The Risk of Subsequent Amputation Following An Initial Lower Extremity Amputation: A Systematic Review
Wong CK1*, Stern JR2, Rick F D’Andrea Jr3, Loven SL3, Panjaki S4, See AS3, Spindler SJ3, Yerovinkina M3, Nowygrod R2
1 Department of Rehabilitation and Regenerative Medicine, Columbia University Medical Center, Neurological Institute, New York, NY, USA.
2 Department of Surgery, New York Presbyterian Hospital, Herbert Irving Pavilion, New York, NY, USA.
3 Program in Physical Therapy, Columbia University, Neurological Institute, NY, USA.
*Corresponding Author
Christopher Kevin Wong, PT, PhD,
Department of Rehabilitation and Regenerative Medicine,
Columbia University Medical Center, 710 West 168th Street, Neurological Institute 8-822, New York, NY, USA.
Tel: 01-212-305-3781/ 01-914-738-9276
Fax: 01-212-305-4569
E-mail: ckw7@cumc.columbia.edu
Received: July 27, 2016; Accepted: October 26, 2016; Published: October 27, 2016
Citation: Wong CK, Stern JR, Rick F D’Andrea Jr, Loven SL, Panjaki S, et al., (2016) The Risk of Subsequent Amputation Following An Initial Lower Extremity Amputation: A Systematic Review. Int J Diabetol Vasc Dis Res,. 4(5), 171-177. doi: dx.doi.org/10.19070/2328-353X-1600036
Copyright: Wong CK © 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: Quantifying subsequent amputation incidence after an initial amputation, whether affecting the ipsilateral or contralateral lower extremity, may enhance decision-making regarding risk reduction. This systematic review sought to determine reamputation risk in patients with vascular disease including diabetes.
Methods: Four databases were searched from January 2005 through July 2015. Reviewers screened articles for inclusion criteria: cohort studies, >80% participants with initial amputations due to vascular disease including diabetes, >100 participants. Articles were excluded when >20% of the initial amputations were due to trauma or >5% were due to cancer. Final article inclusion was approved by reviewer consensus. Bias was assessed with the Joanna Briggs Institute Critical Appraisal Tool for cohort studies.
Results: Of 365 unique records screened, 43 abstracts reviewed, and 21 full articles reviewed, 15 articles were included. Subsequent amputation was most common in the first year after initial amputation with the rates 13.9% ipsilateral and 7.2% contralateral. Specific risk factors included combined diabetes and peripheral artery disease, renal failure, and coronary disease.
Conclusion: The rate of subsequent amputation after primary lower limb amputation is substantial but appears lower than in past decades. Awareness of the problem and potential risk factors may impact clinical decisions regarding patient education and prevention.
2.Introduction
3.Review Methods
3.1.Search Strategy and Screening
3.2.Data Extraction and Synthesis
3.3.Methodological Quality and GRADE of the Evidence
4.Results
4.1.Included Studies
4.2.Subsequent Amputations
4.3.Risk Factors
4.4.Bias Assessment
4.5.Quality of the Evidence
5.Discussion
5.1.Limitations
6.Conclusions
7.References
Key Words
Vascular Disease; Diabetes; Outcome; Reoperation; Contralateral; Artificial Limb.
Introduction
The prevalence of lower limb loss in the USA was 1.5 million in 2005 and expected to double by 2050 [1]. Approximately 185,000 amputations occur each year [2]. While amputation rates due to traumatic events or cancer are decreasing, the incidence of amputation related to diabetes and peripheral artery disease is increasing [3]. The primary cause of lower limb amputations [1], vascular disorders such as diabetes and peripheral artery disease are progressive and affect both limbs making subsequent amputation of the ipsilateral or contralateral limb not uncommon [4]. People with diabetes are especially vulnerable with nearly double the risk of losing the contralateral limb after a first amputation [4].
Subsequent amputations, either ipsilateral extremity re-amputation to a higher level or contralateral extremity amputation of any level, can substantially impact the individual’s functional ability to access the community and participate in the activities that contribute to quality of life. Loss of the contralateral lower extremity may necessitate bilateral prosthetic limbs to walk, requiring increased energy expenditure that severely curtails functional ability [5,6]. People using at least one prosthetic knee have the poorest functional outcomes [7], especially when negotiating stairs [8]. Successively higher amputation correlates with weaker hip extension and lower functional mobility [9]. Subsequent ipsilateral extremity reamputation can mean the person must now control a prosthetic knee which carries great physiologic and functional costs even for people with unilateral amputations [10].
