at our hospital. Controls were 16 healthy volunteer people included inour local “TBS healthy cohort”, matched with case patients by age and sex with a 1:2 ratio.
Densitometry studies were conducted in all, case and control patients, in the lumbar spine (L1-L4), total hip, femoral neck and whole body using a dual-energy X-ray absorptiometry (DXA) (Prodigy, Primo 8.0, GE-Lunar, General Electric Healthcare,Madison, WI, USA). Bone mineral density (BMD) was expressedin g/cm2. T-score and Z-score were evaluated at lumbar spine,total hipand femoral neck. Osteoporosis was defined as T-score at the hip or spine ≤ 2.5 standard deviations meeting the WHO criteria [14].
TBS is an indirect textural index that evaluates pixel gray-level variations in the lumbar spine DXA images and estimates trabecular bone microarchitecture by the projection of the 3D structure onto a 2D plane [15]. TSB also predicts osteoporotic fractures independent of BMD and major clinical risk factors [13]. TBS was evaluated at the DXA lumbar spine (L1-L4) image using TBSiNsight®v2.1 (Med-Imaps, Merignac, France). We used the cutoff points for TBS values established by a working group [16] as follow: TBS ≥1.350 is considered to be normal; TBS between 1.200 and 1.350 is considered to be consistent with partially degraded microarchitecture; and TBS ≤1.200 (low TBS) defined degraded microarchitecture.
According to the European Working Group on Sarcopenia in Older People (EWGSOP) criteria, sarcopenia can be classified into three stages: presarcopenia (characterized bylow muscle mass without impact on muscle strength orphysical performance), sarcopenia (characterized by low muscle mass, plus low muscle strengthor low physical performance) and severe sarcopenia (identified when low muscle mass, low muscle strength and low physical performance are met) [12]. Presarcopenia stage can only be identified by techniques that measure muscle mass accurately and in reference to standard populations so, also, a whole-body DXA scan was performed to measure total lean mass, lean mass of arms and legs and fat mass (enCORE 2005, clinical software, General Electric Healthcare, Madison, WI, USA). Appendicular skeletal muscle mass (ASM) (kg) was determined by the sum of the four lean masslimbs from a DXA and skeletal muscle mass index (SMI) was defined as ASM/height2 (kg/m²). Presarcopenia cutoff points were established by gender as SMI <7.26 kg/m² for men and SMI <5.55 kg/m² for women [12, 17].
All measures were carried out by the same technician.
All procedures in this study were approved by the hospital’s Ethics Committee, and patients signed an informed Medical Consent Form to participate according to the principles of the Declaration of Helsinki. The privacy and confidentiality of the data collected was ensured.
Data were analyzed using the SPSS 19.0 (SPSS Inc®, Chicago, IL, USA) statistical package. A descriptive profile analysis was performed on the sample and expressed as mean ± standard deviation, frequencies and percentages. The distribution of variables was analyzed using the Kolmogorov-Smirnov test. Subsequently, the association between variables was studied using a Chi-square test with Fisher’s exact test and Student’s t-test with Bonferroni’s adjustment. Relationships between TBS and presarcopenia and TBS and BMD and were determined using the Pearson correlation (r) coefficient. Level of statistical significance was established as p ≤ 0.05.
Results
We included 32 HIV-patients, of whom 24 were men and 8 were women, and 16 healthy controls (12 men and 4 women). Case group mean age was 45 ± 10 with no differences compared to control group (mean age 46 ± 8, p=0.729). Concerning to the infection situation, mean CD4 lymphocyte level was 574 ± 270 cell/μL and HIV-1 viral load was undetectable in all of them. When analyzing biochemical parameters, mean calcium level was 9.2 ± 0.3 mg/dL, mean phosphorus level was 3.2 ± 0.7 mg/dL and mean alkaline phosphatase level was 92 ± 32 U/L.
No significant differences were found between cases and control (23.4 ± 4.5 vs 22.5 ± 2.3, p=0.457)in BMI. DXA finding related to BMD, osteoporosis and TBS and their relationship with HIV infection are shown in Table 1.
