Relationship Between Retinal-Renal Complications Among Type 2 Diabetic Subjects in India
Vijay Viswanathan1*, Satyavani Kumpatla1, Priyanka Tilak1, Archana Kuppusamy1
1 CM. V Hospital for Diabetes and Prof M. Viswanathan Diabetes Research Centre, No. 5, Main Road, Royapuram,
Chennai - 600 013. India.
*Corresponding Author
Dr.Vijay Viswanathan, M.D., Ph.D. FRCP (Lon)., FRCP (Glas)
Prof M. Viswanathan Diabetes Research Centre,
WHO Collaborating Centre for Research,
Education and Training in Diabetes,
No. 5, Main Road, Royapuram, Chennai – 600 013, India.
Tel: +91-44-25954913-15
Fax: +91-44-25954919
E-mail: drvijay@mvdiabetes.com
Article Type: Research Article
Received: Aprial 09, 2013; Accepted: Aprial 24, 2013; Published: Aprial 26, 2013
Citation: Viswanathan V, Kumpatla S, Tilak P, Kuppusamy A (2013) Relationship Between Retinal-Renal Complications Among Type 2 DiabeticSubjects in India. Int J Diabetol Vasc Dis Res. 1(2), 8-14. doi: dx.doi.org/10.19070/2328-353X-130003
Copyright: Viswanathan V© 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: The aim of this study was to determine the relationship between retinal-renal complications among type 2 diabetic subjects in India.
Subjects and Methods: A total of 502 subjects with type 2 diabetes who underwent Fundus Photography and Fundus Fluorescein Angiography (FFA) for diabetic retinopathy (DR) and 24hr urinary creatinine clearance (Crcl) test for diabetic nephropathy (DN) on the same day were included in this analysis. They were divided into groups based on the severity of retinopathy and Crcl values. Out of 502 subjects, 272 subjects had subsequent follow-up details spanning 22 months. Anthropometric, haemodynamic and biochemical details at baseline and follow-up and mortality details were recorded.
Results: The mean Crcl values decreased significantly with increasing severity of DR (p < 0.001). The percentage of subjects with non-proliferative diabetic retinopathy also decreased with decreasing Crcl. In the follow-up data, severity of DR increased compared to baseline as per stages of Crcl. There was a decline in survival when both the complications are present. Number of subjects who died was high at severe stages of these complications. Crclwas significantly associated with declining status of both the complications.
Conclusions: The degree of diabetic retinopathy and severity of diabetic nephropathy showed significant association among type2 diabetic subjects.
2.Introduction
3.Materials and Methods
4.Statistical Methods
5.Results
6.Discussion
7.Acknowledgements
8.References
Key Words
Diabetic Nephropathy; Diabetic Retinopathy; Type2 Diabetes; India.
Introduction
The prevalence of type 2 diabetes shows a significant rise world wide [1]. Diabetic Retinopathy (DR) and Nephropathy (DN) are the most common microvascular complications of diabetes [2]. They share common pathogenic mechanisms even though common pathways of capillary damage may lead to different structure and functions of the organs involved. High prevalence of proteinuria in patients with proliferative retinopathy has been reported earlier [3] and some studies reported that DR is more severe in patients with severe DN and those with advanced DN have far more lesions of DR than those without DN [2, 4]. These studies lay evidence that DR and DN coexist and there is a close relationship between the development and progression of these two complications.
There are few similarities in the coexistence of DR and DN being both as microvascular disease and microscopically both have capillary basement membrane thickening. However, capillary closure is apparent in the retina and kidney after sufficient exposure to disease with duration. The pathophysiology of DN and DR is more or less similar, which commences with increase in vascular permeability. The selective increase in permeability to albumin in early DN is caused by loss of polarity across the glomerular basement membrane [5] and the disease mechanism in the eye is probably a breakdown of tight junctions between cells. The onset of proteinuria and proliferative retinopathy are both related to previous poor glycemic control, duration of diabetes and hypertension [6-8].
