A Study to Evaluate Association of Celiac Disease with Insulin Dependent Diabetes and Hypothyroidism in North-West Rajasthan
Kumar S1*, Meena SL2, Aswal VK3, Vyas AK4
1 Professor, Department of Medicine, S.P. Medical College, Bikaner, India.
2 Assistant Professor, Department of Medicine, S.P. Medical College, Bikaner, India.
3 Resident, Department of Medicine, S.P. Medical College, Bikaner, India.
4 Consultant Medicine, Jaipur, India.
*Corresponding Author
Dr. Surender Kumar,
Professor, Depart of Medicine, S.P. Medical College,
PBM Hospital Campus, H.No-2, Bikaner, Rajasthan, India.
Tel: +91- 9414604192
E-mail: drsurendrakumar@rediffmail.com
Received: July 15, 2016; Accepted: August 28, 2016; Published: August 31, 2016
Citation: Kumar S, Meena SL, Aswal VK, Vyas AK (2016) A Study to Evaluate Association of Celiac Disease with Insulin Dependent Diabetes and Hypothyroidism in North-West Rajasthan. Int J Diabetol Vasc Dis Res,. 4(3), 162-165.DOI : dx.doi.org/10.19070/2328-353X-1600034
Copyright: Kumar S© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To study association of Celiac Disease with Insulin Dependent Diabetes and Hypothyroidism in young adults in North-Western Rajasthan.
Method: Total eighty-seven newly diagnosed adult patients of celiac disease were included. Sera of all patients were tested for presence of IgA tissue transglutaminase (tTG) antibody by ELISA using commercially available kits. Three to four intestinal mucosal biopsies were obtained with GI endoscopy from the second part of duodenum in patients with presence of tTG antibodies. Fasting blood glucose (FBG) was measured after overnight fasting (8 hours of fasting overnight). Serum TSH testing was performed on automated immunoassay platforms employing advanced IMA technology.
Results: In our study, out of total 87 patients, 46(52.87%) were from serum TTG group 50-200 and 41(47.12%) from serum TTG group >200. Out of total 87 patients, 14 patients had their TSH >4.2 and out of them 12 and 2 patients were from serum TTG group 50-200 and >200 respectively and the difference was statistically significant (p<0.01).15 patients were found with impaired glucose tolerance and out of them 11 and 4 were from serum TTG group 50-200 and >200 respectively. Only 10 patients had their fasting blood sugar >125 and out of them 9 and 1 were from serum TTG group 50-200 and >200 respectively and the difference was found significant (p<0.01).
Conclusion: Our study concludes that there is significant association of CD with thyroid dysfunction and impaired glucose tolerance. All CD patients should be screened for thyroid dysfunction and impaired glucose tolerance. Early recognition of CD and hence early appropriate management may help in reducing severity of various autoimmune disorders, improving quality of life in these patients.
2.Introduction
3.Material and Methods
3.1.Inclusion Criteria
3.2.Exclusion Criteria
4.Results
5.Discussion
6.Conclusion
7.References
Key Words
Celiac Disease; Diabetes; Hypothyroidism.
Introduction
Celiac disease is a permanent intolerance to ingested gluten that results in immunologically mediated inflammatory damage to the small-intestinal mucosa [1]. Classically the patient manifests with diarrhoea. Such classical symptomatic patients represent the tip of the iceberg [2]. Majority of patients of Celiac disease manifest as anaemia, osteoporosis, convulsions, short stature, weight loss, fatigue, generalised weakness, cheliosis, glossitis, dry skin. North India is referred as a “celiac belt”, where a greater than average number of people exhibit symptoms of celiac disease. This is partially because more wheat is consumed in this region, but also because the population possesses haplotypes necessary for celiac disease to develop [3]. The inflammatory process, mediated by T cells, leads to disruption of the structure and function of the small bowel's mucosal lining and causes malabsorption as it impairs the body's ability to absorb nutrients, minerals and fatsoluble vitamins A, D, E and K from food.
Celiac disease is associated with a wide range of autoimmune diseases including insulin-dependent diabetes, dermatitis herpetiformis, autoimmune thyroid disease, autoimmune hepatitis, primary biliary cirrhosis, atrophic gastritis, glutenrelated ataxia and connective tissue diseases. This has been explained by the sharing of certain common genetic factors. It has been recently discovered that the prevalence of autoimmune disorders in celiac disease is related to the duration of exposure to gluten. The longer the exposure to gluten, the greater the risk of autoimmunity developing in other organ systems [4]. Also, it is apparent that those who had been challenged with gluten for diagnostic purposes had an increased risk for developing autoimmune disorders. These data add weight to the argument for the development of screening programs to ensure diagnosis as early as possible. It also casts doubt on the practice of gluten challenge to confirm the diagnosis of celiac disease.
