Pentosidine: Can Be Related To The Etiology of Chronic Kidney Disease?
Mohsen Kerkeni1*, Hassan. Bouzidi2, Ahmed. Letaief3, Mohamed. Hammami1
1 Laboratory of Biochemistry, LR12ES05, Faculty of Medicine, University of Monastir, Tunisia.
2 Biochemistry Department, CHU Tahar Sfar, Mahdia, Tunisia.
3 Nephrology Department, CHU Fattouma Bourguiba, Monastir, Tunisia.
*Corresponding Author
Mohsen Kerkeni, Ph.D
Biochemistry Laboratory,
Faculty of Medicine,
Monastir University, Monastir, Tunisia.
E-mail: mohsen.kerkeni@yahoo.fr
Article Type: Research Article
Received: January 22, 2014; Accepted: March 1, 2014; Published: March 3, 2014
Citation: Kerkeni M, Bouzidi H, Ahmed L, Hammami M (2014) Pentosidine: Can Be Related To The Etiology Of Chronic Kidney Disease?. Int J Diabetol Vasc Dis Res. 2(2), 49-53. doi: dx.doi.org/10.19070/2328-353X-140009
Copyright: Kerkeni M© 2014 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: Advanced glycation end products (AGEs) and their receptors are prominent contributors to diabetic kidney disease. Clinical importance of AGEs toxicity in kidney disease etiologies had been rarely reported. We measured serum AGEs, sRAGE and Pentosidine levels in diabetic patients with and without nephropathy and examined whether these biomarkers are related to the etiologies of chronic kidney disease (CKD).
Design and methods: We included 30 healthy control subjects and 116 diabetic patients who were further divided into 2 subgroups: one with 30 patients without CKD, the other with 86 CKD patients. AGEs, sRAGE and pentosidine were measured in serum by ELISA.
Results: Serum levels of AGEs, sRAGE and pentosidine were significantly increased in diabetic patients without CKD compared to controls (579.78 ± 113.28 vs. 508.83 ± 119.68 pg/mL; 169.17 ± 30.41 vs. 148.72 ± 32.73 pg/ mL; 247.84 ± 21.42 vs. 214.03 ± 55.05 pg/mL, P<0.001, P<0.01, P<0.05 respectively). In diabetic patients with CKD, serum AGEs, sRAGE and pentosidine levels were significantly higher than diabetic patients without CKD (P<0.001, P<0.01, P<0.001 respectively). Serum Pentosidine levels were increased in CKD patients with tubulointerstitial nephrophathy than other etiologies (P<0.001).
Conclusions: Serum AGEs, sRAGE, and pentosidine levels are related with diabetic patients with and without CKD and pentosidine levels were increased in tubulointerstitial nephrophathy.
2.Introduction
3.Materials and Methods
3.1 Subjects
3.2 Methods
4 Statistical Analysis
5 Results
5.1 General clinical and biochemical parameters of the studied groups
5.2 Serum AGEs, sRAGE, and pentosidine levels in diabetic patients with and without CKD
5.3 Serum AGEs, sRAGE, and pentosidine levels in diabetic patients with etiologies of CKD
6.Discussion
7.Competing interest
8.Contributorship
9.Acknowledgments
10.References
Key Words
Pentosidine; RAGE; Diabetes; CKD; Tubulointerstitial Nephropathy.
Abbreviations
AGEs: Advanced glycation end products; CKD: Chronic kidney disease; CVD: Cardiovascular disease; DM: Diabetes Mellitus; eGFR: estimated glomerular filtration rate; sRAGE: soluble form of receptor for advanced glycation end products.
