Acridine Orange Fluroscence Study of Lung - Histopathology in Autopsy Cases of Burns
Bhanvadia VM1*, Bhetariya BV2, Desai NJ3, BD Gupta4, Patel PN5
1 Assistant Professor, Department of Pathology, Shree M.P. Shah Government Medical College, Jamnagar, Gujarat, India.
2 Associate Professor, Department of Pathology, Shree M.P. Shah Government Medical College, Jamnagar, Gujarat, India.
3 Professor, Department of Pathology, Shree M.P. Shah Government Medical College, Jamnagar, Gujarat, India.
4 Professor and Head, Department of Forensic Medicine, R.D. Gardi Medical College, Surasa, Ujjain, M.P., India.
5 Fellow in Oncopathology, Gujarat Cancer and Research Institute, Ahmedabad, Gujarat, India.
*Corresponding Author
Dr. Viral M. Bhanvadia M.D. (Path),
Assistant Professor, Department of Pathology,
Shree M.P. Shah Government Medical College,
Jamnagar, 361008, Gujarat, India.
Tel: 09998879644
Email: drviral2001@gmail.com
Received: April 16, 2017; Accepted: May 25, 2017; Published: May 31, 2017
Citation: Bhanvadia VM, Bhetariya BV, Desai NJ, BD Gupta, Patel PN (2017) Acridine Orange Fluroscence Study of Lung-Histopathology in Autopsy Cases of Burns. Int J Forensic Sci Pathol. 5(2), 331-336. doi: http://dx.doi.org/10.19070/2332-287X-1700073
Copyright: Bhanvadia VM© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The major cause of death in the burn patients includes multiple organ failure and septicemia but, sometimes the exact cause of death in many fatally burn patients is difficult to detect.
Aim: The aim was to study various histopathological changes in lung in the post-mortem cases of burns, by using routine Haematoxylin and Eosin stain (H&E stain).
Periodic and Schiff ’s Stain (PAS) stain to study the role of acridine orange fluorescence study, to explore the forensic utility of this study and to find out the relationship between duration of survival and histopathological changes observed.
Material & Methods: Total 32 cases of death due to burns were autopsied at mortuary from october 2010 to september 2012, department of Forensic Medicine and Toxicology in our hospital. These were forwarded to Department of Pathology for histopathological examination.
Result: In the present study, maximum number of burns cases in 21-30 years of age group & female predominance. Grossly, 19 cases (59.38%) showed congestion while microscopy showed diffuse alveolar damage (34.38%). The sections stained by acridine orange and observed under fluorescent microscope were negative in 28 cases (87.50%) and lightly positive in 04 cases (12.50%).
Conclusion: Routine microscopy does help us in getting specific lesions in lung due to burns. But PAS and Acridine orange fluorescence do not add anything further in our knowledge of pathology due to burns. However, none of these add any new tool to resolve any forensic issues of burns. Therefore, microscopy (including PAS and fluorescent), if done would be redundant.
2.Introduction
3.Material and Methods
3.1. Method of Stain in Acridine Orange [7]
3.2.Interpretation
4.Results
5.Discussion
6.Conclusion
7.Acknowledgement
8.References
Keywords
Acridine Orange; Fluorescence Study; Diffuse Alveolar Damage; PAS Stain.
Introduction
Burn is an injury which is caused by application of heat or chemical substances to the external or internal surfaces of the body causing destruction of tissues [1].
Every year more than 2 million people sustain burns in India; most of them (around 500,000 people) are treated as outdoor patients. About 2,00,000 are admitted in hospitals while 5,000 of them die [2]. In most of the cases to get the medical cause of death is not difficult. Victims commonly die immediately of hypovolemic shock and due to septicemia or multiple organ failures, if deaths are delayed by few days to few weeks [3].
In modern era, commonly a big hue and cry in media (Print & Electronics) is made over such deaths and their investigations. This puts immense pressure on workers including autopsy surgeons. There are instances that post mortem reports in such cases are referred to second to multiple opinions. In some cases even a second autopsy is being performed because of this hue and cry. There are suggestions by various forensic experts, albeit defensive, to study targeted organs histopathology. However, there are studies contrary to their suggestions [4, 5].
Pulmonary pathologic abnormalities occur in 30-80% of deaths from burn injury [6]. Pulmonary disease exists in several forms, including acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Acute lung injury(ALI)/Acute respiratory distress syndrome (ARDS) is initiated by injury of pneumocytes and pulmonary endothelium, setting in motion a viscous cycle of increasing inflammation, pulmonary vascular permeability, edema, epithelial cell death and pulmonary damage.