Material and Methods
This study was conducted prospectively for a period from January 2011 to September 2012 in Sardar Patel Medical college and associated PBM Hospital, Bikaner, Rajasthan, India. Total eightyseven newly diagnosed adult patients of celiac disease from medical OPD and ward were included in the study.
1. Newly diagnosed patients of celiac disease;
2. Patient age <55 years;
3. Patient age ≥20 years.
1. Patients with age > 55 years and age < 20yrs
2. Known case of celiac disease.
3. Patients with known autoimmune disorders on treatment
Detail medical history, drug history, physical examination, complete blood count, erythrocyte sedimentation rate, calcium profile, liver and renal biochemistry, 25-OH-D, fasting blood sugar and thyroid function tests were performed. Sera of all patients were tested for presence of IgA tissue transglutaminase (tTG) antibody by ELISA using commercially available kits. Antibody titer >50 units was considered positive. Three to four intestinal mucosal biopsies were obtained with GI endoscopy from the second part of duodenum in patients with presence of tTG antibodies. Longitudinally oriented biopsies, with muscularis mucosa seen in section were only included. Biopsies were reported by pathologist, who blinded for tTG antibody report.Biopsies with lesion i.e. total or sub total villous atrophy in addition to crypt hyperplesia and intraepithelial and lamina propria infiltration with mucosal cell, were considered to be consistent with the diagnosis of CD.
Fasting blood glucose(FBG) was measured after overnight fasting (8 hours of fasting overnight). Serum was extracted from whole blood and glucose was measured in the serum. Serum TSH testing was performed on automated immunoassay platforms employing advanced IMA technology.
The ethical committee of our hospital approved the protocol and informed consent was obtained from all patients.
Results
In present study, out of total 87 patients, 46(52.87%) were from serum TTG group 50-200 and 41 (47.12%) from serum TTG group >200. Out of total 87 patients 54 (62.06%) were females and 33 (37.93%) were males and out of 54 females 30 were from serum TTG group 50-200 and 24 were from serum TTG group >200, while out of total 33 males 16 were from serum TTG group 50-200 and 17 were from serum TTG group >200.
In present study, most common presenting complaint of patients was weakness which was found in 80(92%) of patients. Second most common complaint was easy fatiguability in 69 (79.3%) of patients, diarrhoea was present in 28 (32.25) patients, weight loss was present in 17 (19.5%) patients, sensory loss was present in 8 (9.2%) patients and malena was present in 7 (8.0%) patients.
In present study, severe anemia (Hb<7gm%) was found in 40(46.0%) patients. MCV<70 was found in 24 (27.6%) patients MCV>100 was found in 10(11.5%) patients. In PBF, most common type of anemia was microcytic found in 33(37.95) patients while 29(33.3%) patients having normocytic, 17(19.5%) patients having macrocytic and 8(9.2%) patients having dimorphic anemia.
In present study out of total 87 patients, 2 patients had their TSH<0.270 and both were from serum TTG group 50-200 while 71 patients had their TSH between 0.270-4.20 and out of them 32 and 39 were from serum TTG group 50-200 and >200 respectively while remaining 14 patients had their TSH >4.2 and out of them 12 and 2 patients were from serum TTG group 50- 200 and >200 respectively and the difference was statistically significant (p<0.01) (Table 1).
Out of total 87 patients, 62 patients had their fasting blood sugar within normal range, while 15 patients were found with impaired glucose tolerance and out of them 11 and 4 were from serum TTG group 50-200 and >200 respectively. Only 10 patients had their fasting blood sugar >125 and out of them 9 and 1 were from serum TTG group 50-200 and >200 respectively and the difference was found significant (p<0.01) (Table 2).
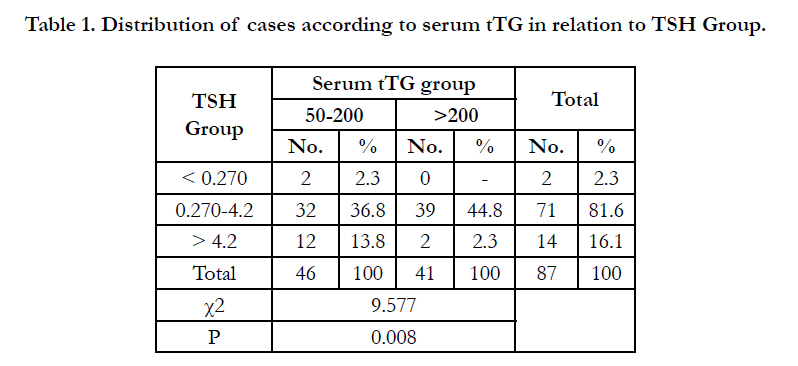

Table 1. Distribution of cases according to serum tTG in relation to TSH Group.