Introduction
There is growing evidence that tubular injury is a major feature in the development of renal dysfunction in diabetes Mellitus (DM). Tubular cells are not only affected secondary to glomerular injury but are also primary targets for pathological influence in diabetes. DM is increasing at an alarming rate in Tunisian population; patients are prone to the development of macro- and microvascular diabetic complications that represent a major cause of morbidity and mortality. The microvascular complications, which affect the small vessels, involve neuropathy, retinopathy and nephropathy. Chronic kidney disease (CKD) affects a significant portion of the world population with a prevalence of 7.2% in adults over age 30 and dramatically increasing to 23.4-35.8% over age 65 [1]. Diabetic patients with CKD represent an important segment of Tunisian population, and mostly because of the high risk of cardiovascular disease (CVD) associated with renal insufficiency, detection and treatment of chronic renal disease is now a public health priority [2,3]. The causes of CKD are various and include glomerular kidney disease, tubular and interstitial kidney disease, pre renal and vascular disorders, diabetes mellitus, and hypertension. In addition, histological studies of CKD confirmed that renal function correlates better with tubular and interstitial changes than with glomerular changes. DM is the most common cause of CKD in Tunisian patients. There are multiple pathways involved in the pathogenesis of diabetic CKD, one recent hypothesis, has an important goal is the endogen production of advanced glycation end products (AGEs) and its exogenous accumulation by dietary sources in Tunisian population. AGEs are formed by the Maillard process, a non-enzymatic reaction between ketones or aldehydes, the amino groups of proteins, lipids and nucleic acids that contributes to the aging of macromolecules [4,5]. Previous studies have confirmed that AGEs and receptor for AGEs (RAGE) interaction elicits oxidative stress generation in various types of cells and subsequently evokes vascular inflammation, macrophage and platelet activation, and thrombosis, thereby playing an important role in the development and progression of vascular complications in diabetes [6]. Several different receptors for AGEs have been identified, one of which is termed RAGE. Different cell types including human endothelial cells express RAGE [7]. The functional role of these soluble forms of RAGE in the circulation remains unclear, but they may reflect the activity of the AGE-RAGE axis. In uraemia, in the absence of diabetes, a 2-to 3-fold increase in AGEs has been reported, which indicates that the kidney plays an important role in the accumulation of these compounds. Clinical importance of AGEs toxicity in kidney disease etiologies had been rarely reported. Therefore, the first aim of this study was to examine whether serum AGEs, sRAGE and pentosidine are associated with the presence of diabetes, and with CKD in Tunisian patients. The second aim of the study was therefore to investigate the relationship of AGEs, sRAGE and pentosidine with etiologies of CKD.
The local ethics committee approved this study. Written informed consent was obtained from all patients before the enrollment. In this prospective cohort study, we measured serum concentration of AGEs, sRAGE and pentosidine in 146 participants (age range, 50-75 years). The subjects were divided into 2 groups: Group I is composed of healthy volunteers (n=30) with no DM or renal function impairment. Group II is composed of type 2 diabetic patients (n=30) without renal function impairment. Group III is composed of type 2 diabetic patients (n=86) with CKD. Etiologies of CKD in patients were chronic glomerular nephritis (n=28), chronic tubulointertitial nephropathy (n=36), and vascular nephropathy (n=22). CKD defined as decreased estimated glomerular filtration rate (eGFR). The eGFR was calculated using the 4-variable Modification of Diet in Renal Disease (MDRD) Study equation of Levery and colleagues [8]. For each patient, a data sheet was completed with the patient’s identification code, age, sex, and duration of diabetes. All diabetic patients received antidiabetic and traditional cardiovascular drugs.
Methods
In all subjects, venous blood was collected in the morning after an overnight fast. The samples were stored at -80°C until analysis. Random plasma glucose, hemoglobin A1C (HbA1C) was measured using G7 HPLC Analyser (Tosoh Europe N.V), serum creatinine, and lipid levels (HDL, LDL, cholesterol, and triglyceride), were measured using enzymatic methods by CX9 Auto-chemical analysis instrument (Beckman CX9, USA). AGEs, sRAGE, and pentosidine were quantitatively determined in serum by enzyme-linked immunosorbent assay (ELISA) kits provided by ABO Switzerland Co., Ltd, according to the manufacturer’s instructions. Briefly, the microtiter plate has been pre-coated with an antibody specific to Human AGEs (or sRAGE or Pentosidine). Samples were added, after incubation and washing, plates were incubated with HRP, developed with TMB substrate, and OD450 was determined using an ELISA plate reader.