Present study is an effort to identify the histopathological changes occurring in the lungs of burn deaths with the help of routine H&E stain and special stains like PAS and acridine orange fluorescence dyes to find relationship between duration of survival and various histopathological changes observed in lung due to burns. As there are only few studies conducted in this regard till now, it will be of immense help for further research in this field. Also, to know whether such studies would help in deciding medicolegal nature of cases.
Material and Methods
An prospective longitudinal study was conducted on 32 cases of burns obtained from autopsies conducted by the Department of Forensic Medicine in M.P. Shah Government Medical College & GG Government Hospital, Jamnagar, a district, located in the western part of Gujarat, a state in India, from October 2010 to September 2012. Jamnagar, All suicidal, homicidal and accidental cases of burns in the all age group were included. Cases of electrocution, radiological injuries and where the bodies were decomposed, were excluded. Clinical case records of the deceased were reviewed in all cases before autopsies were undertaken.
After opening the thoracic and abdominal cavities during autopsy procedure, both lungs were removed and fixed in 10% neutral buffered formalin solution. Lungs were examined grossly and representative sections were taken. Routine microscopic examination by hematoxylin & eosin (H&E) as well as Periodic acid Schiff (PAS) stain and fluorescence study by acridine orange stain were done in all cases. As a control of PAS stain, section from appendix was taken whereas for the control purpose of fluorescence study, a paraffin section from a case of acute myocardial infarction was taken which was showing changes of MI grossly as well as microscopically in H&E stain.
1) 1% solution of Acridine orange was prepared by dissolving 1g of the powder in 100 ml phosphate buffer of pH7.0; 2) Paraffin embedded sections were brought to water; 3) Staining with acridine orange solution is effected for 3-5 seconds, the slides being continuously adjusted during this time to avoid non-specific deposition of acridine orange; 4) The stained sectioned are repeatedly rinsed in phosphate buffer for 10-15 minutes using 2-3 changes of buffer solution. To wash away of non-specific deposits of acridine orange; At the end of the staining, the sections attained moderately dark brown colour visible to the naked eye. 5) The sections were then mounted in buffer solution and viewed under Ultra Violet fluorescent microscope immediately.
Examination under fluorescent microscope using low power magnification revealed necrosed tissue by its grass green colour. The intensity of green colour is directly proportional to the severity of damage.
Results
In the present study, wide age range was observed from 11 to 90 years. Maximum number of cases were in the age group of 21 to 30 years (31.25%) followed by age groups of 11 to 20 years (28.12%) and 31 to 40 years (21.87%). Out of 32 cases, 28 (87.50%) were females and only 4 (12.50%) were males. In 21 to 30 years age group, 80% were female and 20% were males. In 11 to 20 years age group, all (100%) were female.
It was observed that 9 cases (28.13 %) could not survive for more than 12 hours, whereas 6 cases (18.75 %) of the victims died between 4 to 5 days after the burns incident [Table-1].
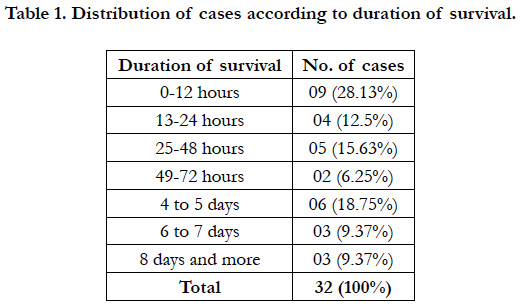

Table 1. Distribution of cases according to duration of survival.
Cases showed burns varying from 41 % to 100 %. Sparing one, rest of the cases showed more than 50% area involvement. Out of total 32 cases, 31 had dermo-epidermal burns (96.87%) and the only remaining one case had deep burns (3.13%).
In majority of cases, cause of death was septicaemia (37.50%) followed by hypovolemic shock (31.25%) and acute renal failure (21.88%), while in only three cases cause of death was neurogenic shock (9.37%) [Table-2].
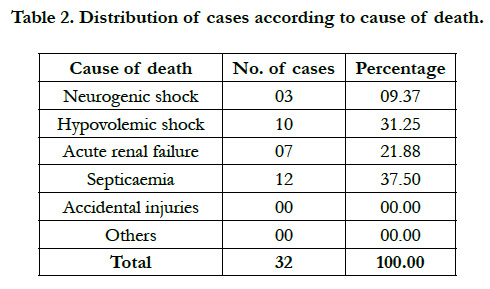
Table 2. Distribution of cases according to cause of death.