It has been suggested that 25-50% of type 2 diabetic patients may have kidney alterations [9]. From the recent studies, it is evident that the presence of retinopathy itself may reveal patients at risk for nephropathy [10-12]. In a cross sectional study of patients with type 1 and type 2 diabetes to determine the predictive value of DR, univariate analysis indicated that patients with DR were 5.68, 13.39 and 3.51 times as likely to have DN compared with those without DR in the whole study population and in type 1 and type 2 diabetes respectively [10].
The association between DR and DN has been demonstrated in other populations. However, there is lack of evidence that determine the association of retinalrenal complications among subjects with type 2 diabetes in India. Hence the aim was to evaluate the impact of retinopathy as assessed by Fundus Photography and Fundus Fluorescein Angiography (FFA) on the rate of progression of nephropathy as assessed by creatinine clearance (Crcl) in 24hr urine collection. We also aimed to evaluate the associated risk factors and its outcome in the coexistence of these two complications.
Materials and Methods
Subjects with type 2 diabetes who underwent retinal and renal examination on the same day from June 2006 to June 2007 in a tertiary care hospital in India were included in this study. All the subjects underwent Fundus Photography and FFA for DR and 24 hour urinary Crcl test for DN. Those who had presence of DR (any grade) attributable to type 2 diabetes and with persistent proteinuria were included and subjects with type 1 diabetes, gestational diabetes and subjects with incomplete laboratory data were excluded from this analysis. A total of 502 (M:F 351:151) subjects with mean age of 55.8 years and mean duration of diabetes of 13.8 years were selected for this analysis. Out of 502 subjects, 272 (M:F 191:81) subjects who had subsequent follow-up details of both the complications spanning a median follow-up period of 22 months were further analysed for their outcome. All the follow-up biochemical, anthropometric and haemodynamic details were obtained from the medical records of the subjects.All the subjects were known diabetic patients and were on treatment with oral hypoglycemic agents and known hypertensives were on antihypertensive medication. The study was approved by the Institutional Ethics committee.
Retinal examination was performed in all the subjects by a trained ophthalmologist. Fundus Photography was taken to document DR followed by FFA to confirm findings, to look for macular ischaemia and to rule out subtle neovascularization. DR was classified based on International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales (13). This international clinical classification system is based on an evidence-based approach of ETDRS and WESDR studies. Retinopathy was classified as non-proliferative (microaneurysms, intra-retinal hemorrhages, hard exudates without new vessels) or proliferative (newly formed blood vessels and/or growth of fibrous tissue into the vitreous cavity or scars of photocoagulation). Subjects were divided into groups based on the severity of DR [Group1 had Non-Proliferative Diabetic Retinopathy (NPDR) (n=231), group2 had clinically significant macular edema (NPDR with maculopathy) (n=231) and group3 subjects had Proliferative Diabetic Retinopathy (PDR) (n=40)]. They were further divided into groups based on the Crcl values as per KDOQI guidelines from stage 1 to stage 4. Stage1 (group1) (Crcl ≥90ml/min) (n=219), stage2 (Crcl 60-89ml/min) (group 2) (n=181), stage3, (group 3) (Crcl 30-59ml/min) (n=64) and stage4 (group 4) (Crcl < 30ml/min) (n=38).
Demographic, anthropometric and hemodynamic details like age, gender, systolic blood pressure (SBP), diastolic blood pressure (DBP), family history and duration of diabetes were recorded. BMI was calculated. Biochemical details like fasting and postprandial plasma glucose, HbA1c, lipid profile, urea, creatinine and 24hr proteinuria values were recorded. All the biochemical estimations were done by using standard enzymaticrocedures using Hitachi auto analyzer 912. Plasma glucose was estimated by glucose oxidase peroxidase method. HbA1c was measured by HPLC (Bio-Rad) method. Renal parameters like urea were estimated by kinetic enzymatic UV assay. Serum or urine creatinine was estimated by Jaffe’s kinetic method. Urinary protein was determined by turbidimetric procedure using trichloroacetic acid reagent. Fasting serum samples were used to estimate total cholesterol by using specific enzymatic reagents which react with cholesterol oxidase-PAP. Triglyceride by GPO-PAP method, low density lipoprotein cholesterol by direct method and high density lipoprotein cholesterol enzymatically by cholesterol esterase and cholesterol oxidase coupled with polyethylene glycol to the amino groups. Very low density lipoprotein cholesterol was calculated by dividing triglyceride by 5 (TG/5).
