Sadistic Sexual Assault Case Study
Alghffar EA1*, Said AA2
1 Radwan Forensic Consultant, Abha Medicolegal Center, Saudi Arabia.
2 ALHabshan Forensic Consultant, Abha Medicolegal Center, Saudi Arabia.
*Corresponding Author
Eman Abd Alghffar,
Radwan Forensic Consultant, Abha Medicolegal Center, Saudi Arabia.
Email: emanradwan93@yahoo.com
Received: February 17, 2017; Accepted: April 03, 2017; Published: May 16, 2017
Citation: Alghffar EA, Said AA (2017) Sadistic Sexual Assault Case Study. Int J Forensic Sci Pathol. 5(2), 326-330. doi: http://dx.doi.org/10.19070/2332-287X-1700072
Copyright: Alghffar EA© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.History of the Murder
3.External Examination
4.Autopsy and Exposing the Body Cavities
5.The Head, Face and Neck
6.The Chest
7.Abdomen and Pelvis
8.Discussion
9.References
Introduction
Sexual sadism disorder is the condition of experiencing sexual arousal in response to the extreme pain, suffering or humiliation of others [1]. Several other terms have been used to describe the condition, and the condition may overlap with other conditions that involve inflicting pain. It is distinct from situations in which consenting individuals use mild or simulated pain or humiliation for sexual excitement [4]. Sexual sadism disorder has been found to be potentially dangerous if paired with symptoms of borderline personality disorder or psychopathy which increases the likelihood of one acting on their sexually sadistic fantasies.
History of the Murder
IN 25/1/2016 police notified about assault happened in social follow-up house, police and forensics responded and transfer to scene of the crime. They found that a domestic worker female was assaulted by another worker female both females are Christian and Kenyan nationality the assailant was in a hysterical state strains her hair and shouts by Kenyan language she said that she follows the orders of their religion and there is a demon inside her body asked her to drink blood to get out from her body so she assault the victim. Police found blood in various locations and under the internal stairs of the wards for female workers the assailant arrested. The victim have transferred to Hospital the medical reports approved presence of many injuries scattered in her head and body with sever assault on the reproductive system.
Witten's was two females one is Saudi citizenship employer she said she had seen the offending drag the victim with her hair on the internal stairs and tried to assault her, but victim ran away and then fall on the floor then the offending enter her hand into the body of the victim and withdraw blood and drink it, the other wittiness was Kenyan, she heard that the assailant was speaking with Kenyan language and said that she wanted to drink blood to get rid from demon.
Summary of Medical File
The file approved that victim admitted to hospital in a coma with vaginal bleeding, immediately, endotracheal tube inserted with artificial respiration many blood analysis done with normal result. CT brain shows severe head injury - brain hernation and edema broken lower jaw, vaginal examination showed sever laceration vaginal orifice perennial laceration, treatment: stitches of wounds supportive medicine and fluid was given. Many blood analysis (Liver, kidney function, sugar level, blood gases, calcium and potassium level done with normal result toxicology analysis free (no hypnotic - antidepressant - alcohol).
Birth day in identification card of the victim is-1971/ 5/19 . Victim died within three days of admission.
External Examination
Bare dark color female 170 cm length and 80 kg the body was in cold stiffness with faint hypostasis at the background there is no butterfaction there is minimal bleeding from the nose.
The recent injuries as following:
1. Many small brown abrasions in the middle of the frontal area.
2. Multiple blue contusions with variable size and shape scattered all over the face, at the frontal area look at Figures (1 & 3), around eyes with subcongictival hemorrhage (Figure 2), also checks - lips and left mandible angel (Figure 4), the size of contusion from 1 X 2 cm up to 3 X 4 cm.
3. Five longitudinal blue contusions variable in length from 8 cm to 15 cm width about 1 cm three in front of the left thigh and two in front of right thigh.
4. Many stitches in vaginal and anal orifices after removal the stitches we found Large lacerated wound measuring about 7 X 5 cm including the posterior vaginal wall, perennial and
anal canal orifice making them as one opening - Five superficial small injures around anal opening every one about 2 cm length and 3 mm width (Figure 5).
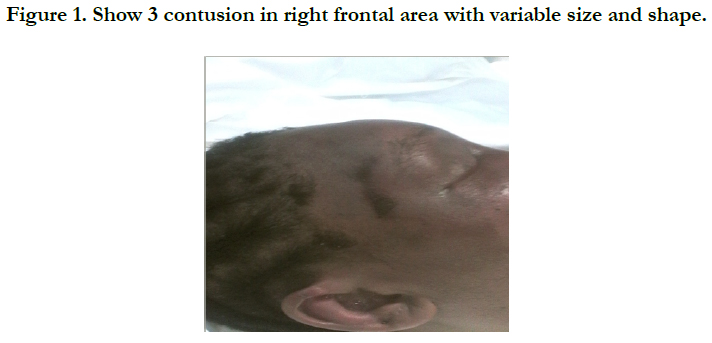

