Walking Economy is Impaired in Older Men and Women with Type 2 Diabetes
Gardner AW*, Montgomery PS
Reynolds Oklahoma Center on Aging, Donald W. Reynolds Department of Geriatric Medicine, University of Oklahoma Health Sciences Center (OUHSC), Oklahoma City, OK, USA.
*Corresponding Author
Andrew W. Gardner, Ph.D.,
Professor and Donald W. Reynolds Chair in Aging Research, OUHSC, Donald W. Reynolds Department of Geriatric Medicine, 1122 N.E. 13th Street,
O’Donoghue Research Building, Suite 1200, Oklahoma City, OK 73117, USA.
Tel: (405) 271-4272 ext. 42743
Fax: 405-271-3887
E-mail: andrew-gardner@ouhsc.edu
Received: April 26, 2016; Accepted: May 18, 2016; Published: May 19, 2016
Citation: Gardner AW, Montgomery PS (2016) Walking Economy is Impaired in Older Men and Women with Type 2 Diabetes. Int J Diabetol Vasc Dis Res, S3:002. 7-12.DOI : dx.doi.org/10.19070/2328-353X-SI03002
Copyright: Gardner AW© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: We compared the walking economy in older participants with and without type 2 diabetes.
Methods: Walking economy was determined in 115 older participants with type 2 diabetes and 130 older control participants without diabetes by continuously measuring oxygen uptake during a treadmill test in which the work rate was at a constant speed of 2 mph and a grade of 0% for a duration of 10 minutes. Participants also completed a Balke treadmill protocol for the determination of peak oxygen uptake, defined as the highest oxygen uptake value attained during the final work stage attained. Fractional utilization was then calculated as the walking economy oxygen uptake divided by peak oxygen uptake, expressed as a percentage.
Results: Compared to those without diabetes, participants with type 2 diabetes were older (p=0.042), had higher prevalence of men (p=0.034), obesity (p=0.010), chronic kidney disease (p=0.020), peripheral artery disease (p=0.024), and had a higher body mass index (p=0.025), and waist/hip ratio (p=0.006). After adjusting for these variables, the participants with diabetes had higher walking economy (p<0.001), fractional utilization (p<0.001), and lower peak oxygen uptake (p<0.001) than those without diabetes (p<0.001).
Conclusions: Older men and women with type 2 diabetes are less economical when they ambulate at a given speed than compared to control participants without diabetes, independent of their greater co-morbid burden. The impaired walking economy in the diabetic participants is further magnified by their lower aerobic fitness, thereby leading to a higher fractional utilization of oxygen consumed during a given walking task.
2.Introduction
3.Methods
3.1 Participants
3.2 Outcome Measurements
3.3 Statistical Analyses
4.Results
5.Discussion
5.1.Walking Economy in Type 2 Diabetes
5.2. Fractional Utilization and Peak Oxygen Uptake in Type 2 Diabetes
5.3.Potential Mechanisms
5.4.Limitations
5.5.Conclusion and Clinical Significance
6.Acknowledgements
7.References
Keywords
Ambulation; Exercise; Mobility; Oxygen Consumption; Women.
Introduction
The global prevalence of diabetes mellitus in adults is 9%, affecting 415 million adults in 2015 which is expected to increase to nearly 642 million by 2040 [1]. People over the age of 60 have a disproportionately high prevalence, as approximately 35% of all cases worldwide (135 million) are older adults [2]. Type 2 diabetes mellitus represents up to 95% of these cases [3], and is associated with high burden of comorbid conditions, such as peripheral neuropathy, nephropathy, retinopathy, cardiovascular complications, and a high mortality rate that exceeds 5 million per year [2]. Not surprisingly, 12% of global health expenditure is spent on diabetes [2].
The ability to ambulate well is important in maintaining functional independence in older adults. Walking economy, defined as the oxygen uptake during ambulation, is a key aspect in sustaining ambulatory activities [4]. Impaired walking economy is reflective of high oxygen uptake during a given ambulatory task, and may be a consequence of an altered gait pattern [5-7]. The clinical relevance of poor walking economy is that ambulation is performed at a higher intensity of exercise, particularly when combined with lower aerobic capacity, thereby potentially leading to faster fatigue, limited mobility, and lower daily physical activity. Older adults with diabetes have impairments in spatial and temporal gait characteristics, such as decreased gait velocity, shorter step length, and increased step width, stance time, and double-support time [8-10], all of which may impair walking economy. Additionally, individuals with diabetes have higher prevalence of cardiovascular comorbid conditions, lower physical activity and leg strength, and higher body mass index, which are additional factors that may impact ambulation [10]. However, surprisingly little information is available on the impact of diabetes on walking economy in older adults.