In one study of over 5000 patients using the American College of Surgeons National Surgical Quality Improvement Program database, 4% of patients undergoing amputation returned to the operating room for revision or reamputation within the original hospital stay, with 70% readmission within 30 days of surgery [11]. In another study of over 1700 patients undergoing amputation for any reason, 10% had major ipsilateral extremity reamputation after 1 year [12]. Reamputation risk appears greater after partial foot amputation, as nearly two thirds of limbs undergoing transmetatarsal amputation may require reamputation to a more proximal level [13]. The contralateral extremity is at risk for subsequent amputation as well, though incidence rates of contralateral major amputation appear less than for ipsilateral reamputation: 5.7% at 1 year and 11.5% at 5 years [12]. However, a rate of 35.4% in 5 years has also been reported [14].
The purpose of this systematic review was to quantify the rate of subsequent ipsilateral and contralateral amputation for patients with lower extremity amputations due to vascular disease including diabetes. The secondary aim was to identify specific risk factors associated with subsequent amputation.
Review Methods
This systematic review utilized a study protocol following Cochrane Collaboration recommendations, with the process reported per the PRISMA statement for reviews that evaluate healthcare interventions [15, 16].
Inclusion criteria included: a) Cohort study designs, published since January 2005, with follow-up >3 months. b) Participant samples that included >100 initial amputations, with >80% of amputations associated with vascular disease including diabetes. c) Outcomes that included subsequent amputations defined as ipsilateral reamputation or contralateral amputation. Exclusion criteria included: a) Interventional studies, whether single group or randomized control trials, and those not written in the English language. b) Participant samples limited to nonvascular amputations and with >20% participants with traumarelated amputations. c) Outcomes limited to reoperation/revision without a more proximal secondary amputation.
The following databases were searched to identify related systematic reviews and studies: Cochrane, Embase, and OVID MEDLINE. Searches were restricted to English language articles published since January 2005. The search strategy was based on Boolean operator combinations of MeSH terms and keywords including “amputation,” “lower extremity,” “reoperation,” and “contralateral.” Citations of included articles were added to the search. After removing duplicates, three pairs of reviewers screened potential studies by title for relevance, then abstract for inclusion and exclusion criteria. Each reader screened every paper using a study eligibility form; eligibility was determined by consensus of the reviewer pair, with all six reviewers available in case of disagreement. Articles eligible after the initial screening underwent full-text review with inclusion based on consensus discussion.
Reviewer pairs extracted all data for the included articles using a customized data checklist for sample size, demographics, study type, location, incidence of subsequent ipsilateral or contralateral amputations, and risk factors with odds ratios, risk ratios, or hazard ratios, combined with bias assessment using the Joanna Briggs Institute Critical Appraisal Tool for cohort studies [17]. Quantitative synthesis of incidence rates for subsequent amputation, both contralateral and ipsilateral, was performed. A person-first approach was taken to data synthesis with patients rather than amputation procedures counted. A qualitative analysis of risk factors that substantially change the odds of subsequent amputation involved compiling risk factors with odds ratios, risk ratios, or hazard ratios > 2.0 or < 0.5.
The Joanna Briggs Institute Critical Appraisal Tool for potential study bias consists of ten domains that address relevance to the target population, appropriate data analysis, description of the setting, and identification of confounding factors [17]. Risk of bias in each domain was assessed as high, low, or unclear (when reporting left unclear whether specific potential biases had been addressed). All studies were individual cohort studies and were rated 3 according to the 2011 Center for Evidence Based Medicine Levels of Evidence Rating Scale, though each study could be downgraded based on study biases [15]. Overall quality of the evidence was assessed using the Cochrane GRADE system as high-, moderate-, low-, or very low-quality based on the combined studies level of evidence and potential bias in five domains: study design, indirectness of the evidence, unexplained study heterogeneity or inconsistency, imprecise results, and probability of publication bias [15].