On gross examination of lung, 19 cases (59.38%) showed congestion, 7 cases (21.87%) showed consolidation, 6 cases (18.75%) showed heavy & markedly congested lungs with frothy fluid on cut section (edematous changes) were observed [Figure 1].
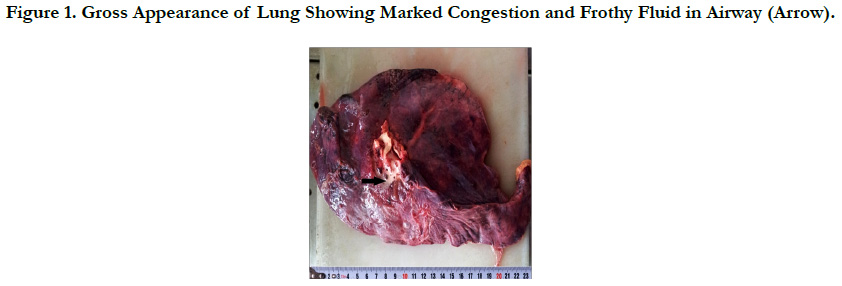
Figure 1. Gross Appearance of Lung Showing Marked Congestion and Frothy Fluid in Airway (Arrow).
On microscopic examination of lung, Predominant histopathological changes were of diffuse alveolar damage (34.38%) followed by interstitial pneumonitis (25%), bronchopneumonia (21.87%) & pulmonary edema (18.75%) [Figure - 2, 3, 4, 5].
All above observed histopathological features were correlated with duration of survival and it was observed that all cases showing changes of pulmonary edema had minimum duration of survival (0-12 hours) whereas cases showing changes of bronchopneumonia had maximum duration of survival (4 days or more). Cases showing changes of diffuse alveolar damage and interstitial pneumonitis were distributed widely in correlation with duration of survival from 0-12 hours to 6-7 days [Table-3].
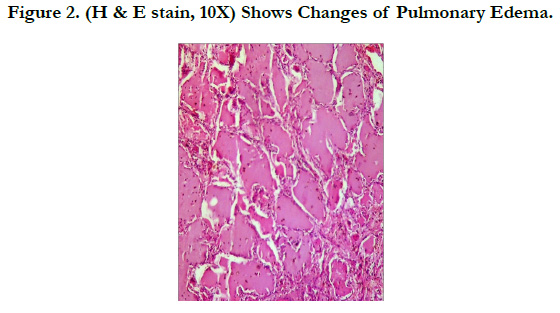
Figure 2. (H & E stain, 10X) Shows Changes of Pulmonary Edema.
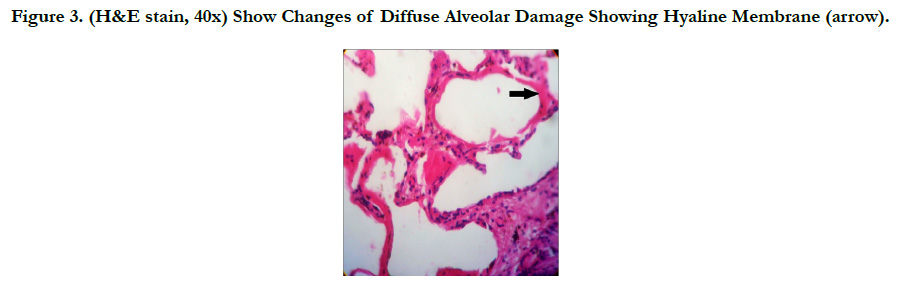
Figure 3. (H&E stain, 40x) Show Changes of Diffuse Alveolar Damage Showing Hyaline Membrane (arrow).
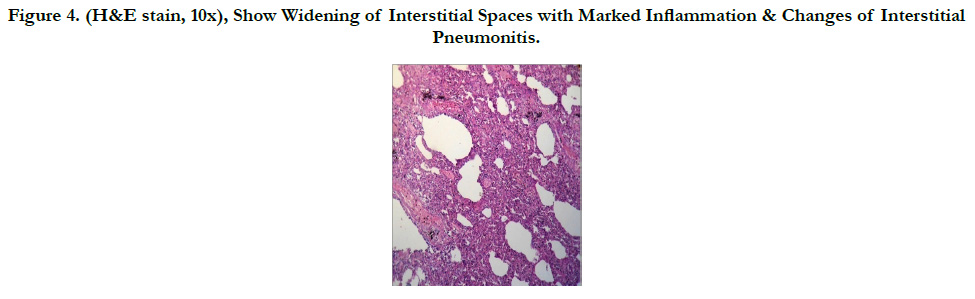
Figure 4. (H&E stain, 10x), Show Widening of Interstitial Spaces with Marked Inflammation & Changes of Interstitial Pneumonitis.