Statistical analysis
All values are expressed as mean ± SD, median and inter-quartile range. A P value less than 0.05 was considered statistically significant. Significance between 2 groups was determined by independent sample Student t-test for continuous variables. Continuous data from >2 groups were compared with 1-way analysis of variance (ANOVA). All analyses were performed using the SPSS program (version 17).
General clinical and biochemical parameters of the studied groups
The clinical characteristics and laboratory data of controls and diabetic patients with and without CKD are shown in Table 1. In diabetic patients, we observed higher body mass index, HbA1C, serum glucose, and lipids profiles in comparison to controls. Serum level of AGEs, sRAGE and pentosidine were significantly increased in diabetic patients than in controls (P < 0.001; P < 0.01; and P < 0.05 respectively).
Values are mean ± SD or median (inter-quartile range). BMI: body mass index
a P< 0.01 compared with diabetic patients without CKD and P< 0.001 with control subjects
b P< 0.05 compared with diabetic patients without CKD and P< 0.001 with control subjects
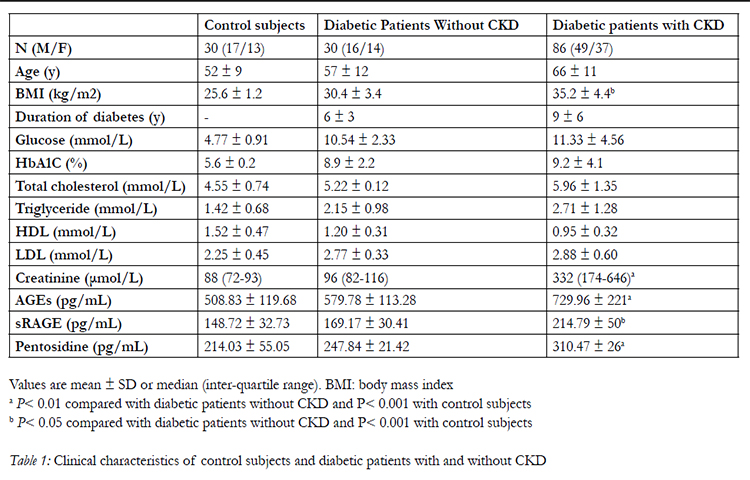

Table 1: Clinical characteristics of control subjects and diabetic patients with and without CKD.
Serum AGEs, sRAGE, and pentosidine levels in diabetic patients with and without CKD
Table 2 also shows results of serum AGEs, sRAGE, and pentosidine levels in diabetic patients with and without CKD. Patients with CKD showed an increased level of serum AGEs, sRAGE, and pentosidine (P < 0.001, P < 0.01 and P < 0.001 respectively).
Values are mean ± SD
a P< 0.01 compared with diabetic patients without CKD and P< 0.001 with control subjects
b P< 0.05 compared with diabetic patients without CKD and P< 0.001 with control subjects
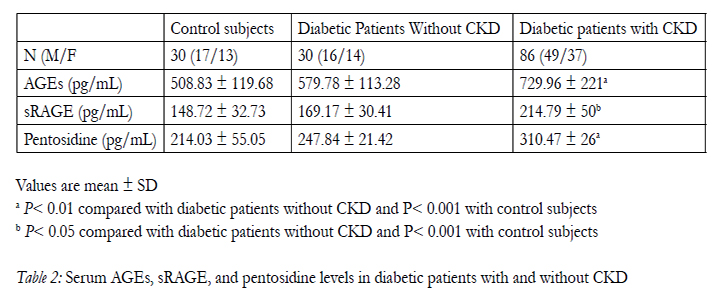
Table 2: Serum AGEs, sRAGE, and pentosidine levels in diabetic patients with and without CKD.