The purpose of this study was to compare the walking economy in older participants with and without type 2 diabetes. We hypothesized that compared to those without type 2 diabetes, participants with diabetes would have worse walking economy, defined as a higher oxygen uptake during walking at a given pace. Furthermore, walking at a constant pace would be performed at a higher fractional utilization (i.e., relative exercise intensity) in the participants with type 2 diabetes due to the combination of having a higher walking economy value and a lower maximal oxygen uptake.
Methods
Approval and Informed Consent
The institutional review board at the University of Oklahoma Health Sciences Center approved the procedures of this study. Written informed consent was obtained from each participant at the beginning of investigation.
Recruitment
Individuals with and without type 2 diabetes who were ≥ 50 years of age, and who were able to walk independently without a walking aid [11] were recruited to participate in this study. The participants were recruited by distributing informational flyers in clinics at the University of Oklahoma Medical Center and in various locations in the Oklahoma City area, and by media advertising in local newspapers and in campus-wide email messages.
Medical Screening
Participants were evaluated during a medical history and physical examination. Demographic information, height, weight, body mass index, waist and hip circumferences, cardiovascular risk factors, co-morbid conditions, blood samples, and a list of current medications were obtained.
Definitions of Clinical Characteristics
Obesity was defined by a body mass index ≥30 [12], and abdominal obesity was defined by a waist circumference ≥102 cm in men and ≥94 cm in women [12]. Hypertension was defined by having at least one of the following conditions: a systolic blood pressure ≥140 mmHg, a diastolic blood pressure ≥90 mmHg, or currently taking antihypertensive medications [13]. Dyslipidemia was defined by having at least one of the following conditions: a cholesterol value ≥200 mg/dl, a triglyceride value ≥150 mg/dl, a low-density lipoprotein level ≥130 mg/dl, a high-density lipoprotein level < 40 mg/dl in men and < 50 mg/dl in women, or currently taking lipid-lowering medications [14]. Peripheral artery disease was determined by measuring the ankle and brachial systolic blood pressures after 10 minutes of supine rest, as previously described [15], and was defined by an ankle/brachial index value <0.90 [16]. Coronary artery disease was defined by having at least one of the following conditions: a history of coronary percutaneous transluminal angioplasty, coronary stents, coronary artery bypass graft, myocardial infarction, or symptoms of exertional angina. Cerebrovascular disease was defined by having one of the following conditions: a history of carotid stents, coronary endovascular angioplasty, coronary bypass graft, stroke, or transient ischemic attacks. Chronic kidney disease was determined using the four variable modification of diet in renal disease equation, and was defined as having an estimated glomerular filtration rate < 60 ml/ min per 1.73 m2 [17].
Inclusion and Exclusion Criteria
Participants were included in the type 2 diabetes group if they met either or both of the following criteria: fasting plasma glucose ≥126 mg/dl [2], and/or current use of diabetes medications such as oral medications and/or insulin [18]. Individuals were included in the non-diabetic control group if they met both of the following criteria: fasting plasma glucose < 100 mg/dl, and not taking diabetes medications [3]. Individuals in either group were excluded from participating for the following reasons: (a) fasting plasma glucose between 100 and 125 mg/dl and not on diabetes medications, (b) any condition that would contraindicate performing exercise tests according to the American College of Sports Medicine [19], (c) active cancer, (d) stage 5 chronic kidney disease (end stage), as defined by an estimated glomerular filtration rate < 15 ml/min per 1.73 m2 [17], (e) abnormal liver function [19], and (f) lower extremity ulcerations. A total of 115 participants with type 2 diabetes and 130 participants without diabetes were deemed eligible for this investigation.