Presence of other diabetic complications like diabetic neuropathy, peripheral vascular disease and coronary artery disease (CAD) occurred during the follow-up visits was noted. Neuropathy was diagnosed as Vibration Perception Threshold >25V by biothesiometer (14). Peripheral vascular disease was diagnosed if the ankle brachial index was < 0.8. The presence of CAD was defined by any history of CAD, hospital records of confirmed myocardial infarction and definite history of angina or coronary revascularization procedure. Out of 502 subjects, 272 subjects who had follow-updetails were again divided as per KDOQI guidelines and DR status. Outcome of the subjects was determined from their current status of DR and DN compared to their baseline status. Subjects who died were recorded and the cause of death was obtained and noted from the hospital mortality register. Cardiovascular death was defined as death caused by ischaemic heart disease, definite history of angina, stroke or sudden death.
During follow-up visits,subjects were coded as improved if they showed improvement in their renal status as per KDOQI stages and decrease in the severity of their retinopathy status. Subjects were considered as retaining same status if during their follow-up they were found to be in the same stage of renal and DR status; however they were considered as deteriorated if they showed deterioration in DR and DN status compared to baseline status. Latest status available for the subjects who died was noted.
Statistical Methods
The analysis was performed using SPSS (version 16.0, Illinois, USA) software. Mean and SD and proportions are reported as relevant. Unpaired student’s t-test was used to compare continuous variables and chisquare test was used to evaluate proportions between groups.
Cox’s proportional hazard model (Forward stepwise addition method) was used to examine the predictive factors for the occurrence of the two complications.The model included age, gender, BMI, hypertension, family history of diabetes, duration of diabetes, smoking habit, HbA1c and presence of other complications like diabetic neuropathy and cardiovascular disease, total cholesterol, triglycerides and Crcl as independent variables. All the subjects having the follow-up data and showing decline in any of the two complications were included as dependent variable. Subjects who attained mortality were excluded from the analysis.
Kaplan Meier survival analysis was performed for 253 subjects who had follow-up details available to determine their survival time.
Results
A total of 502 subjects at baseline were categorized according to their DR and Crcl status. Table 1 summarizes the baseline demographic, hemodynamic, anthropometric and biochemical details of the study groups as per grades of DR. There was no significant difference observed in age, BMI, family history and duration of diabetes, presence of hypertension and smoking habit among the groups. SBP was significantly higher in subjects with PDR. HbA1c% was similar among the groups. Subjects with PDR had significantly higher urea levels than subjects with NPDR. The mean Crcl values decreased significantly with increasing severity of DR (p< 0.001).
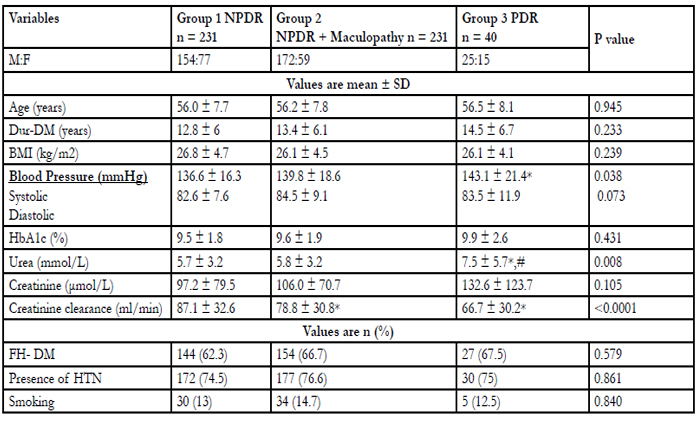

Table 1: Baseline demographic, anthropometric, hemodynamic and biochemical details of the study groups as per grades of diabetic retinopathy Dur-DM; duration of diabetes, FH-DM; family history of diabetes, HTN; Hypertension p < 0.05; * Vs NPDR; # Vs NPDR+Maculopathy.