Serum AGEs, sRAGE, and pentosidine levels in diabetic patients with etiologies of CKD
CKD patients were also classified into 3 subgroups with etiologies of CKD as follow: Group G1 with chronic tubulointerstitial nephropathy, G2 with glomerular nephritis, and group G3 with vascular nephropathy (Table 3). We showed an increased pentosidine levels in patients with chronic tubulointerstitial nephropathy than other etiologies (P < 0.01). No difference was noted in serum AGEs and sRAGE levels in each etiology. CKD Patients with tubulointerstitial nephropathy showed a decreased eGFR than other etiology (P < 0.01).
Values are mean ± SD.
* P < 0.01 compared with G2 and with G3 group.
Group G1 with chronic tubulointerstitial nephropathy,
G2 with glomerular nephritis, and group G3 with vascular nephropathy.
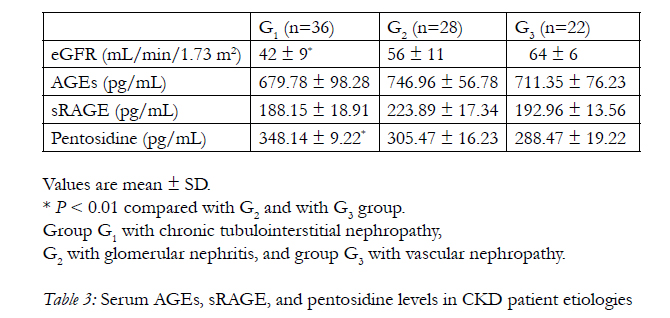
Table 3: Serum AGEs, sRAGE, and pentosidine levels in CKD patient etiologies.
Discussion
This study was designed to investigate the levels of AGEs, pentosidine and their receptor RAGE in human diabetic with and without nephropathy and in the etiology of CKD. We have demonstrated that serum AGEs, sRAGE and pentosidine are elevated in diabetic patients without CKD than the control subjects. Moreover, these biomarkers were significantly increased in CKD diabetic patients. These findings are in concordance with previous studies [9,10-12].
AGEs are metabolized and removed by the kidney but the kidney is also a site for accumulation of AGEs and AGE-related damage [13]. AGEs upregulate inflammation and the synthesis of fibronectin, laminin, and collagen IV in the kidney and promote glomerular sclerosis, fibrosis, and hypertrophy [14]. The kidney is affected by AGEs, and declining renal function entails an increase in serum AGEs, thereby amplifying damage from AGEs. AGEs are not merely a marker of renal insufficiency, as treatment with AGE inhibitors improves renal function, suggesting a direct role of AGEs in the pathogenesis of reduced renal function [15]. This is in contrast to what has been shown with hyperhomocysteinemia in kidney disease, where levels rise with declining renal function, but treatment has not been shown to be substantially beneficial [16]. Our findings also showed that elevated serum sRAGE are associated with CKD diabetic patients and with each etiology of CKD. One of mechanism by which AGEs can induce end-organ injury is via a ligand-receptor RAGE, which is widely expressed in the kidney including in podocytes, and tubular epithelial cells [17,18]. Nuclear factor NF-κB sites are located on the RAGE promoter and control cellular expression of RAGE, linking RAGE to the inflammatory response. RAGE knock-out mice are protected against macrophage influx, glomerulosclerosis and proteinuria in the adriamycin model (abstract JASN nov 2006, vol 17; 66A). RAGE also has roles in the pathogenesis of renal disorders that are not associated with diabetes, such as obesityrelated glomerulopathy, hypertensive nephropathy and ischemic renal injuries [19].