Peak Aerobic Power
Oxygen uptake, respiratory quotient, and ventilation were measured continuously with a Medical Graphics VO2000 metabolic system (Medical Graphics Inc, St. Paul, MN) during a Balke treadmill protocol. The participants performed this test consisting of a constant walking speed of 3.4 mph, beginning at an initial incline of 2% grade and increasing an additional 2% grade every two minutes until exhaustion. Heart rate was recorded at the completion of each minute of exercise, and blood pressure was measured during the final minute of each 2-minute work stage. The highest oxygen uptake obtained during the final minute of exercise was recorded as the peak oxygen uptake, expressed in ml.kg-1min-1. The final values obtained during the test for respiratory quotient, ventilation, heart rate, and blood pressure were recorded as peak values. The test-retest intraclass reliability coefficient for peak oxygen uptake in our laboratory is R = 0.95, and the coefficient of variation is 3.4%.
Walking Economy Treadmill Test
This test was the
experimental protocol used to obtain the primary outcome measure of walking economy (oxygen uptake expressed as ml.kg-1min-1). Participants performed the walking economy treadmill test in which the work rate was at a constant speed of 2 mph and a grade of 0% for a duration of 10 minutes [20]. Oxygen uptake, respiratory quotient, and ventilation were measured continuously throughout the test with the Medical Graphics VO2000 metabolic system. Heart rate was recorded at the end of each minute of exercise, and blood pressure was obtained every other minute during the test. To better ensure that the participants had reached a metabolic steady-state level, the minute values of oxygen uptake, respiratory quotient, and ventilation were averaged over the final three minutes of the exercise test. Heart rate and blood pressure were calculated as the average values obtained during minute 8 and minute 10 of the test. The test-retest intraclass reliability coefficient for walking economy in our laboratory is R = 0.92, and the coefficient of variation is 3.8%.
All statistical analyses were performed using the Statistical Package for the Social Sciences software – SPSS version 23 (IBM Corp, New York, USA). Continuous variables were summarized as mean and standard deviation, whereas categorical variables were summarized as relative frequency. Unpaired t-tests for the continuous variables and chi-square tests for the categorical variables were used to assess whether differences in the clinical characteristics existed between the groups with and without type 2 diabetes. One-factor analysis of covariance (ANCOVA) was used to compare walking economy and the other metabolic and cardiovascular measurements during submaximal and peak exercise, after adjusting for clinical characteristics that were significantly different between the two groups (age, sex, body mass index, waist/hip ratio, obesity, and peripheral artery disease). Residual analysis was performed, homoscedasticity was analyzed by graphical analysis (scatterplot) and adherence to the normal distribution was tested using the Kolmogorov-Smirnov test. All analyses were performed with a two-tailed significance level of 0.05.
Results
The clinical characteristics of the participants with and without type 2 diabetes are displayed in Table 1. Compared to the controls, the participants with diabetes were older (p = 0.042), had higher prevalence of men (p = 0.034), obesity (p = 0.010), chronic kidney disease (p = 0.020), and peripheral artery disease (p = 0.024), and they had a higher body mass index (p = 0.025), and waist/hip ratio (p = 0.006).
The peak exercise performance measurements of participants with and without type 2 diabetes are shown in Table 2. After adjustment for age, sex, body mass index, waist/hip ratio, obesity, chronic kidney disease, and peripheral artery disease, the peak oxygen uptake was lower in the participants with diabetes than in the controls (p < 0.001). None of the other measures obtained at peak exercise were significantly different between the two groups.
The submaximal exercise performance measurements of participants with and without type 2 diabetes are shown in Table 3. After adjustment for age, sex, body mass index, waist/hip ratio, obesity, chronic kidney disease, and peripheral artery disease, the participants with diabetes had higher values for walking economy (p < 0.001), fractional utilization (p < 0.001), and systolic blood pressure during submaximal exercise than in the controls.
