Application of Premixed Insulin NovoMix®30 and NovoRapid® as Multiple Daily Injections or as Basal Bolus Format in Selected Diabetic Patients: Practical Evidence from Prospective Case Series
Aziz KMA*
Consultant Diabetologist, Research Scientist (Diabetes, Endocrinology and Metabolism), Aseer Diabetes Center of Aseer Central Hospital, Ministry of Health, Abha, Saudi Arabia.
*Corresponding Author
Kamran Mahmood Ahmed Aziz,
Consultant Diabetologist, Research Scientist (Diabetes, Endocrinology and Metabolism),
Aseer Diabetes Center of Aseer Central Hospital, Ministry of Health,
P. O. Box 34, Abha, Saudi Arabia.
E-mail: drkamran9999@yahoo.com
Received: May 03, 2017; Published: May 08, 2017
Citation: Aziz KMA (2017) Application of Premixed Insulin NovoMix®30 and NovoRapid® as Multiple Daily Injections or as Basal Bolus Format in Selected Diabetic Patients: Technical Evidence from Prospective Case Series. Int J Diabetol Vasc Dis Res,. 5(2e), 1-2. doi: dx.doi.org/10.19070/2328-353X-1700013e
Copyright: Aziz KMA© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Managing type-1 or type-2 diabetes by insulin is one of the best techniques, especially for type-2 diabetics after oral hypoglycemic agents (OHAs) failure. Multiple daily injections (MDI) or basal bolus methodology is an ideal regimen for type-1 diabetics [1, 2]. However, it is a difficult option for type-2 diabetic patients, especially older age groups. Most of type-2 diabetics usually prefer two injections per day, in the morning and evening. Analog premixed biphasic insulins include NovoMix® 30, Humalog Mix® 25 and Humalog Mix® 50. These insulin analogs are also recommended because of their safety and efficacy as compared to older or traditional insulins (Human Regular Insulin such as Humulin® R and Actrapid®, neutral protamine Hagedorn or NPH and their mixtures of premixed human insulin 30/70), which are associated with more frequent hypoglycemia. Safety and efficacy of insulin analogs have also been demonstrated during Ramadan fasting [3]. Basal insulin analogs include glargine (Lantus®), detemir (Levemir®) and degludec (Tresiba®); bolus or mealtime insulins analogs, also called rapid acting insulin analogs (RAIs), are aspart (NovoRapid®), Lispro (Humalog®) and glulisine (Apidra®). Furthermore, basal bolus insulin regimen is ideal and best fits for type-1 diabetics, and should be prescribed to them [4-8].
In the last decades, there has been increasing preference for Premixed Biphasic Insulin Analogs. However, also it has been observed that physicians are now prescribing premixed insulin three times a day (after failure to achieve glycemic targets twice daily injections). Some of limited trials were also conducted to demonstrate that premixed biphasic insulin analogs and NovoMix® 30 three times as day achieved a good glycemic control [9, 10]. It should be mentioned here that such technique is not standard one, however. This technique will be applicable to the limited number of patients. Patients with advanced age, erratic meal pattern, compromised renal failure, chronic renal disease (CRD) or advanced renal disease/end stage renal disease (ESRD) will not benefit from such insulin regimen and can experience severe hypoglycemia. According to our last ten years of clinical practice, 30-40% of such patients usually experience hypoglycemia, especially in the evening or late night. We have also recently published such cases, where three injections of premixed insulin analogs (Humalog® Mix 25 and Humalog® Mix 50) were associated with evening or late night hypoglycemia and described a new method of prescribing premixed insulin analogs in the morning and evening (before the breakfast and dinner) and giving a third injection of RAIs at lunch, instead of prescribing premixed insulin three times a day [11]. Hence, in this way, Premixed or biphasic insulin analogs can be used in basal bolus format, when basal bolus insulin regimen itself becomes difficult (4-5 injections per day) for type-2 diabetic patients, especially elderly subjects.