Table 2 shows baseline demographic, anthropometric, haemodynamic, biochemical and DR status of the groups as per stages of Crcl. Age, BMI, presence of positive family history and duration of diabetes, smoking habit were similar among the groups. Presence of hypertension was significantly higher among group3 and group4 (p=0.001). Blood pressure values were significantly higher among group4 than groups 1 and 2. There was no significant difference noted among the four groups with respect to their glucose levels. Urea and creatinine levels were higher among groups 3 and 4. At baseline, among group1, NPDR was found in 102 (44.2%), 102 (44.2%) subjects had NPDR with Maculopathy and 15 (37.5%) had PDR. Similarly, in group2, 90 (39%) had NPDR, 79 (34.2%) had NPDR with maculopathy and 12 (30%) had PDR. In Group3, it was 22 (9.5%), 33 (14.3%) and 9 (22.5%) respectively whereas it was 17 (7.4%), 17 (7.4%) and 4 (10%) of subjects in group 4. The percentage of subjects with NPDR decreased drastically with decreasing Crcl.
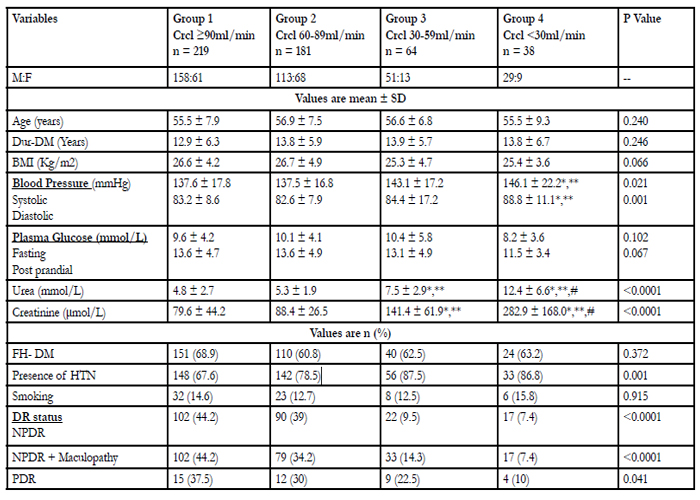
Table 2: Clinical characteristics of the study groups as per stages of Creatinine clearance (Crcl) Dur-DM; Duration of diabetes, FH-DM; family history of diabetes *Vs CrCl ≥90ml/min, ** Vs CrCl 60-89ml/min, # Vs CrCl 30-59ml/min.
Table 3 shows the comparison of baseline and follow-up details, retinopathy status and mortality as per stages of Crcl in a subgroup of 272 subjects who had followup details out of 502 subjects. There was no significant difference in age, BMI and SBP in the baseline and follow-up data. DBP was higher in group4 with Crcl < 30ml/min compared to groups 1 and 2 at baseline whereas DBP values were similar at follow-up. There was no statistically significant difference noted in lipid profile both in the baseline and follow-up data except triglycerides at follow-up.
At follow-up, in group1, 12.5% had no DR, 38.8% had NPDR, 31.3% had NPDR and Maculopathy, and 17.5% had PDR. In group2, the percentage of subjectswith no NPDR was 4.3%, 31.4% had NPDR, 50% had NPDR and Maculopathy, 14.3% of subjects had PDR. Similarly, in group3, the percentages were 3.7 vs 31.5 vs 44.5 vs 20.4% respectively. None of the subjects were without retinopathy in group4, while 18.4% had NPDR, 55.1% had NPDR with Maculopathy and 26.5% had PDR. Table 3 also shows the number of cases died during follow-up.