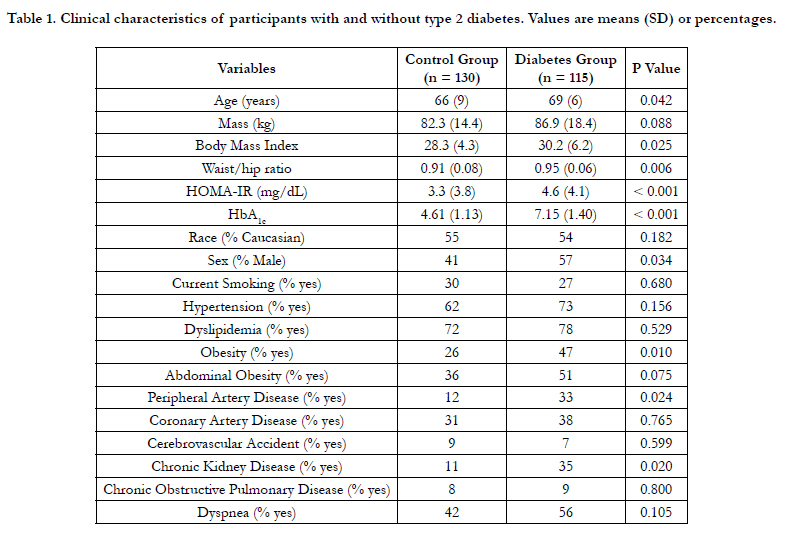

Table 1. Clinical characteristics of participants with and without type 2 diabetes. Values are means (SD) or percentages.
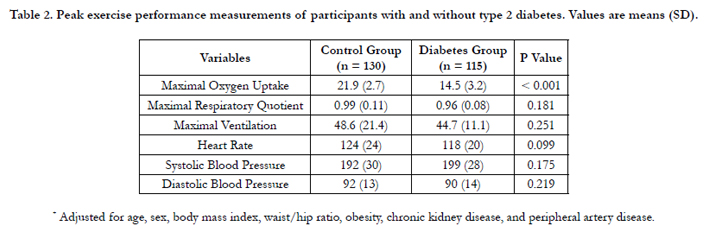
Table 2. Peak exercise performance measurements of participants with and without type 2 diabetes. Values are means (SD).
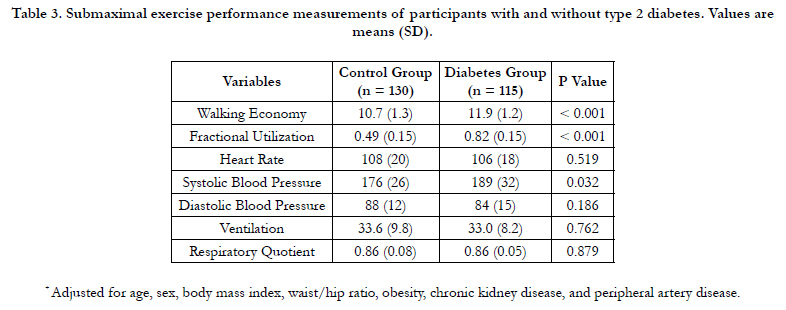
Table 3. Submaximal exercise performance measurements of participants with and without type 2 diabetes. Values are means (SD).
Discussion
The novel findings of this investigation were that after adjusting for greater co-morbid burden, participants with type 2 diabetes had impaired walking economy, lower peak oxygen uptake, and higher fractional utilization than compared to those without diabetes.
Walking economy during ambulation represents the metabolic cost of exercise. Less economical walking, measured by higher oxygen uptake at a constant work rate, indicates that exercise is performed at a higher percentage of exercise capacity, thereby reducing the tolerance to sustain ambulation [4]. Our participants with type 2 diabetes had an 11% higher walking economy than those with diabetes as they walked at a given pace of 2 mph during a submaximal treadmill test. This finding indicates that older men and women with type 2 diabetes require a greater amount of oxygen to ambulate at an absolute exercise intensity that is representative of many activities of daily living, which may limit their ability to sustain exercise, impair their physical function, and reduce their physical activity level.
The negative impact of poor walking economy of the participants with type 2 diabetes is magnified even further by their 34% lower peak oxygen uptake, which supports previous work [21]. This observation indicates that the task of ambulating at a given pace of 2 mph is accomplished at a much higher fractional utilization (i.e., relative exercise intensity) of 82% of peak exercise in those with diabetes compared to only 49% of peak in the control group. The higher fractional utilization of the participants with type 2 diabetes suggests that they may have been ambulating near or above their anaerobic threshold, whereas the low fractional utilization of the non-diabetic controls indicates that exercise was accomplished aerobically. The submaximal exercise task was not only more challenging metabolically for those with diabetes, but it also elicited a more exaggerated cardiovascular response, measured by a higher systolic blood pressure during ambulation than compared to the non-diabetic controls. It is possible that the higher exercise systolic blood pressure in participants with type 2 diabetes was related to greater endothelial dysfunction [22] or greater activation of the pressor reflex [23].