Results
The search strategy yielded 365 unique citations screened for eligibility, after duplicates were removed. As of July 2015, no systematic reviews had quantified the incidence of reamputation after primary lower extremity amputation. Screening by title and abstract excluded 344 articles for relevance, leaving 21 for full-text review. Another 6 articles were excluded (see Figure 1) because they lacked relevant statistics, did not meet inclusion criteria, or in one case used the same data set as another included study. Thus, data were compiled from 15 mostly retrospective cohort studies, including both single and multiple hospital settings from various countries (Table 1).
The combined studies summarize the experiences of 9,711 participants. Study cohorts ranged from 116 to 3,555 participants with average ages ranging from 53.8 to 78.9 years. Participants in all but 2 studies were predominantly male, and most studies reported a majority of participants with diabetes. Weighted values were calculated to account for variations in sample size. The combined sample averaged 64.4 years of age, 54.8% were men, and 72.9% had diabetes. In the 4 United States studies that reported race, 32.6% of participants were non-white. The initial amputation levels included both minor (partial foot and ankle) and major lower extremity amputations (above ankle) (Table 2).
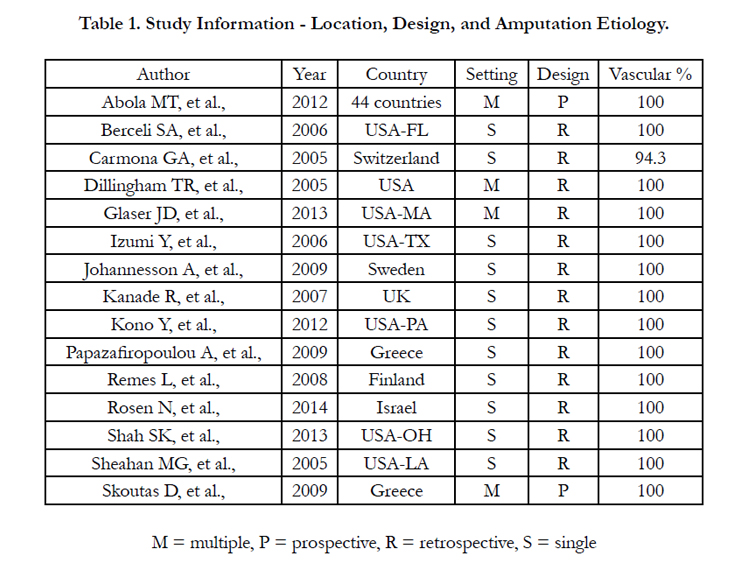

Table 1. Study Information - Location, Design, and Amputation Etiology.
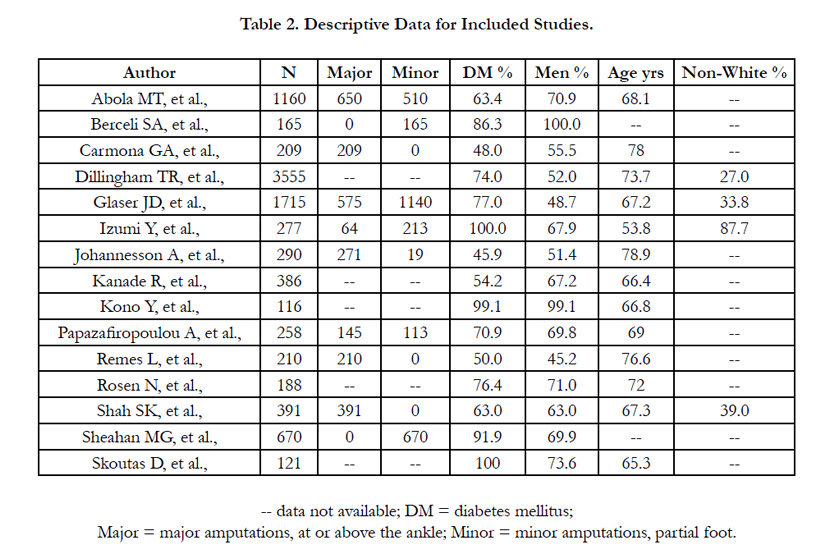
Table 2. Descriptive Data for Included Studies.