Figure 1. Show 3 contusion in right frontal area with variable size and shape.
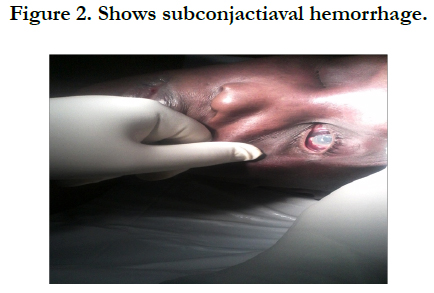

Figure 2. Shows subconjactiaval hemorrhage.
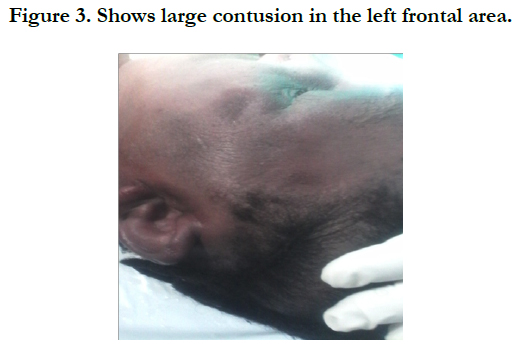

Figure 3. Shows large contusion in the left frontal area.
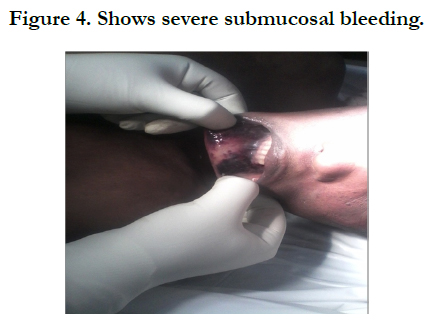

Figure 4. Shows severe submucosal bleeding.


Figure 5. After removal of stitches large wound extend from posterior vaginal wall to anal canal making them one hole with five superficial small injures around anal opening.
Autopsy and Exposing the Body Cavities
By incision the scalp from behind each ear, and reflection of tissues forwards to the lower forehead and back to the occipital. Midline incision from above larynx to the pubis the skin, subcutaneous tissues and fat are flayed off laterally from the main incision.
The Head, Face and Neck
By scalp incision we found subcutaneous bleeding in frontal area, circular bleeding 3 cm diameter at versus vertex, and bleeding in both temporal muscles. There is vertical fissure fracture in outer table of left parietal bone 3 cm length (Figure 6), by rising the vault of the skull there is milled to moderate subdural and subarachnoid hemorrhage cover most brain surface (Figure 7) base of skull was free from fractures. There is subcutaneous hemorrhage around comminuted fracture in the left mandible angle, also minimal bleeding on posterior surface of left thyroid cartilage Other facial bones, hyoid bone and cervical vertebrae free from fractures also the trachea and esophagus free from injuries with clear lumen.
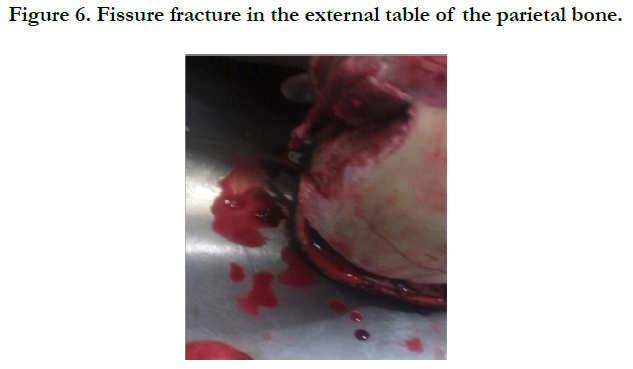

Figure 6. Fissure fracture in the external table of the parietal bone.
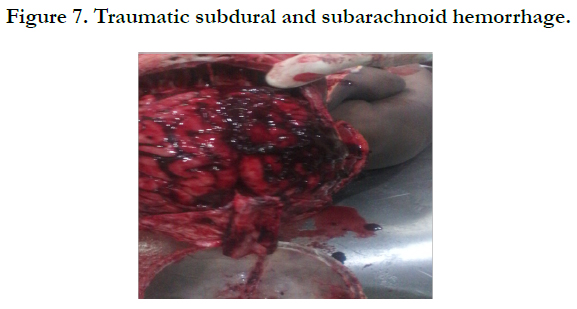