In this paper, we are also presenting a new regimen of managing diabetes by insulin injections, and case series, where premixed biphasic insulin analogs with one injection of RAIs at lunch can manage uncontrolled diabetes successfully. We selected 35 patients who were difficult to control, with High HbA1c, demonstrating frequent hypoglycemia and fasting hyperglycemia. This was approved by the research committee of Aseer Diabetes Center and the study protocols were according to Declaration of Helsinki (DoH). Table-1 shows characteristics of 35 patients which were uncontrolled on three injections of NovoMix® 30, and these patients were experiencing hypoglycemia, especially evening time, after dinner or late night. Self-monitoring of blood glucose was given to such patients to detect hypoglycemia severity and it's timings. In spite of hypoglycemia, their HbA1c was high (because of hypoglycemia and over eating). Increase weight was an additional finding. Additionally, all of these patients presented with fasting hyperglycemia, an observation explained by Somogyi effect/phenomenon [12-14].
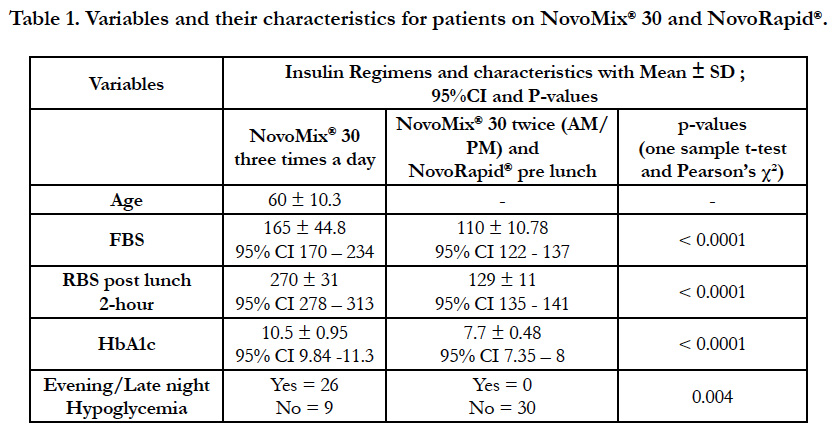

Table 1. Variables and their characteristics for patients on NovoMix 30 and NovoRapid.s
It can be observed in the table-1 that most of the patients were elderly (Mean age 60 ± 10.3) who were uncontrolled, experienced hypoglycemic events, high fasting blood sugar (FBS) and two hour post lunch Random blood sugar (RBS). Some of the patients even reached up to values of 300 mg/dl. Patients were counseled and shifted to NovoMix® 30 two times daily,before five minutes of breakfast (AM) and dinner (PM); pre-lunch NovoRapid® was prescribed (5 minutes before the meal). Extensive education, dose adjustments and self-monitoring of blood glucose (SMBG) was given to all of these patients. Within 2-3 months, patients were followed up in the clinic and demonstrated significant improvement with FBS reductions (165 ± 44.8 versus 110 ± 10.78; p-value <0.0001), post lunch RBS reductions (270 ± 31 versus 129 ± 11 ; p-value < 0.0001), HbA1c reductions (10.5 ± 0.95 versus 7.7 ± 0.48; p-value <0.0001) and total reductions in hypoglycemia events (Pearson's χ² p-value 0.004).
Learning objectives from these case series are that basal bolus format is the ideal choice for type-1 diabetics (4-5 injections/day). However, it is difficult for type-2 patients of older age. Instead of prescribing premixed NovoMix® 30 (or Humalog® Mix 25/Humalog® Mix 50) three times a day, these subjects can be managed better with premixed insulins twice a day (AM and PM) and a third injection of NovoRapid® (or any RAIs) pre lunch, which is also an easy option. Hence, premixed insulin used in such a way mimics MDI or basal bolus format regimens and can be used in out-patient diabetology clinics. Insulin Analogs (RAIs and long acting) currently remains the best way to manage diabetes by insulin injections [15-20].
References
- Kamran MA Aziz (2012) Management of Type-1 and Type-2 Diabetes by Insulin Injections in Diabetology Clinics-A Scientific Research Review. Recent Pat Endocr Metab Immune Drug Discov. 6(2): 148-170.
- Zinman B (1989) The physiologic replacement of insulin. N Engl J Med. 321(6): 363-370.