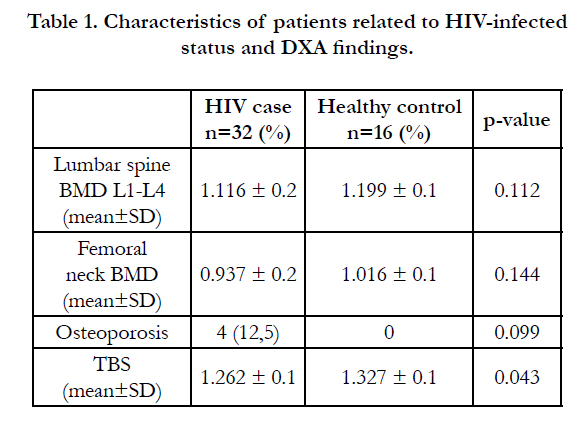

Table 1.Characteristics of patients related to HIV-infected status and DXA findings
We found presarcopenia in 31% of cases and osteoporosis in 12.5%. HIV-infected people have a significant more prevalence of low TBS than controls (44% vs 12.5%, p=0.031). Respecting HIV-infected people group, poor correlations were found between TBS and presarcopenia (r: -0.174, p=0.342) and also between presarcopenia and BMD findings (lumbar spine L1-L4, r: -0.053, p=0.772; femoral neck, r: -0.078, p=0.670; total hip, r: -0.085, p=0.644). On the other hand, strong correlation was observed between TBS and lumbar spine L1-L4 BMD (r: 0.590, p=0.001), and good correlations were found between TBS and femoral neck BMD (r: 0.395, p=0.025) and also TBS and total hip (r: 0.365, p=0.040).
Discussion
In the ART era, most patients achieve a most likely lifelong virologic suppression. Growth of the aging HIV-positive people has interfered with of non-HIV associated comorbidities management.
Osteoporosis and sarcopenia are principal components of frailty syndrome and the responsible for functional impairment and increase morbidity and mortality [8-10]. The direct cost attributed to sarcopenia in 2000 was 1.5% of health care expenditure en USA and it is estimated a 10% decrease in its prevalence would save 1.1 billion $ in health-related cost [18].
We found a high prevalence of presarcopenia (31%), greater than data from studies conducted in both general population [8]. In a recent study, Wasserman et al., [19] reported a presarcopenia prevalence of 20% in HIV-infected persons significantly associated to male gender, recreational psychoactive substance use and intravenous drug use HIV transmission category. We also found a high prevalence of TBS<1.200 (44%), never reported before in HIV-infected people.
There are few data in literature regarding presarcopenia and BMD and present study is the first one evaluating presarcopenia and TBS relationship in HIV-positive population as associated conditions. Verschueren et al., [11] found that being diagnosed with presarcopenia in general population are more likely to have a higher risk of osteoporosis. Our results do not confirm this finding in HIV-infected population.
Our study has several limitations. The small sample size did not allow excluding new unknown relationships. We identified some associations but could not infer temporal relationship. These results require further research and follow up with a larger number of patients along both groups. A specific design is need to evaluated influence of individual ART regimens, sex ratio, tobacco and alcohol use and vitamin D levels on presarcopenia and TBS, since changes in this issues have been related to BMD and limb fat mass [7, 20, 21].
This preliminary study has important strengths. First, we include a healthy paired control group so findings on TBS and precarcopenia effects in HIV infected peopleare supported by the design. Second, to our knowledge, this is the first study focused on presarcopenia in HIV-infected patients and the clinical use of TBS in this population to evaluate fracture risk. This study demonstrates, we believe, the importance of applying new techniques, like TBS, and assessment new concepts, like presarcopenia, in HIV-positive people.
Conclusion
In the present study perform on HIV-infected adults with a durably virologic suppression, we have found more prevalence of abnormalities at the trabecular bone microarchitecture measured by TBS so this technique could be useful to predict fracture risk in HIV-infected population. Contrary to our expectations we could not demonstrate an existing relationship between TBS and muscle mass expressed as presarcopenia. On the other hand, significant correlations between TBS and BMD in several locations were found in our population. Longitudinal researches are needed to determine the impact of low lean muscle mass in aging HIV-infected people in order to adopt appropriate preventive interventions.
References
- Brown T T, Qaqish R B. (2006) Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS 20(17): 2165- 2174 .doi:10.1097/QAD.0b013e32801022eb.
- Castronuovo D, Cacopardo B, Pinzone, MR, Di Rosa M, Martellotta, et al., (2013) Bone disease in the setting of HIV infection: update and review of the literature. Eur Rev Med Pharmacol Sci, 17(18): 2413-2419.
- Güerri-Fernández R, Villar-García J, Díez-Pérez A, Prieto-Alhambra D (2014) HIV infection, bone metabolism, and fractures. Arq Bras Endocrinol Metabol. 58(5): 478-483.