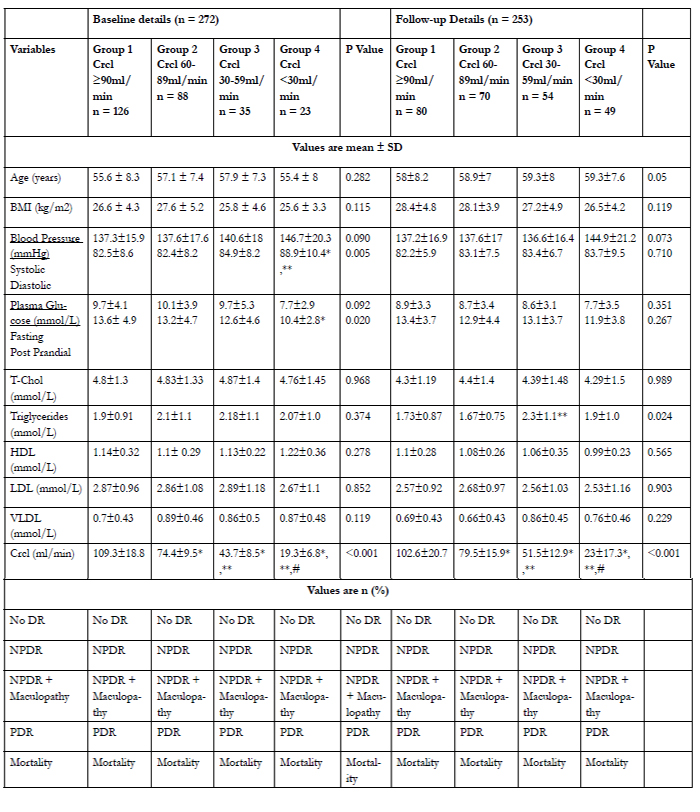
Table 3: Comparison of biochemical details and retinopathy status at baseline and during follow-up in a subgroup of subjects as perstages of Creatinine clearance.
* Vs Crcl ≥90ml/min; ** Vs Crcl 60-89ml/min; # Vs Crcl 30-59ml/min
In the baseline data, group 1 subjects with Crcl ≥90 ml/min, 15.2% of subjects were treated with ACE inhibitors (ACEI), 7.1% with Angiotensin II Receptor Blocker antagonist (ARB), 27.7% with combination of ACEI and ARB, 2.7% with beta blockers (BB) and 47.3% of subjects were treated with a combination of any two or three drugs. In Group 2 subjects with Crcl 60-89 ml/min, about 3.5% were treated with ACEI, 21.2% with ARB, 7% with a combination of ACEI and ARB, 11.8% with BB and 56.5% with combination of any two or three drugs. In Group 3 subjects (Crcl of 30-59 ml/min), none of them were treated with ACEI or BB, whereas 7.1% were treated with ARB and 92.8% were treated with a combination of drugs. In Group 4 (Crcl < 30 ml/min), none of the subjects were treated with ACEI or BB, 14.3% were treated with ARB and 85.7% with a combination of drugs. At follow-up, it was 10.1 vs 8.9 vs 20.2 vs 7.9 vs 52.8% respectively in Group 1. In Group 2, 3.0% were treated with ACEI, 7.6% with ARB, 25.8% with ACEI plus ARB, none of them were treated with BB and 63.6% with a combination of drugs. In Group 3, none of them were treated with ACEI and BB, 25% were treated with ARB, 8.3% were treated with a combination of ACEI and ARB and 66.7% with a combination of any two or three drugs. In group 4, none of them were treated with BB, 5% with ACEI, 20% with ARB, 10% with ACEI and ARB and 65% were treated with a combination of drugs.