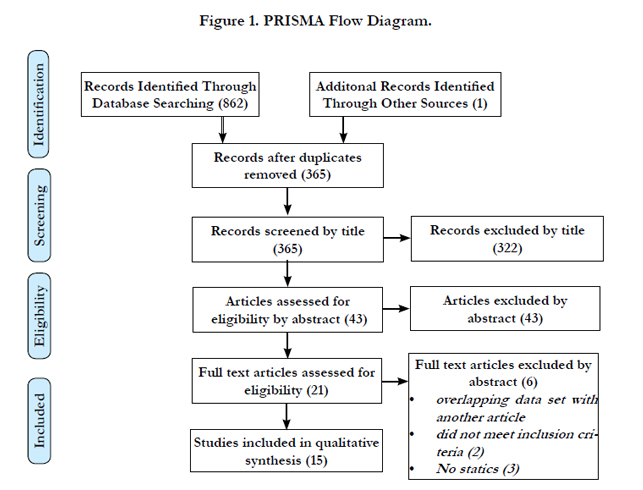

Figure 1. PRISMA Flow Diagram.
Of the 15 included studies, 14 reported the incidence of subsequent ipsilateral amputation and 9 reported the incidence of subsequent contralateral amputation. The overall weighted average incidence of subsequent amputation, whether ipsilateral or contralateral, was 23.7%. Specifically, the overall weighted rate of subsequent amputation was 16.1% for the ipsilateral and 7.9% for the contralateral extremity. Methodologies and reporting style varied among studies, but follow-up at 1, 3, and 5 years for ipsilateral and 1 and 5 years for contralateral were most common. Follow-up for 2-3 years are reported together under 3-year followup, and for 4-5 years are reported together under 5-year followup. The rate of subsequent ipsilateral amputation was 13.9% at 1 year, 19.8% at 2-3 years, and 15.6% at 4-5 years. The rate of subsequent contralateral amputation was 7.2% at 1 year, 17.7% at 2-3 years, and 11.4% at 5 years (Table 3).
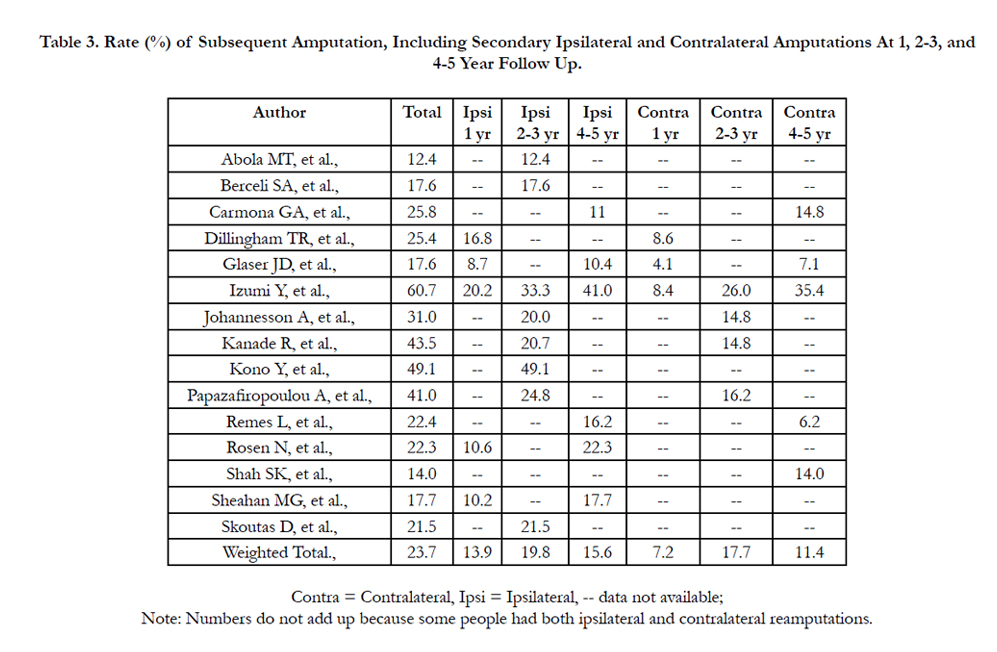
Table 3. Rate (%) of Subsequent Amputation, Including Secondary Ipsilateral and Contralateral Amputations At 1, 2-3, and 4-5 Year Follow Up.