- Rothman MS, Bessesen MT (2012) HIV infection and osteoporosis: patho physiology, diagnosis, and treatment options. Curr Osteoporos Rep, 10(4): 270-277, doi:10.1007/s11914-012-0125-0.
- Deeks SG (2011) HIV infection, inflammation, immunosenescence, and aging. Annu Rev Med, 62: 141-55, doi:10.1146/annurevmed- 042909-093756.
- de Luis D A, Bachiller P, Palacios T, Conde R, Izaola O, et al (2012) Relationship of fat distribution with adipokines in patients with acquired immunodeficiency virus infection. J Clin Lab Anal, 26(5): 336-341, doi:10.1002/jcla.21528.
- Natsag J, Kendall MA, Sellmeyer DE, McComsey GA, Brown TT (2015). Vitamin D, osteoprotegerin/receptor activator of nuclear factor-kappaB ligand (OPG/RANKL) and inflammation with alendronate treatment in HIV-infected patients with reduced bone mineral density. HIV Med, 17(3):196-205, doi:10.1111/hiv.12291.
- Pereira FB, Leite AF, de Paula AP (2015). Relationship between pre-sarcopenia, sarcopenia and bone mineral density in elderly men. Arch Endocrinol Metab. 59(1): 59-65. doi:10.1590/2359-3997000000011.
- Tarantino U, Baldi J, Celi M, Rao C, Liuni FM, et al., (2013) Osteoporosis and sarcopenia: the connections. Aging Clin Exp Res, 25 Suppl 1: S93-5, doi:10.1007/s40520-013-0097-7.
- Ali S, Garcia JM. (2014) Sarcopenia, cachexia and aging: diagnosis, mechanisms and therapeutic options - a mini-review. Gerontology, 60(4): 294-305, doi:10.1159/000356760.
- Verschueren S, Gielen E, O'Neill T W, Pye S R, Adams J E, et al. (2013). Sarcopenia and its relationship with bone mineral density in middle-aged and elderly European men. Osteoporos Int, 24(1): 87-98, doi:10.1007/s00198-012-2057-z.
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, et al., (2010) Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing, 39(4): 412-423, doi:10.1093/ageing/afq034.
- Silva BC, Leslie WD, Resch H, Lamy O, Lesnyak O, et al., (2014). Trabecular bone score: a noninvasive analytical method based upon the DXA image. J Bone Miner Res, 29(3): 518-530, doi:10.1002/jbmr.2176.
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group (1994). World Health Organ Tech Rep Ser, 843, 1-129.
- Bousson V, Bergot C, Sutter B, Levitz P, Cortet B, et al., (2012) Trabecular bone score (TBS): available knowledge, clinical relevance, and future prospects. Osteoporos Int. 23(5): 1489-1501, doi:10.1007/s00198-011-1824-6.
- Cormier C, Lamy O, Poriau S. TBS in routine clinial practice: proposals of use [Internet]. Plan-les-Outes, Switzerland: Medimaps Group; 2012., Available from: www.medimapsgroup.com/upload/MEDIMAPSUK-WEB.pdf.
- Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, et al., (1998) Epidemiology of sarcopenia among the elderly in New Mexico.Am J Epidemiol, 147(8): 755-763.
- Janssen I, Shepard D S, Katzmarzyk P T, Roubenoff R (2004) The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc, 52(1): 80-85.
- Wasserman P, Segal-Maurer S, Rubin DS (2014) High prevalence of low skeletal muscle mass associated with male gender in midlife and older HIVinfected persons despite CD4 cell reconstitution and viral suppression. J Int Assoc Provid AIDS Care, 13(2): 145-152, doi:10.1177/2325957413495919.
- Brown TT, Moser C, Currier JS, Ribaudo H J, Rothenberg J, et al. (2015). Changes in Bone Mineral Density After Initiation of Antiretroviral Treatment With Tenofovir Disoproxil Fumarate/Emtricitabine Plus Atazanavir/Ritonavir, Darunavir/Ritonavir, or Raltegravir. J Infect Dis, 212(8): 1241-1249, doi:10.1093/infdis/jiv194.
- Rojas J, Lonca M, Imaz A, Estrada V, Asensi V, et al., (2015). Improvement of lipoatrophy by switching from efavirenz to lopinavir/ritonavir. HIV Med, 17(5):340-349. doi:10.1111/hiv.12314.