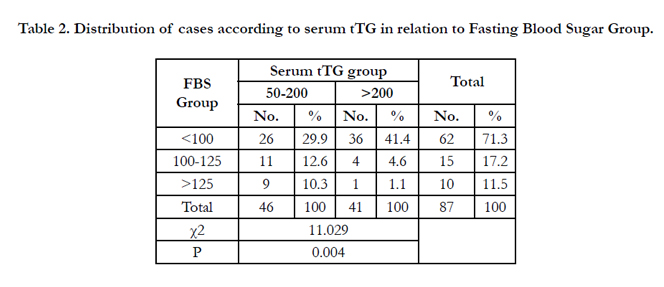
Table 2. Distribution of cases according to serum tTG in relation to Fasting Blood Sugar Group.
Discussion
CD is an immune-mediated small intestinal enteropathy that is triggered by exposure to dietary gluten in genetically predisposed individuals. Traditionally patients with CD presented with malabsorption dominated by diarrhoea, steatorrhoea, weight loss or failure to thrive (‘classical CD’) [5] but over time the proportion of newly diagnosed patients with malabsorptive symptoms has decreased, and ‘non-classical CD’ and even asymptomatic CD have gained prominence. Newly diagnosed patients with CD can present with a wide range of symptoms and signs, including anaemia, vague abdominal symptoms (often similar to irritable bowel syndrome (IBS)), neuropathy, ataxia, depression, short stature, osteomalacia and osteoporosis, liver disease, adverse pregnancy outcomes and lymphoma or with few or no apparent symptoms at all.
In present study, most common presenting complaint of patients was weakness which was found in 80(92%) of patients. Second most common complaint was easy fatiguability in 69 (79.3%) of patients, diarrhoea was present in 28 (32.25) patients, weight loss was present in 17 (19.5%) patients, sensory loss was present in 8 (9.2%) patients and malena was present in 7(8.0%) patients.
Scharla [6] in the year 2003 studied a case of 60 year old woman, she reported loss of weight, non specific GI symptoms and weakness.
Jones et al., [7] in year 2006 studied that in recent years, there had been increasing recognition that the pattern of presentation of celiac disease may be changing. The classic sprue syndrome with diarrhoea and weight loss may be less common than the more subtle presentation of celiac disease such as anaemia. In our study, severe anemia (Hb<7gm%) was found in 40 (46.0%) patients.
MCV<70 was found in 24(27.6%) patients MCV>100 was found in 10 (11.5%) patients. In PBF, most common type of anemia was microcytic found in 33(37.95) patients while 29(33.3%) patients having normocytic, 17(19.5%) patients having macrocytic and 8 (9.2%) patients having dimorphic anemia.
In our study out of total 87 patients, 2 patients had their TSH <0.270 and both were from serum TTG group 50-200 while 71 patients had their TSH between 0.270-4.20 and out of them 32 and 39 were from serum TTG group 50-200 and > 200 respectively while remaining 14 patients had their TSH > 4.2 and out of them 12 and 2 patients were from serum TTG group 50- 200 and >200 respectively and the difference was also statistically significant (p<0.01).
Out of total 87 patients, 62 patients had their fasting blood sugar within normal range, while 15 patients were found in impaired glucose tolerance and out of them 11 and 4 were from serum TTG group 50-200 and >200 respectively. Only 10 patients had their fasting blood sugar >125 and out of them 9 and 1 were from serum TTG group 50-200 and >200 respectively and the difference was found significant (p<0.01). Mehardad et al., [9] in the year 2012 described that celiac disease (CD) is closely associated with other autoimmune endocrine disorders, particularly autoimmune thyroid disease. The aim of this study was to find the frequency of celiac disease in patients with hypothyroidism in Guilan province, north of Iran. A total of 454 consecutive patients with hypothyroidism underwent celiac serological tests antiGliadin antibodies (AGA), antitissue transglutaminase antibodies (IgAtTG) and antiendomysial antibodies (EMA-IgA). Small intestinal biopsy was performed when any of celiac serological tests was positive. Eleven (2.4%) patients were positive for celiac serology, and two patients with documented villous atrophy were diagnosed with classic CD (0.4%; 95%). Two patients with classic CD had Hashimoto’s thyroiditis (HT) (0.6%; 95%). Six (54.5%) of 11 were suffering from overt hypothyroidism and 45.5% from subclinical hypothyroidism. Six (54.5%) had HT, and 45.5% had non autoimmune hypothyroidism.