Diabetes was a significant risk factor for subsequent amputation with odds or hazard ratios ranging from 2.9 to 3.7 [12, 18, 19]. Diabetes in combination with peripheral artery disease had a hazard ratio of 9.1 for subsequent amputation [12]. Other risk factors identified within various predictive models included chronic renal insufficiency (HR=2.2), end stage renal disease (HR=3.9), peripheral artery disease (HR=2.9) [12], amputation within past year (OR=2.6)[18], gangrene upon admission (OR=3.8), coronary artery disease (OR=2.3), prolonged antibiotic use >2 weeks after amputation (OR=2.3, HR=3.1) [19,20], and heel lesions (2.6=HR) [21]. Subsequent bypass surgery (OR=2.1) [22], dialysis (HR=2.42) [23], and discharge to intermediate or long-term care (HR=2.45, 5.34) also carried greater risk [24]. Among the 3 studies [23-25] reporting data only after primary major amputations (N=810) and the 2 studies [22, 26] reporting data only after primary minor amputations (N=835) the rate of subsequent amputation combining ipsilateral and contralateral amputations was 17.6% and 17.7% for major and minor amputations, respectively.
Low risk of bias was apparent in most domains for the combined studies (Figure 2). Potential for bias exists for some studies with respect to representing the target population: only 3 of 13 articles [24, 27, 28] used multi-center data. The remaining articles came from single institutions and had smaller sample populations. Two articles did not specify from what setting or location the data originated [20, 21].
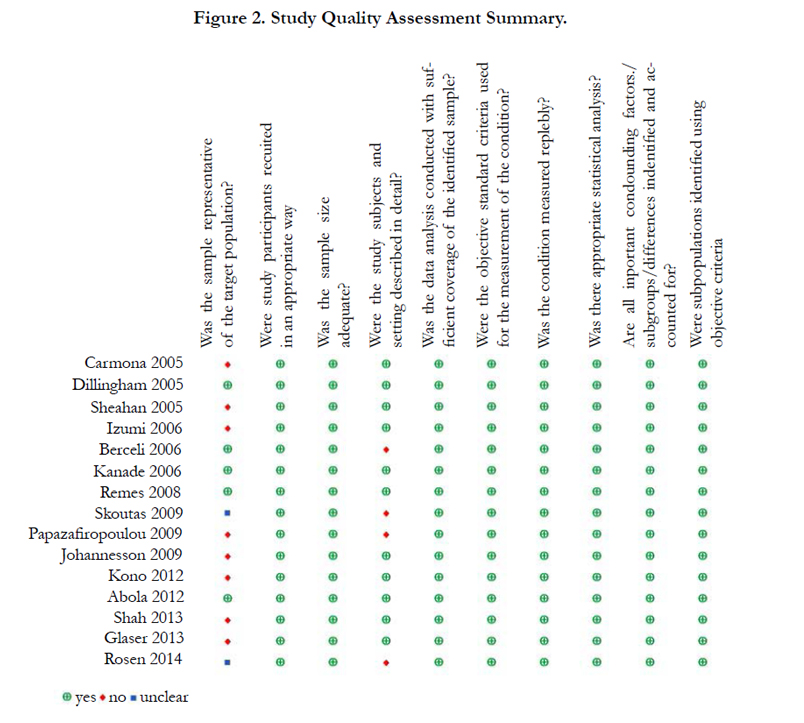
Figure 2. Study Quality Assessment Summary.
Since all 15 articles were cohort studies they were given a Level of 3 according to the 2011 Center for Evidence Based Medicine Levels of Evidence Rating Scale. Three articles were upgraded to 3+ due to large sample sizes [12, 18, 27]; three were downgraded to 3- due to small sample sizes and vague descriptions of the setting [19, 20, 29]. Overall, the quality of the combined body of evidence for these 15 papers was moderate.
Discussion
Lower extremity amputation is a significant life-altering event, and amputation rates in people with diabetes and peripheral artery disease are increasing [27]. The 15 studies included in this systematic review were an international selection that varied in outcomes and other characteristics and focused on patients with amputations associated with vascular disease including diabetes, a very high-risk population among whom over one-third die within the first year following amputation, and approximately half die within five years [12]. Reamputation in this population often lead to further disability and loss of independence. The goal of this study was to systematically quantify rates of reamputation and identify risk factors across multiple studies, so that people at risk can be potentially identified early.