There are several potential mechanisms for the impaired (i.e., higher) walking economy in the diabetic group. Because the participants with type 2 diabetes performed the walking task at a much higher relative intensity, they may have had a greater recruitment of fast-twitch motor units, which would increase oxygen uptake during exercise [24,25]. Additionally, muscle denervation may impair optimal motor unit recruitment during exercise [26], thus making exercise less efficient. Indeed, impairment in peripheral nerve function in older individuals with diabetes partially explains their worse physical function compared to non-diabetic controls [27]. Furthermore, individuals with diabetes have slower oxygen kinetics during the onset of exercise [21], which may lead to an oxygen deficit and reduced efficiency in performing subsequent exercise, as evident by an increase in the slow component of oxygen uptake during a constant exercise work load [4]. Finally, older individuals with diabetes have alterations in spatiotemporal gait characteristics compared to non-diabetic controls, such as decreased gait velocity, shorter step length, greater step width, and increased stance time and double-support time [8-10]. These spatiotemporal alterations have not only been observed in older diabetics with peripheral neuropathy [28], but also in those without peripheral neuropathy [29,30], suggesting that type 2 diabetes may result in central damage to the vestibular, somatic, and autonomic systems from impaired microcirculation, or that a compensatory strategy is adopted for greater stability and balance at the expense of gait speed [1].
Several limitations exist for this study. Participants were volunteers and therefore may represent those who were more interested in their health, who had better transportation to our research center, and who had better health than individuals who did not volunteer. The cross-sectional design comparing those with and without diabetes does not indicate causality. Furthermore, these results are only generalizable to older men and women with type 2 diabetes, who are overweight-to-mildly obese, and who have a high prevalence of hypertension and dyslipidemia. Despite these limitatons, this study had a good representation of men and women, and caucasians and African-Americans. Thus, we believe the findings in the present investigation are generalizable to a large number of older men and women with type 2 diabetes who have concomitant cardiovascular risk factors.
We conclude that older men and women with type 2 diabetes are less economical when they ambulate at a given speed than compared to control participants without diabetes, independent of their greater co-morbid burden. The impaired walking economy in the diabetic participants is further magnified by their lower aerobic fitness, thereby leading to a higher fractional utilization of oxygen consumed during a given walking task. The clinical significance of impaired walking economy in older men and women with type 2 diabetes is that ambulation is completed at higher metabolic intensity, which may limit their ability to sustain exercise.
Acknowledgements
Supported by National Institute on Aging (R01-AG-24296), Oklahoma Center for Advancement of Science and Technology (HR09-035), from National Center for Research Resources (M01-RR-14467), and from an endowed chair in aging research through the Reynolds Oklahoma Center on Aging. We have no disclosures.
References
- de Souza Moreira B, Sampaio RF, Cavalcanti Furtado SR, Dias RC, Kirkwood RN (2015) The Relationship between Diabetes Mellitus, Geriatric Syndromes, Physical Function, and Gait: A Review of the Literature. Current Diabetes Reviews.
- International Diabetes Federation (2015) I D F Diabetes Atlas, 7th Edition. 1-144.
- American Diabetes Association (2014) Diagnosis and classification of diabetes mellitus. Diabetes Care.37 Suppl 1S81-90.
- Womack CJ, Sieminski DJ, Katzel LI, Yataco A, Gardner AW (1997) Oxygen uptake during constant-intensity exercise in patients with peripheral arterial occlusive disease. Vasc Med 2(3): 174-178.
- Crowther RG, Spinks WL, Leicht AS, Quigley F, Golledge J (2007) Relationship between temporal-spatial gait parameters, gait kinematics, walking performance, exercise capacity, and physical activity level in peripheral arterial disease. J Vasc Surg 45(6): 1172-1178.
- Gardner AW, Forrester L, Smith GV (2001) Altered gait profile in subjects with peripheral arterial disease. Vasc Med 6(1): 31-34.
- Scherer SA, Bainbridge JS, Hiatt WR, Regensteiner JG (1998) Gait characteristics of patients with claudication. Arch Phys Med Rehabil 79(5): 529-531.