Few studies, by immunohistochemical analysis of renal biopsies from patients with diabetic nephropathy, demonstrated that the extent of AGEs formation in the glomerular and tubulointerstitial compartments correlates with the severity of diabetic nephropathy. In the glomeruli, this correlation was much stronger for carboxymethyl-lysine than for pentosidine, suggesting that carboxymethyl-lysine is an important AGEs in the pathogenesis of diabetic glomerulosclerosis. In contrast, pentosidine was major AGEs identified in the interstitium, with less consistent mesangial and extremely rare glomerular basement membranes involvement [17,20]. However, Mao et al. showed that pentosidine was localized in glomerular basement membrane [21].
Tubular cells are direct targets for enhanced glucose levels present in diabetes. Glucose uptake to tubular cells is independent of insulin, resulting in a direct relation of the plasma glucose concentration to the intracellular glucose level of tubular cells. In addition, excess glucose in the glomerular filtrate leads to enhanced proximal tubular glucose reabsorption, further augmenting the effects of hyperglycemia on intracellular glucose efflux within the proximal tubule. On exposure to glucose, tubular cells secrete vasoactive hormones like angiotensine II (due to the activation of the local intrarenal renin-angiotensin system), transforming growth factor b and matrix proteins. Glucose-dependent metabolic pathways and vasoactive hormones may directly influence tubular and interstitial cells, leading to renal dysfunction caused by nonglomerular mechanisms [22-24]. The proximal tubule is a site of reabsorption and catabolism of circulating AGEs found in diabetes. AGEs are taken by proximal tubular epithelial cell in the lysosomal apparatus and lead to cellular hypertrophy due to decreased protein breakdown resulting from reduced lysosomal proteinase activities, with a concomitant stimulation of protein synthesis [13,25].
Experimental evidence linking pentosidine accumulation to renal tubules injury has been obtained [26,27]. What could be the pathophysiological significance of renal pentosidine accumulation? Several studies support the in vivo and in vitro nephrotoxicity of AGEs [28,29]. As reviewed previously, AGE-modified proteins initiate a range of cellular responses including enhanced growth factor expression, cellular proliferation and apoptosis, angiogenesis and tissue remodelling by binding to AGE-specific receptors that might be involved in nephrotoxicity. Receptor for AGEs contributes to mesangial activation and transforming growth factor- β production; processes which converge to cause albuminuria and glomerulosclerosis [30]. These data suggest that renal AGEs accumulation that have resulted from a primary renal disorder, once present, can itself become a perpetuating factor in ongoing renal damage. These observations are of interest in light of the recent demonstration that the role of AGEs and oxidative stress in vascular complications in diabetes and AGEs induce mesangial cell loss and dysfunction, glomeruloscerosis and tubulointerstitial fibrosis [31]. For more interesting, in our study, serum pentosidine levels were increased in CKD patients with tubulointerstitial nephrophathy than CKD patients with chronic glomerular nephritis or CKD patients with vascular nephropathy. Alternatively, CKD patients with tubulointerstitial nephrophathy showed a decreased eGFR than other etiology. Pentosidine may be strongly implicated in severity of diabetic nephropathy, especially with tubulointerstitial nephrophathy. Accumulation of pentosidine within tubular cells probably reflects the tubular reabsorption of free-form pentosidine. This compound has been identified in the plasma and the urine [32]. Furthermore, pentosidine concentration is markedly elevated in uremic plasma [32]. Pentosidine probably originates from dietary sources and from the degradation of AGE-modified matrix tissues proteins. The molecular masse of free-form pentosidine (379D) allows complete filtration through the capillary glomerular basement membranes. We speculated that pentosidine, as a tubulo-nephrotoxicity AGE, might accelerate the development and severity of diabetic nephropathy and increased pentosidine might be involved in tubulointerstitial cell accumulation and causing dysfunction, as plausibly mediated by the AGERAGE axis activity. Further studies in models and in vivo are needed in order to establish definitive conclusions related to the mechanism link between pentosidine and tubulointerstitiel injury and/or mesangial injury in diabetes CKD.