Table 4 shows the conversion of 272 subjects from baseline till median follow-up of 22 months as per Crcl and DR stages. Considering Crcl stages, among group1, none of the subjects showed improvement in renal status, 40.5% remained similar as baseline, 54.8% showed deteriorated renal status from baseline. Among group2, 31.8% improved, 14.8% remained same and 51.1% had deteriorated renal status. In group3, improvement was seen in 17.1%, 8.6% remained same and 62.9% had worsened renal status. In group4, 13% showed improvement, 56.5% remained same and none of them showed deterioration in the renal status. The percentages of subjects who died were 4.8, 2.3, 11.4 and 30.4 % in the four groups respectively (Table 4, Panel A).
Conversion of study subjects from baseline till median follow-up of 22 months as per DR stages showed that among NPDR group, 14.5% had improved retinal status, 21.4% remained same as baseline, 58.8% had deteriorated retinal status and 5.3% of subjects died.
Among NPDR with maculopathy, 24.4% improved,42.8% remained same, 23.5% had deteriorated retinal status and the percentage of subjects who died was 9.2%. In PDR, 31.8% improved, 63.6% remained same, none of the subjects deteriorated while 4.5% died (Table 4, Panel B). The cause of death was either due to renal failure or cardiovascular events.
Values are n (%)
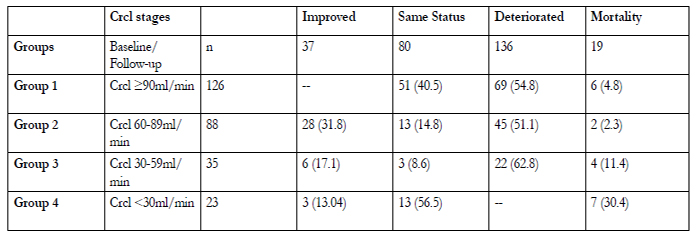
Table 4 Panel A: Conversion of the study subjects from baseline till median follow-up of 22 months as per Creatinine clearance stages.
Values are n (%)
Table 4 Panel B: Conversion of the study subjects from baseline till median follow-up of 22 months as per Diabetic Retinopathy (DR) stages
Among NPDR with maculopathy, 24.4% improved, 42.8% remained same, 23.5% had deteriorated retinal status and the percentage of subjects who died was 9.2%. In PDR, 31.8% improved, 63.6% remained same, none of the subjects deteriorated while 4.5% died (Table 4, Panel B). The cause of death was either due to renal failure or cardiovascular events.
As per the Cox’s proportional hazard model, considering all the subjects who had follow-up data and had showed deterioration in any of the two complications over a median follow-up of 22 months as dependent variable, total cholesterol with Hazard Ratio (HR) of 1.004, 95% confidence interval (CI) (1.001-1.007), (P=0.007) and Crcl with HR of 0.995, 95% CI (0.990- 1.000), (P=0.041) emerged as significant determinants of declining status in the subjects having both the complications as compared to baseline. Subjects who died were not included in this analysis
Figure 1 shows the survival rate of subjects with both complications with respect to duration of follow-up in months. It was observed that there is a continuous decline in the survival rate once both the complications are attained. Nearly, 60% deteriorated at about 22 months. It was also found that the survival will be for a maximum of 68 months with the presence of both the complications.
Discussion
It is a well known fact that subjects with diabetes are at high risk of developing complications such as nephropathy retinopathy and neuropathy than subjects without diabetes [15]. DR is characterized by microvascular abnormalities, proliferation of retinal vessels and increased retinal vascular permeability leading to the development of non proliferative and proliferative DR and macular edema [16]. DN is a life threatening complication which predisposes to excess morbidity and mortality resulting from renal failure and cardiovascular disease [17, 18]. Our hypothesis was that to see whether the severity of DR had any relationship with the presence and severity of DN in people with type2 diabetes. Studies in other populations documented a well known association between advanced DR stages and macroalbuminuria in type2 diabetic patients [19, 20]. Data from developing countries showing the relationship between these two diabetic complications are sparse but the current study supports the close relationship between presence of DR and severity of DN among type 2 diabetic patients in India.