- Roman de Mettelinge T, Cambier D, Calders P, Van Den Noortgate N, Delbaere K(2013) Understanding the relationship between type 2 diabetes mellitus and falls in older adults: a prospective cohort study. PLoS One 8(6): e67055.
- Roman de Mettelinge T, Delbaere K, Calders P, Gysel T, Van Den Noortgate N, et al. (2013) The impact of peripheral neuropathy and cognitive decrements on gait in older adults with type 2 diabetes mellitus. Arch Phys Med Rehabil 94(6): 1074-1079.
- Brach JS, Talkowski JB, Strotmeyer ES, Newman AB (2008) Diabetes mellitus and gait dysfunction: possible explanatory factors. Phys Ther 88(11): 1365-1374.
- Ozdirenc M, Biberoglu S, Ozcan A (2003) Evaluation of physical fitness in patients with Type 2 diabetes mellitus. Diabetes Res Clin Pract 60(3): 171-176.
- Expert Panel on the Identification Evaluation and Treatment of Overweight and Obesity in Adults (1998) Executive summary of the clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. Arch Intern Med 158(17): 1855-1867.
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, et al. (2003) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 289(19): 2560-2572.
- Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol In Adults (2002) Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation.106(25): 3143-3421.
- Gardner AW, Killewich LA, Katzel LI, Womack CJ, Montgomery PS, et al. (1999) Relationship between free-living daily physical activity and peripheral circulation in patients with intermittent claudication. Angiology.50(4): 289-297.
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, et al. (2006) ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 113(11): e463-e654.
- National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39(2): S1-266.
- Dolan NC, Liu K, Criqui MH, Greenland P, Guralnik JM, et al. (2002) Peripheral artery disease, diabetes, and reduced lower extremity functioning. Diabetes Care 25(1): 113-120.
- Linda S Pescatello (2014) ACSM's guidelines for exercise testing and prescription.(9th edn),Lippincott Williams & Wilkins, Philadelphia, PA. 456 .
- Womack CJ, Sieminski DJ, Katzel LI, Yataco A, Gardner AW (1997) Improved walking economy in patients with peripheral arterial occlusive disease. Med Sci Sports Exerc 29(10): 1286-1290.
- Regensteiner JG, Bauer TA, Reusch JE, Brandenburg SL, Sippel JM, et al. (1998) Abnormal oxygen uptake kinetic responses in women with type II diabetes mellitus. J Appl Physiol 85(1): 310-317.
- Tzemos N, Lim PO, MacDonald TM (2002) Is exercise blood pressure a marker of vascular endothelial function? QJM 95(7): 423-429.
- Baccelli G, Reggiani P, Mattioli A, Corbellini E, Garducci S, et al. (1999) The exercise pressor reflex and changes in radial arterial pressure and heart rate during walking in patients with arteriosclerosis obliterans. Angiology 50(5): 361-374.
- Shinohara M, Moritani T (1992) Increase in neuromuscular activity and oxygen uptake during heavy exercise. Ann Physiol Anthropol 11(3): 257-262.
- Vollestad NK, Wesche J, Sejersted OM (1990) Gradual increase in leg oxygen uptake during repeated submaximal contractions in humans. J Appl Physiol 68(3): 1150-1156.
- England JD, Regensteiner JG, Ringel SP, Carry MR, Hiatt WR (1992) Muscle denervation in peripheral arterial disease. Neurology 42(5): 99s4-999.
- Chiles NS, Phillips CL, Volpato S, Bandinelli S, Ferrucci L, et al. (2014) Diabetes, peripheral neuropathy, and lower-extremity function. J Diabetes Complications 28(1): 91-95.
- Sawacha Z, Spolaor F, Guarneri G, Contessa P, Carraro E, et al. (2012) Abnormal muscle activation during gait in diabetes patients with and without neuropathy. Gait Posture 35(1): 101-105.
- Petrofsky J, Lee S, Bweir S (2005) Gait characteristics in people with type 2 diabetes mellitus. Eur J Appl Physiol 93(5-6): 640-647.
- Yavuzer G, Yetkin I, Toruner FB, Koca N, Bolukbasi N (2006) Gait deviations of patients with diabetes mellitus: looking beyond peripheral neuropathy. Europa medicophysica 42(2): 127-133.