In conclusion, elevated serum AGEs, sRAGE and pentosidine are associated with diabetic patients with and without CKD and both AGEs and their receptor appear to be associated with the severity of diabetic nephropathy. These findings are of interest in light of the recent observation that serum pentosidine levels were increased in CKD patients with tubulointerstitial nephrophathy. Further studies, especially larger, population- based prospective studies are required to confirm the findings suggested by the current study.
Competing interest
The authors declare that they have no conflict of interest.The local ethics committee (CHU Fattouma Bourguiba,centre 0707) approved this study.
Contributorship
MK conceived of the study, analysed statistical data and drafted the manuscript. HB participated in routinely biochemical Laboratory measurements. AL recruited patients and clinical data. MK carried out and performed the immunoassays for AGEs, sRAGE and pentosidine. MH conceived of the study, participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Acknowledgements
Author Kerkeni express his sincere appreciation to Prof. Francois Trivin (Saint-Joseph Clinical Laboratory Medicine, Paris, France) for his continued direction and encouragement throughout the study.
References
- Levey A, Eckardt K, Tsukamoto Y et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcome (KDIGO). Kidney Int 2005;67: 2089-100.
- Abderrahim E, Zouaghi K, Hedri H et al. Renal replacement therapy for diabetic end-stage renal disease. Experience of a Tunisian hospital centre. Diabetes Metab 2001; 27: 584-90.
- Ben Maïz H, Abderrahim E, Ben Moussa F, Goucha R, Karoui C. Epidemiology of glomerular diseases in Tunisian from 1975 to 2005, Influence of changes in healthcare and society. Bull Acad Natl Med 2006; 190: 403-16.
- Stern D, Yan SD, Yan SF, Schmidt AM. Receptor for advanced glycation end products: a mutiligand receptor magnifying cell stress in diverse pathologic setting. Advanced Drug Delivery Reviews 2002; 54: 1615-625.
- Takeuchi M, Yamagishi S. Involvement of toxic AGEs (TAGE) in the pathogenesis of diabetic vascular complications and Alzheimers’s disease. Journal of Alzheimers Disease 2009; 16: 845-858.
- Hou FF, Ren H, Owen WF Jr et al. Enhanced expression of receptor for advanced glycation end products in chronic kidney disease. J Am Soc Nephrol 2004;15:1889-896.
- Kalousva M, Hodkova M, Kazderova M et al. Soluble receptor for advanced glycation end products in patients with decreased renal function. Am J Kidney Dis 2006; 47: 406-411.
- Levery AS, Corsh J, Balk F et al, National Kidney Foundation practice guideline for chronic kidney disease: evaluation, classification, and stratification, Ann Intern Med 2003; 139:137-147.
- Brownlee M, Cerami, A, Vlassara H. advanced glycosylation end products in tissue and the biochemical basis of diabetic complications. N Engl J Med 1988;318:1315-321.
- Dyer DG, Dunn JA, Thorpe SR, et al. Accumulation of Maillard reaction products in skin collagen in diabetic and aging. J Clin Invest 1993;91:2463-469.
- McCance DR, Dyer DG, Dunn JA, et al. Maillard reaction products and their relation to complications in insulin-dependent diabetes mellitus. J Clin Invest 1993; 91:2470-478.
- Beisswenger PJ, Moore LL, Brinck-Johnsen T, and Curphey TJ. Increased collagen-linked pentosidine levels and advanced glycosylation end products in early diabetic nephropathy. J Clin Invest 1993; 92:212-217.
- Gugliucci A, Bendayan M. Renal fate of circulating advanced glycated end products (AGE): evidence for reabsorption and catabolism of AGE-peptides by renal proximal tubular cells. Diabetologia 1996;39: 149-160.