The overall reamputation risk from the synthesized data reported within the past 11 years was 23.7%, which was substantially lower than the 28-51% 5-year reamputation rate reported by the Amputation Coalition of America, which cites 1995 NIH data [30]. The reasons for different rates of reamputation between decades remains unknown and is likely multi-factorial, but advancements in medical therapy including newer diabetic agents and HMG-CoA inhibitors (statins) as well as more aggressive use of endovascular procedures in the tibial vessels to maximize perfusion may have contributed [31].
The ipsilateral reamputation rate in the current review was less than but similar to data published in 1980 [32], however the contralateral amputation rate was much lower. Ipsilateral reamputation ranged from 10% to 49%, with an overall weighted risk of 16.1%. In long-term follow-up, the rate of subsequent ipsilateral amputation was 13.9% at 1 year, 19.8% at 2-3 years, and 15.6% at 4-5 years. It is important to note, however, that 2 of the 3 largest studies (with 4715 patients representing almost 50% of the total sample) did not report data out to 4-5 years [18, 27]. Limited reported 5-year data may also explain the paradoxically lower contralateral and total reamputation rates when comparing data at 4-5 years to 2-3 years. While the total reamputation rate in specific studies with 5-year follow-up data ranged from 17.6% [12] to 60.7% [14], the combined data included studies with only 1-year follow-up and may thus underestimate overall reamputation risk.
Most ipsilateral reamputations occurred within the first year after the index amputation. Overall, the combined data demonstrated no greater reamputation risk after minor index amputation than after major amputation [12, 18]. However, in one study of 277 participants, minor index amputations corresponded more closely with subsequent ipsilateral amputations than did major index amputations [14]. Aggressive limb salvage attempts can lead to lower level amputations which are less than ideal, but have some chance of healing. Patients may favor a lower amputation to preserve function, even given a high likelihood of failure and need for subsequent reamputation to the appropriate level after which the result can be durable [14]. Variations in surgical practice, outcome reporting, and procedural coding, may obfuscate the rate of subsequent amputations occurring after minor amputations.
The risk of contralateral amputation remains relatively constant over time. These amputations are more reflective of a general progression of the underlying disease, and thus the risk does not diminish. A contralateral amputation of the remaining limb poses a significant threat for patients with prior lower extremity amputation. After a unilateral amputation, the remaining limb is heavily relied upon for walking and daily activities [33]. The weighted risk of contralateral reamputation was 7.9% in this review, again substantially lower than data from the Amputation Coalition of America that reported a contralateral amputation rate of 55% within two to three years of the initial amputation [30]. Specifically, the rate of subsequent contralateral amputation in the current review was 7.2% at 1 year and 17.7% at 2-3 years. The lower rate compared to reports from past decades [30] may be attributed to improved limb loss prevention efforts. Additionally, people with minor index amputations had heightened risk of receiving contralateral amputations when compared to those having an initial major amputations [27]. While all patients with amputations generally favor the remaining limb [33], those with minor amputations are presumably more ambulatory initially than patients with major amputations, and therefore may use the contralateral limb more heavily.
Subsequent amputations occurred more frequently in diabetic patients than in non-diabetics [34, 35]. In one study, nearly half (45.9%) of participants with diabetes underwent subsequent amputation [28]. In another, patients with diabetes had higher ipsilateral amputation rates (29.7% vs 12.7%), as well as contralateral amputation (19.9% vs 7.1%) when compared to their non-diabetic counterparts [29]. These findings reinforce the high-risk nature of the diabetic cohort and the need for wound care and early referral for limb salvage surgery when signs of malperfusion initially present. When a patient with diabetes requires amputation, it can often be the first of several.
Several additional co-morbid conditions were identified as risk factors for reamputation. The most significant was renal insufficiency/end stage renal disease, followed by peripheral artery disease, amputation within the past year, presence of gangrene upon admission, and coronary artery disease. These conditions often present in the diabetic or peripheral arterial disease patient populations [36]. Identifying patients with risk factors associated with reamputation at the time of index amputation could prompt increased patient education, monitoring, and rehabilitation efforts that may aid in the prevention of reamputation and its associated morbidity in the future.