- Kamran MA Aziz (2013) Effect of Fasting Ramadan in Diabetes Control Status - Application of Extensive Diabetes Education, Serum Creatinine with HbA1c Statistical ANOVA and Regression Models to Prevent Hypoglycemia. Recent Pat Endocr Metab Immune Drug Discov 7(3): 233-251.
- Holcombe JH, Zalani S, Arora VK, Mast CJ (2002) Comparison of insulin lispro with regular human insulin for the treatment of type 1 diabetes in adolescents. Clin Ther. 24(4): 629-638.
- Heinemann L, Heise T, Jorgensen LN, Starke AA (1993) Action profile of the rapid acting insulin analogue: Human insulin B28Asp. Diabet Med. 10(6): 535-539.
- Olsen HB, Kjeldsen TB, Balschmidt P, Glendorf T, Havelund S (2011) Rapid acting insulin analogues.
- NICE (National Institute of Clinical Excellence) (2002) Guidance on the use of long-acting insulin analogs for the treatment of diabetes-insulin glargine. Technology Appraisal Guidance.
- Robenstock J, Park G, Zimmerman J (2000) Basal insulin glargine (HOE 901) versus NPH insulin in patients with type 1 diabetes on multiple daily insulin regimens. Diabetes Care. 23(8): 1137-1142.
- Garber AJ, Wahlen J, Wahl T, Blesser P, Allen E, et al., (2006) Attainment of glycemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30 (the 1-2-3 study). Diabetes Obesity Metab. 8(1): 58–66.
- Farcasiu E, Ivanyi T, Mozejko-Pastewka B, Birkus Z, Csog J, et al., (2011) Efficacy and safety of prandial premixed therapy using insulin lispro mix 50/50 3 times daily compared with progressive titration of insulin lispro mix 75/25 or biphasic insulin aspart 70/30 twice daily in patients with type 2 diabetes mellitus: a randomized, 16-week, open-label study. Clin Ther. 33(11): 1682-93. doi: 10.1016/j.clinthera.2011.10.00.
- Aziz KMA (2017) Using Premixed Biphasic Insulin Analogs Humalog® Mix 25 and Humalog® Mix 50 in Basal Bolus Format: Evidence from Research, Clinical Practice and Case Reports. J Diabetes Metab Disord Control. 4(3): 00114. DOI: 10.15406/jdmdc.2017.04.00114.
- Somogyi M (1938) Insulin as a cause of extreme hyperglycemia and instability. Bull St Louis Med Soc. 32: 498-500.
- Raskin P (1984) The Somogyi phenomenon. Sacred cow or bull? Arch Intern Med. 144(4): 781-787.
- Choudhary P, Davies C, Emery CJ, Heller SR (2013) Do high fasting glucose levels suggest nocturnal hypoglycaemia? The Somogyi effect-more fiction than fact? Diabet Med. 30(8): 914-917.
- Dall V (1999) Preclinical safety pharmacology studies on the rapid-acting insulin analogue, insulin aspart. Artzneim Forsch Drug Res. 49(5): 463-470.
- Heise T, Nosek L, Ronn BB, Endahl L, Heinemann L, et al., (2004) Lower within-subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes. Diabetes. 53(6): 1614-1620.
- Hermansen K, Fontaine P, Kukolja KK, Peterkova V, Leth G, et al., (2004) Insulin analogs (insulin detemir and insulin aspart) versus traditional human insulins (NPH insulin and regular human insulin) in basal-bolus therapy for patients with type 1 diabetes. Diabetologia 47(4): 622-629.
- Seipke G, Geisen K, Neubauer HP, Pittius C, Rosskamp R, et al., (1992) New insulin preparations with prolonged action profiles: A21-modified arginine insulin. Diabetologia 35(Suppl1): A4-A5.
- Heineman L, Linkescowa R, Rave K, Hompesh B, Sedlak M, et al., (2000) Time-action profile of the long acting insulin analog glargine (HOE 901) in comparison with those of NPH insulin and placebo. Diabetes Care. 23(5): 644-649.
- American Diabetes Association (2017) Standards of Medical Care in Diabetes. Diabetes Care. 40(Suppl 1): S1-S135.