- Yang CW, Vlassara H, Peten EP et al. Advanced glycation end products up-regulate gene expression found in diabetic glomerular disease. Proc Natl Acad Sci USA 1994; 91: 9436-440.
- Williams ME, Bolton WK, Khalifah RG et al. Effects of pyridoxine in combined phase 2 studies of patients with type 1 and type 2 diabetes and overt nephropathy. Am J Nephrol 2007; 27: 605-614.
- Jamison RL, Hartigan P, Kaufman JS, Goldfard DS, Warren SR,Guarino PD, Gaziano JM. Effect of homocysteine lowering on mortality and vascular disease in advanced chronic kidney disease and end-stage renal disease: a randomized controlled trial. JAMA 2007; 298: 1212-214.
- Tanji N, Markowitz GS, Fu C. Expression of advanced glycation end products and their cellular receptor RAGE in diabetic nephropathy and nondiabetic renal disease. J Am Soc Nephrol 2001; 11:1656-666.
- Morcos M, Sayed AA, Bierhaus A, et al. Activation of tubular epithelial cells in diabetic nephropathy. Diabetes 2002;51:3532-544.
- D’Agati V, Schmidt AM. RAGE and the pathogenesis of chronic kidney disease. Nat Rev Nephrol 2010;6: 352-360.
- Horie K, Miyata T, Maeda K, et al. Immunohistochemical colocalisation of glycoxidation products and lipid peroxidation products in diabetes renal glomerular lesions. J Clin Invest 1997;100:2995-3004.
- Mao Y, Ootaka T, Saito T, et al. The involvement of advanced glycation endproducts (AGEs) in renal injury of diabetic glomerulosclerosis:association with phenotypic change in renal cells and infiltration of immune cells. Clin Exp Nephrol 2003;7:201-209.
- Ziyadeh FN. Significance of tubulointerstitiel changes in diabetic renal disease. Kidney Int Suppl 1996;54:50-56.
- Cooper ME, Gilbert RE, Jerums G. Diabetic vascular complications.Clin Exp Pharmacol Physiol 1997; 24:770-775.
- Cooper ME. Pathogenesis, prevention, and treatment of diabetic nephropathy. Lancet 1998, 352:213-219.
- Miyata T, Ueda Y, Horie K, et al. Renal catabolism of advanced glycation end products: the fact of pentosidine. Kidney Int 1998;53:416-422.
- Dominguez JH, Tang N, Xu W, et al. Studies of renal injury III :Lipid-induced nephropathy in type II diabetes. Kidney International 2000;57:92-104.
- Waanders F, Greven WL, Baynes JW et al. Renal accumulation of pentosidine in non-diabetic proteinuria-induced renal damage in rats. Nephrol Dial Transplant 2005; 20: 2060-70.
- Vlassara H, Strker LJ, Teichberg S et al. Adanced glycation end products induce glomerular sclerosis and albuminuria in normal rats. Pro Natl Acad Sci USA 1994; 91: 11704-708.
- Yamagishi S, Inagaki Y, Okamoto T et al. Advanced glycation end products inhibit de novo protein synthesis and induce TGF-beta overexpression in proximal tubular cells. Kidney Int 2003;63: 464-473.
- Wendt TM, Tanji N, Guo J, et al. RAGE drives the development of glomerulosclerosis and implicates podocytes activation in the pathogenesis of diabetic nephropathy. Am J Pathol 2003;162: 1123-1137.
- Yamagishi SI, Maeda S, Matsui T et al. Role of advanced glycation end products (AGEs) and oxidative stress in vascular complications in diabetes, Biochimica Biophisica Acta 2012; 1820:663-671.
- Miyata, TY, Ueda T, Shinzato Y, et al. Accumulation of albuminlinked and free-form pentosidine in the circulation of uremic patients with end-stage renal failure: renal implications in the pathophysiology of pentosidine. J Am Soc Nephrol 1996;7:1198-206