The findings in this review were limited by variations in data reporting: the initial amputation level, amputation side and limb dominance, and multiplicity of subsequent amputations were not always defined. Follow-up time did not include the initial 3-month post-operative period and varied within and among studies. Socio-economic risk factors including income and race were not included and medical risk factors were not consistently defined or reported preventing quantitative synthesis. Some studies did not report basic demographic data. Inter-rater reliability of reviewer data extraction was not assessed. In addition, while the search terms selected resulted in nearly 1,000 articles, relevant articles may have been missed due to narrow search parameters.
Conclusions
This systematic review quantifies the reamputation risk as reported in current literature, which was substantially lower than the risk reported in past decades. Those patients requiring amputation secondary to diabetes and/or peripheral artery disease, however, continue to be at high risk. The presence of comorbidities typical of this cohort, namely renal and cardiac disease, appears to independently confer additional risk for reamputation. These patients should be counseled early and appropriate steps taken to educate and prevent this outcome.
References
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Brookmeyer R (2008) Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 89(3): 422-429.
- Owings MF, Kozak LJ (1998) Ambulatory and inpatient procedures in the United States, 1996. National Center for Health Statistics. Vital Health Stat. 13(139).
- Dillingham TR, Pezzin LE, MacKenzie EJ (2002) Limb amputation and limb deficiency: epidemiology and recent trends in the United States. South Med J. 95(8): 875-883.
- Schofield CJ, Libby G, Brennan GM, MacAlpine RR, Morris AD, et al., (2006) Mortality and hospitalization in patients after amputation. Diabet Care. 29(10): 2252-2256.
- Bhangu S, Devlin M, Pauley T (2009) Outcomes of individuals with transfemoral and contralateral transtibial amputation due to dysvascular etiologies. Prosthet Orthot Int. 33(1): 33-40.
- Wright DA, Marks L, Payne RC (2008) A comparative study of the physiological costs of walking in ten bilateral amputees. Prosthet Orthot Int. 32(1): 57-67.
- Karmarkar AM, Graham JE, ReistetterTA, et al., (2014) Association between functional severity and amputation type with rehabilitation outcomes in patients with lower limb amputation. Rehabil Res Pract. 2014: 961798.
- Ebrahimzadeh MH, Moradi A, Bozorgnia S, Hallaj-Moghaddam M (2016) Evaluation of disabilities and activities of daily living of war-related bilateral lower extremity amputees. Prosthet Orthot Int. 40(1): 51-57.
- Raya MA, Gailey RS, Fiebert IM, RoachKE (2010) Impairment variables predicting activity limitation in individuals with lower limb amputation. Prosthet Orthot Int. 34(1): 73-84.
- Hoffman MD, Sheldahl LM, Buley KJ, Sandford PR (1997) Physiological comparison of walking among bilateral above-knee amputee and ablebodied subjects, and a model to account for the differences in metabolic cost. Arch Phys Med Rehabil. 78(4): 385-392.
- Curran T, Zhang JQ, Lo RC, Fokkema M, Buck DB, et al., (2014) Risk factors and indications for admission after lower extremity amputation in the American College of Surgeons National Surgical Quality Improvement Program. J Vasc Surg. 60(5): 1315-1324.
- Glaser JD, Bensley RP, Hurks R, Mark C. Wyers, Chaikof EL, et al., (2013) Fate of the contralateral limb after lower extremity amputation. J Vasc Surg. 58(6): 1571-1577.
- Stone PA, Back MR, Armstrong PA, Keeling WB, Johnson BL, et al., (2005) Midfoot amputations expand limb salvage rates for diabetic foot infections. Ann Vasc Surg. 19(6): 805-811.
- Izumi Y, Satterfield K, Lee S, Harkless LB (2006) Risk of reamputation in diabetic patients stratified by limb and level of amputation: a 10-year observation. Diabet Care. 29(3): 566-570.
- Higgins JPT, Green S (eds) (2011)) Cochrane handbook for systematic reviews of interventions, version 5.1.0. The Cochrane Collaboration: London.
- Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 151(4): 264-269.
- Joanna Briggs Institute (2014) Reviewers’ Manual Appendix V (c) – Critical Appraisal Tool for Descriptive Studies.