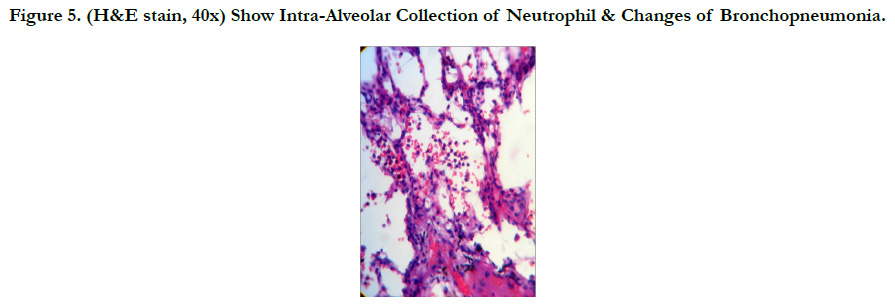
Figure 5. (H&E stain, 40x) Show Intra-Alveolar Collection of Neutrophil & Changes of Bronchopneumonia.
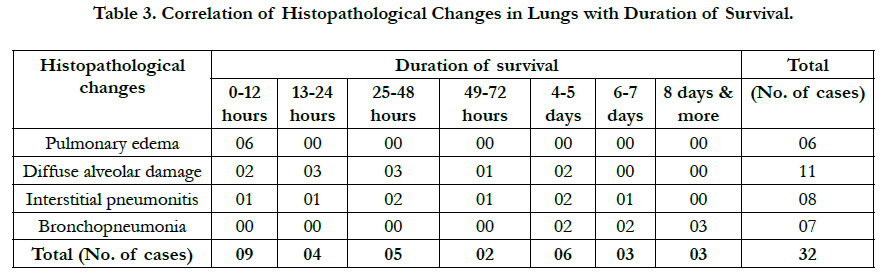
Table 3. Correlation of Histopathological Changes in Lungs with Duration of Survival.
It was observed that sections taken from lungs stained by PAS stain were negative in 21 cases (65.63%) and positive in 11 cases (34.37%) showing PAS +ve hyaline membrane formed due to diffuse alveolar damage [Table- 4].
It was observed that sections taken from lungs stained by acridine orange stain and observed under fluorescent microscope were negative in 28 cases (87.50%) and lightly positive in 04 cases (12.50%) [Table-5] [Figure 6]. Results were comparable to control slide of acridine orange stain of early and late myocardial infarct under fluorescent microscope [Figure 7, 8].
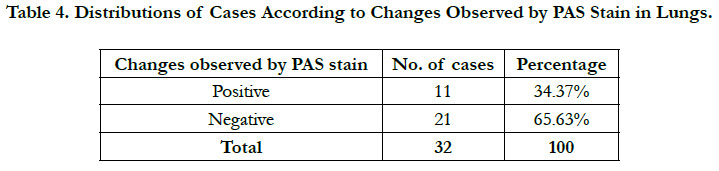
Table 4. Distributions of Cases According to Changes Observed by PAS Stain in Lungs.
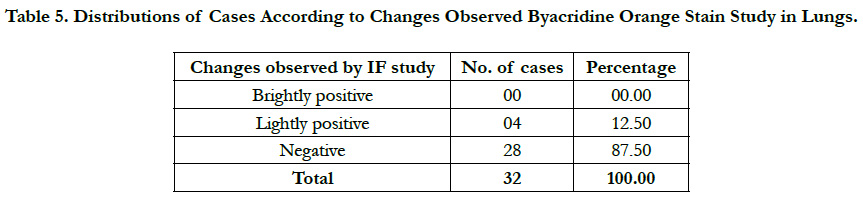
Table 5. Distributions of Cases According to Changes Observed Byacridine Orange Stain Study in Lungs.
Figure 6. Immunofluroscence Stain - Lightly Positive in Lungs (IF stain, 40X).

Figure 7. Immuno Fluroscence Stain- Lightly Positive in Early Myocardial Infarct (control slide- IF stain, 40X).