Figure 7. Traumatic subdural and subarachnoid hemorrhage.
The Chest
After midline incision and flayed off the skin, subcutaneous tissues and fat laterally and cutting the sternoclavicular joints removing sternum, and peritoneum incision exposing all the body cavities removal all chest and abdominal viscera as one block there is no subcutaneous hemorrhage we extract the heart and lungs. Examination of heart chambers aorta pulmonary coronaries was free. Examination of lungs showed no injuries but minimal basal lung collapse small foci of anthracosis chest cavity free from bleeding and effusion and thoracic vertebra were intact.
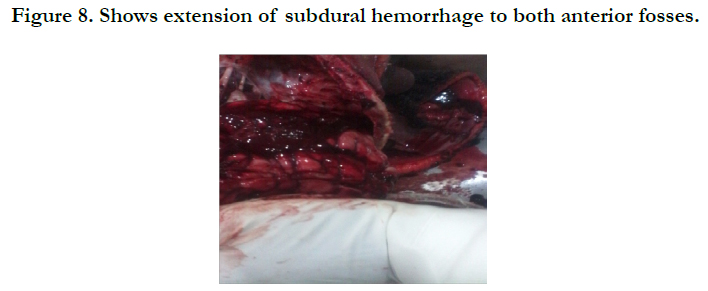

Figure 8. Shows extension of subdural hemorrhage to both anterior fosses.
Abdomen and Pelvis
We found minimal clotted blood in the left side of the pelvis and the left transverse ligament (Figure 10 ) then we extract the uterus, ovaries and vagina and we found some stitches with some clotted blood in the lacerated wound which comprehensive lower part of vagina as well as the lower part of anterior wall of anal canal and anus with stitches in lower ends of deep pudendal and left vaginal artery (Figure 9). The uterus, tubes and ovaries size was normal, the slit of uterus show small menstrual blood. The other viscera stomach, liver, spleen, pancreas, kidneys and intestines both types were intact. Then we felt the safety of the rest of the bones of the body.
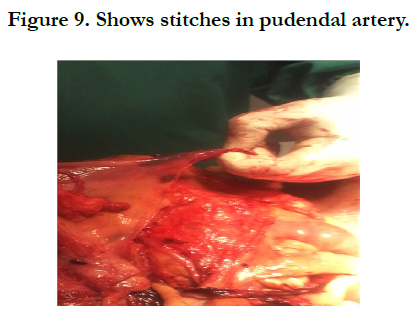
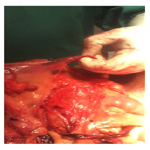
Figure 9. Shows stitches in pudendal artery.
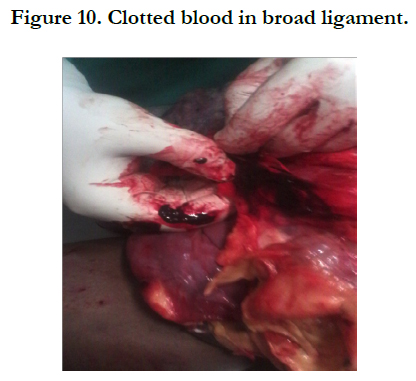

Figure 10. Clotted blood in broad ligament.
NB: The following Figures shows the positive finding data.
The results of toxicology analysis were free (no hypnotic - antidepressant-alcohol-alkaloid ).
1. Injuries seen and described from item 1 to item 4 detected in external examination virtual scattered face, back and genitals, lower extremities as well as what we have seen by autopsy, subglail, subarachnoid hemorrhage brain injuries and pelvis all injuries, traumatic and frictional occurred as a result of clash with blunt objects and consistent with the occurrence of with assaulting by hand and traction on the stair while the wounds in the external genital organs consistent with the occurrence of the introduction of solid body inside the vagina of the victim, such as the hand of the accused.
2. The cause of death related to head injuries Brain hemorrhage edema stroke and swollen leading to compression on the vital centers of the heart and breathing in the brain.
3. The case considered sadistic assault.
Discussion
Robert. et al., 1994, [7] said that Homosexuality as a condition of "sexual desire or behavior directed toward a person or persons of one's own sex". Homosexual acts a bad choice for individuals is the significantly higher rates of domestic violence in homosexual couples. In addition, according to experts homosexual murders are relatively or quite common and often homosexual murders are very brutal. Also, the homosexual population has a greater propensity to engage in illegal drug use.
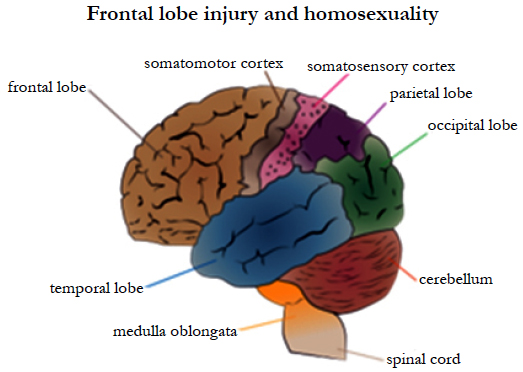