- Abola MT, Bhatt DL, Duval S, Cacoub PP, Keo H, et al., (2012) Fate of individuals with ischemic amputations in the REACH Registry: three-year cardiovascular and limb-related outcomes. Atherosclerosis. 221(2): 527-535.
- Kono Y, Muder RR (2012) Identifying the incidence of and risk factors for reamputation among patients who underwent foot amputation. AnnVasc Surg. 26(8): 1120-1126.
- Rosen N, Gigi R, HaimA, Salai M, Chechik O, et al., (2014) Mortality and reoperations following lower limb amputations. Israel Med Assoc J. 16(2): 83-87.
- Skoutas D, Papanas N, Georgiadis GS, Zervas V, Manes C, et al., (2009) Risk factors for ipsilateral reamputation in patients with diabetic foot lesions. Int J Low Extrem Wound. 8(2): 69-74.
- Sheahan MG, Hamdan AD, Veraldi JR, Skillman JJ, Campbell DR, et al., (2005) Lower extremity minor amputations: the roles of diabetes mellitus and timing of revascularization. J Vasc Surg. 42(3): 476-480.
- Shah SK, Bena JF, Allemang MT, Kelso R, Clair DG, et al., (2013) Lower extremity amputations: factors associated with mortality or contralateral amputation. Vasc Endovasc Surg. 47(8): 608-613.
- Remes L, Isoaho R, Vahlberg T, Hiekkanen H, Korhonen K, et al., (2008) Major lower extremity amputation in elderly patients with peripheral arterial disease: incidence and survival rates. Aging Clin Exp Res. 20(5): 385-393.
- Carmona GA, Hoffmeyer P, Herrmann FR, Vaucher J, Lacraz A, et al., (2005) Major lower limb amputations in the elderly observed over ten years: the role of diabetes and peripheral arterial disease. Diabet Metab. 31(5): 449-454.
- Berceli SA, Brown JE, Irwin PB, Ozaki CK, (2006) Clinical outcomes after closed, staged, and open forefoot amputations. J Vasc Surg. 44(2): 347-352.
- Dillingham TR, Pezzin LE, Shore AD (2005) Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 86(3): 480-486.
- Kanade R, Van Deursen R, Burton J, Davies V, Harding K, et al., (2007) Re-amputation occurrence in the diabetic population in South Wales, UK. IntWound J. 4(4): 344-352.
- Papazafiropoulou A, Tentolouris N, Soldatos RP, Liapis CD, Dounis E, et al., (2009) Mortality in diabetic and nondiabetic patients after amputations performed from 1996 to 2005 in a tertiary hospital population: a 3-year follow-up study. J Diabet Complications. 23(1): 7-11.
- Amputee Coalition of America (ACA) Preventing further limb loss among people with diabetes, 2015. [Accessed 2015, Dec 23]. Available at www.amputee-coalition.org/fact_sheets/preventingamp.html.
- Genovese EA, Chaer RA, Taha AG, Marone LK, Baril DT, et al., (2015) Risk factors for long-term mortality and amputation after open and endovascular treatment of acute limb ischemia. Ann Vasc Surg. 30: 82-92.
- Ebskov B, Josephsen P (1980) Incidence of reamputation and death after gangrene of the lower extremity. Prosthet Orthot Int. 4(2): 77-80.
- Gailey R, Allen K, Castles J, Kucharik J, Roeder M (2008) Review of secondary physical conditions associated with lower-limb amputation and longterm prosthesis use. J Rehabil Res Dev. 45(1): 15-29.
- Dillingham TR, Pezzin LE (2008) Rehabilitation setting and associated mortality and medical stability among persons with amputations. Arch Phys Med Rehabil. 89(6): 1038-1045.
- Tentolouris N, Al-Sabbagh S, Walker MG, et al., (2004) Mortality in diabetic and nondiabetic patients after amputations performed from 1990 to 1995: a 5-year follow-up study. Diabet Care. 27(7): 1598-1604.
- Girman CJ, Kou TD, Brodovicz K, Alexander CM, Engel S, et al., (2012) Risk of acute renal failure in patients with Type 2 diabetes mellitus. Diabet Med. 29(5): 614-621