Figure 8. IF - brightly positive in old myocardial infarct (control slide- IF stain, 40X).
It was observed that routine H&E staining did show above referred pathological findings. But the use of PAS stain did not increase any further knowledge. On the contrary, it was negative in about 65 percent of cases. Similarly, use of Acridine orange stain also did not throw any further light on whatever knowledge achieved by H&E stain, the fluorescence turned out to be negative in about 87 per cent of cases and rest of the cases also it was only weakly positive.
Discussion
In the present study, maximum numbers of cases were in the age group of 21 to 30 years (31.25%) followed by age groups of 11 to 20 years (28.12%) and 31 to 40 years (21.87%). Females (87.50%) outnumbered males (12.50%) with M: F ratio of 1:7.
Age & Gender distribution of cases in present studies are concordant with of other Indian studies [8-10]. However study done by study by Olaitan PB et al., showed maximum number of cases in old aged male [11]. This may be due to different geographical region and environmental factors.
Maximum deaths were due to accidental burns (65.63%) and the rest were due to suicidal burns (34.37%). Chawla et al., & Jagannath HS et al., studied majority of cases due to accidental burns [2-10].
In present study, most of the cases had history of flame burns (81.25%) while remaining cases had chemical burns (18.75%). Buchade D et al., and Olaitan PB studied similar finding [9, 11].
In the present study it was observed that maximum number of cases (28.13 %) of the victims could not survive for more than 12 hours. Chawla et al., & Buchade D et al., studied majority of cases duration of survival is not more than 24 hours [2, 9].
In majority cases of the present study, cause of death was septicaemia (37.50%) followed by hypovolemic shock (31.25%) and acute renal failure (21.88%). Chawla et al., studied majority cases cause of death was due to septicemia [2].
In present study, majority of gross findings of lungs showed heavy, firm, congestion followed by congestion & frothy fluid on cut surface & consolidation, which is in accordance with other studies.
In present study, majority of histopathological features showed diffuse alveolar damage followed by interstitial pneumonitis, diffuse interstitial edema, bronchopneumonia and pulmonary edema. Rare findings like focal atelectasis, areas of emphysema, necrotizing bronchiolitis were also seen. Toor AH et al., observed diffuse alveolar damage in 16 (48.48%) patients, acute bronchopneumonia in seven (21.21%) patients, and necrotizing inflammation in seven (21.21%) patients, which is accordance with other study [12].
Argamaso RV showed changes of pulmonary edema in majority of cases (70.00%) followed by pneumonitis and abscess formations in 26.66% of cases [13]. So, these findings are not consistent with present study. Different rate of post burn survival may be the cause of this discrepancy.
In the present study all cases showing changes of pulmonary edema had minimum duration of survival (0-12 hours) whereas cases showing changes of bronchopneumonia had maximum duration of survival (4 days or more). Cases showing changes of diffuse alveolar damage and interstitial pneumonitis were distributed widely in correlation with duration of survival from 0-12 hours to 6-7 days.
Hasleton PS et al., noted congestion of alveolar walls, interstitial and intra alveolar edema and intra alveolar hemorrhage in first 48 hours. Pneumonia and septicemia were common findings after 48 hours. Intravascular microthrombi denoting disseminated intravascular coagulation along with above changes were also noted after 48 hours [14]. So, present study is in accordance with this study.
In the present study, histochemistry by PAS stain in sections taken from lungs was performed to get any possible extra information. 21 cases (65.63%) were found negative and 11 cases (34.37%) were showing PAS positivity where hyaline membrane was formed due to diffuse alveolar damage.
Chopra P et al., have proved that the examination of myocardium after acridine orange stain, under fluorescent light is more sensitive than autofluorescence for detecting ischemia [16]. This method has previously been shown to be useful in the identification of myocardial infarcts in both humans and experimental animals. In the present experimental study, It was observed that sections taken from lungs stained by acridine orange stain and observed under fluorescent microscope were found negative in 28 cases (87.50%) and lightly positive in 04 cases (12.50%). This light positivity may be due to necrotic areas which can occur in diffuse alveolar damage [1, 15]. Bhetariya BV et al., studied profile of kidney in burns cases by acridine orange stain and observed under fluorescent microscope were lightly positive in 15 cases (46.88%) and brightly positive in 08 cases (25.00%) whereas negative in 09 cases (28.12%) [17].
Though other authors have studied myocardium [16] and kidneys [17] using fluorescence technique, we did not come across any studies similar to present one.