In the year 2002, Collin et al., [9] described that celiac disease is a permanent intolerance to dietary gluten. The risk of clinically silent celiac disease is increased in various autoimmune conditions. The endocrinologist, especially, should maintain high suspicion and alertness to celiac disease, which is to be found in 2-5% of patients with insulin-dependent diabetes mellitus or autoimmune thyroid disease. Patients with multiple endocrine disorders, Addison’s disease, alopecia, or hypophysitis may also have concomitant celiac disease.
Pozgaj and Metelko [10] in the year 2003 described that celiac disease is a permanent intolerance to dietary gluten. Its well known features are abdominal symptoms, malabsorption of nutrients, and small-bowel mucosal inflammation with villous atrophy, which recover on a gluten-free diet. The risk of clinically silent celiac disease is increased in various autoimmune conditions.
Ch'ng CL et al., [11] in 2007 found thatthe pattern of presentation of CD has altered over the past three decades. Many cases are now detected in adulthood during investigation of problems as diverse as anemia, osteoporosis, autoimmune disorders, unexplained neurological syndromes, infertility and chronic hypertransaminasemia of uncertain cause. Among autoimmune disorders, increased prevalence of CD has been found in patients with autoimmune thyroid disease, type 1 diabetes mellitus, autoimmune liver diseases and inflammatory bowel disease. Prevalence of CD was noted to be 1% to 19% in patients with type 1 diabetes mellitus, 2% to 5% in autoimmune thyroid disorders and 3% to 7% in primary biliary cirrhosis in prospective studies. Conversely, there is also an increased prevalence of immune based disorders among patients with CD. The pathogenesis of co-existent autoimmune thyroid disease and CD is not known, but these conditions share similar HLA haplotypes and are associated with the gene encoding cytotoxic T-lymphocyteassociated antigen-4. Screening high risk patients for CD, such as those with autoimmune diseases, is a reasonable strategy given the increased prevalence. Treatment of CD with a gluten-free diet should reduce the recognized complications of this disease and provide benefits in both general health and perhaps life expectancy. It also improves glycemic control in patients with type 1 diabetes mellitus and enhances the absorption of medications for associated hypothyroidism and osteoporosis. It probably does not change the natural history of associated autoimmune disorders.
Conclusion
Our study concludes that there is significant association of celiac disease with thyroid dysfunction particularly hypothyroidism that may be clinically silent in initial stage of disease. Patients with celiac disease also have significantly impaired glucose tolerance that may worsen as disease remain uncontrolled. So all celiac disease patients should be screened for thyroid dysfunction and impaired glucose tolerance. Screening for celiac disease with serological testing is non invasive and should be considered in Indian patients with suggestive symptoms or associated autoimmune conditions. Early recognition of CD and hence early appropriate management may help in reducing severity of various autoimmune disorders, improving quality of life in these patients.
References
- Joseph A Murray (1999) The widening spectrum of celiac disease. Am J Clin Nutr March. 69(3): 354-365.
- Catassi C, Fabiani E, Rätsch IM, Coppa GV, Giorgi PL, et al., (1996) The celiac iceburg in Italy. A multicenter antigliadin antibodies screening for celiac disease in school-age subjects. Acta Paediatricia. 412: 29-35.
- Gryphon Myers (2012) Celiac Disease More Prevalent in North Indian, Asian Populations. Celiac Disease Research.
- Ventura A, Magazzù G, Greco L (1999) Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. SIGEP Study Group for Autoimmune Disorders in Celiac Disease. Gastroenterology.117(2): 297-303.
- Ludvigsson JF, Bai JC, Biagi F, Card TR, Ciacci C, et al., (2014) Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut. 63(8): 1210-28. doi:10.1136/gutjnl-2013-306578
- Scharla S (2003) Causes of osteoporosis: don't forget celiac disease. Dtsch Med Wochenschr. 128(17): 916-9.
- Jones S, D'Souza C, Haboubi NY (2006) Patterns of clinical presentation of adult celiac disease in a rural setting. Nutr J. 5: 24.
- Mehrdad M, Mansour-Ghanaei F, Mohammadi F, Joukar F, Dodangeh S, Mansour-Ghanaei R (2012) Frequency of Celiac Disease in Patients with Hypothyroidism. J Thyroid Research 1-12.
- Collin P, Kaukinen K, Välimäki M, Salmi J (2002) Endocrinological disorders and celiac disease. Endocr Rev. 23(4): 464–83.
- Pozgaj F, Metelko Z (2003) Celiac disease and diabetes mellitus. Diabetologia Croatica. 32-34.
- Ch’ng CL, Jones MK, Kingham JGC (2007) Celiac Disease and Autoimmune Thyroid Disease. Clinical Medicine & Research. 5(3): 184-192.