Frontal lobe injury and homosexuality.
Neurosurgery journal Psychiatry [6]. 2007 reported that: Disinhibited sexual behavior has been reported following damage to the frontal lobes, particularly the orbitofrontal region of the limbic system.
American Psychiatric Association. 2013 ( reported that there is relationships between “sexual deviation”, with a lesion temporal and extra temporal. The frontal lobe plays a role in controlling sexual behavior.
We review the human literature examining the effects of neurological insult on human sexual behaviour. We provide a synthesis of the findings to date, and identify key brain regions associated with specific aspects of human sexual behaviour. These include subcortical and cortical regions, with the mesial temporal lobe and the amygdala in particular being a crucial structure in the mediation of human sexual drive.
Breslow: et al., 1985 [2] discussed the fact about how the woman really rape/sexually assault another woman.
Many of us have been bought up to believe that rape/sexual assault requires penile penetration - and so when it comes to women- on-women sexual violence, some dismiss that sexual assault can even occur between lesbians. This is a falsehood.
Sexual assault between women can include:
- Forced vaginal/anal penetration with digits or objects;
- Forced sexual touching.
Sexual sadism disorder is the term refers to the “recurrent and intense sexual arousal from the physical or psychological suffering of another person, as manifested by fantasies, urges, or behaviors”. It is classified as one of the paraphilias, called an “algolagnic disorder”, which is one of the “anomalous activity preferences”. The formal diagnosis of Sexual Sadism Disorder would apply if the individual has acted on these urges with a nonconsenting person or if the urges cause significant distress to the individual.
Sexual sadism could be diagnosed if:
1. The person repeatedly and intentionally inflicted suffering on a nonconsenting person, to experience sexual excitement.
2. Repeatedly or exclusively preferred simulated or mild suffering with a consenting sexual partner.
3. Employs extensive, permanent, or potentially fatal suffering to achieve sexual excitement, regardless of the consent of the other person.
Dietz: Et al., 1990 said that [3] Sadistic personality disorder does not actually refer to any sexual interest and instead refers to the pervasive disregard for the well-being of others. It is usually associated with a history of violence and criminality (which can include, but is not limited to sexual crimes).
Krueger., 2010 [5] told that Marquis de Sade, as disorder is derivative of his name Marquis de Sade, a French aristocrat, philosopher and writer of explicit sexual works, was born in Paris in 1740. His writings depict violence, criminality and blasphemy against the Catholic Church. During the French Revolution he was an elected delegate to the National Convention. The last 13 years of his life were spent in an insane asylum. He died in 1814.
References
- American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders (5th edn), Arlington, VA: American Psychiatric Publishing.
- Breslow N, Evans L, Langley J (1985) On the prevalence and roles of females in the sadomasochistic subculture: Report of an empirical study. Arch Sex Behav. 14(4): 303-317.
- Dietz PE, Hazelwood RR, Warren J (1990) The sexually sadistic criminal and his offenses. Bull Am Acad Psychiatry Law. 18(2): 163-178.
- Freund K, Blanchard R (1986) The concept of courtship disorder. J Sex Marital Ther. 12(2): 79-92.
- Krueger RB (2010) The DSM diagnostic criteria for sexual sadism. Arch Sex Behav. 39(2): 325-345.
- Baird AD, Wilson SJ, Bladin PF, Saling MM, Reutens DC (2007) Neurological control of human sexual behaviour: insights from lesion studies. J Neurol Neurosurg Psychiatry. 78(10): 1042–1049.
- Robert T Michael, John H Gagnon, Edward O Laumann, Gina Kolata (1994) Sex in America: A Definitive Survy. Little, Brown and Company, Boston.