Conclusion
1. On gross examination, lungs were predominantly heavy, firm, congested. In few cases, areas of consolidation were seen.
2. Microscopically, sections taken from lungs studied by H & E stain showed changes of pulmonary edema in cases with minimum duration of survival (0-12 hours) and changes of bronchopneumonia in cases with maximum duration of survival (4 days and more). Changes of diffuse alveolar damage and interstitial pneumonitis were seen in the cases with wide range of duration of survival.
3. PAS stain showed positivity in sections taken from lungs where hyaline membrane was formed due to diffuse alveolar damage.
4. Fluorescent study using acridine orange showed positivity in sections taken from lungs of cases showing necrotic changes with H & E stain. They were brightly positive in some cases and lightly positive in others which indicate the extent and intensity of necrosis and diffuse alveolar damage.
5. PAS and flourescence studies undertaken by us confirm our findings studied by H&E stain in few cases, while in majority of cases they showed negative results.
6. It is suggested that these advance techniques do not add any new dimension to the forensic value of burn cases.
Acknowledgement
We are very thankful to Dr. Pravina Santwani, Professor & head of department for their kind support & guidance.
References
- Reddy KSN (2009) The essentials of forensic medicine & toxicology. (28th edn), K. Suguna Devi publications, Om Sai Laser Graphics, Hyderabad, India. 280, 258.
- Chawla R, Chanana A, Rai H, Aggarwal AD, Singh H, et al., (2011) Clinico-Pathological Profile in Deaths Due To Burns. J Indian Acad Forensic Med. 33(1): 14-17.
- Taylor FW, Gumbert JL (1965) Cause of Death from Burns: Role of Respiratory Damage. Ann surg. 161(4): 497-501.
- Gupta BD, Jani CB (2003) Status of histopathological examination in medicolegal postmortem examination: Indian scenario. J Forensic Med Toxicol. 20(2): 15 8.
- Molina DK, Wood LE, Frost RE (2007) Is routine histopathologic examination beneficial in all medicolegal autopsies ? Am J Forensic Med Pathol. 28(1): 1-3.
- Herndon DN, Barrow RE, Linares HA, Prien T, Traber LD, et al., (1988) Inhalation injury in burned patients: effects and treatment. Burns Incl Therm Inj. 14(5): 349–356.
- Gohel H, Desai N, Tripathi S, Gupta B, Santwani P (2012) Post mortem, study of heart in cases death using acridine orange fluorescene and haematoxylin and eosin stain. IJHMC. 1(5): 115-123.
- Gorea RK, Ahluwalia (1990) Deaths due to Thermal Injury – An autopsy study. IJFS. 4(3): 109.
- Buchade D, Kukde H, Dere R, Savardekar R (2011) Pattern of Burns. Cases Brought to Morgue, Sion Hospital, Mumbai: A Two Year Study. J Indian Acad Forensic Med. 33(4): 311-12.
- Jagannath HS, Tapare V, Rayate M (2011) Study of socio-demographic profile of burncases admitted in Shri Chhatrapati Shivaji Maharaj General Hospital, Solapur. National J of Community Med. 2(1): 19-23.
- Olaitan PB, Jiburum BC (2006) Analysis of burn mortality in a burns centre. Ann Burns Fire Disasters. 19(2): 59-62.
- Toor AH, Tomashefski JF, Kleinerman J (1990) Respiratory tract pathology in patients with severe burns. Hum Pathol. 21(12): 1212-1220.
- Argamaso RV (1967) Pathology, Mortality and Prognosis of Burns: A Review of 54 Critical and Fatal Cases. Canad Med Ass J. 97(9): 445-449.
- Hasleton PS, McWilliam L, Haboubui NY (1983) The lung parenchyma in Burns. Histopathology. 7(3): 333-347.
- Kumar, Abbas, Fausto, Aster (2010) Robbins and Cotran: Pathological basis of disease. ( 8th edn), PA, USA, Elsevier. 2010: 421, 680-682, 935-938.
- Chopra P, Sabherwal U (1988) Histochemical and Fluorescent Technique for Detection of Early Myocardial ischemia following Experimental coronary Artery occlusion: A Comparative and Quantitative study. Angiology. 39(2): 132-40.
- Bhetariya BV, Desai NJ, Gupta BD, Patel PN (2016) Profile of Kidney Histopathology in Cases of Burns - Particular Emphasis on Acridine Orange Fluorescence Study and to Explore its Forensic Utility. J Clin Diagn Res. 10(4): EC01-EC05.