It was reported that atleast one fifth of the diabetic individuals are affected by multiple complications and the frequency increases with increasing age and duration of diabetes [21]. Our study subjects were also older and had longer duration of diabetes which evidently proved that increased age and duration of diabetes were responsible for the development of both the complications. In the baseline data, the groups were matched with respect to age, BMI, presence of positive family history of diabetes, glucose levels, smoking habit and duration of diabetes both as per grades of DR and stages of Crcl.
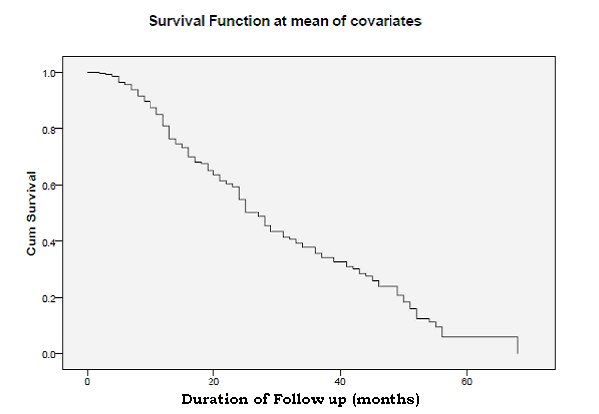
Figure 1 shows the Kaplan Meier survival analysis of the individuals who had follow up details
A study from Jordan showed that nephropathy, which is assumed to result from other microvascular complications of diabetes, was found to be significantly associated with DR [22]. In WESDR, there was a strong correlation between DN and severity of DR in all age groups [23, 24]. Our study results also complied with similar findings of worsening of DN with increasing severity of DR. In our study, the mean Crcl was found to be decreased significantly with increasing severity of DR. The percentage of subjects with NPDR also decreased with decreasing Crcl.
In contrast to the well known 3 major risk factors for the development of microvascular disease, such as glycemic status, hypertension and duration of diabetes, our study revealed total cholesterol and Crcl to be significantly associated with the declining status of both the complications by Cox’s proportional hazard model. When comparing basal and follow-up mean lipid levels, there was no significant difference noted except triglycerides at follow-up, but total cholesterol showed significant association in this analysis.
Findings from our study also highlighted that the mortality rate will be high when both DR and DN co-occur. Continuous decline of renal function was also found to be correlating with the advanced stages of DR. In the follow-up data, severity of DR increased compared to baseline as per stages of Crcl. More number of subjects died who had Crcl < 30 ml/min at follow-up. The cause of death was either renal failure or cardiovascular event. Similar to our findings Trevisan et.al also revealed that there was a drastic reduction in kidney function and higher death rate among type 2 diabetes in the presence of both the complications [25].
Since the mortality rate of the patients in our study was high, it was also observed that once both the complications occur, the improvement was seen in much lesser percentage of subjects in a median follow-up period of 22 months. Approximately 60% of subjects remained in the same status of severe Crcl or DR stages. Majority of the patients remained in the same status as that of baseline. This could be because the followup period considered is too short to observe probable changes. This is one of the limitations of our study. A decline in survival was noted when both the complications are present and about 60% of the cases deteriorated at about a median follow-up of 22 months. The maximum survival rate was less than 65 months. A similar declining pattern was observed in another study stating only 22.2% survival rate in 10 years follow-up of type 1 diabetic patients [26].
Another limitation was that it was not a prospectively planned randomized study. The analysis was done with the available hospital based data, so the effect of other potential confounders needs to be studied in future. There was a lack of systematic examination of both the complications during follow-up. The data was collected retrospectively and survival analysis was done only for the subjects whose follow-up details were available. However, utmost care has been taken while collecting the data of subjects who had follow-up of both the complications.
The present study highlights the need for screening the patients periodically to look for diabetic complications. Modification of risk factors with appropriate treatment strategies may delay the progression of these diabetic complications. In conclusion, a positive association was found between the degree of DR and DN in type2 diabetes. Patients with DR should undergo an evaluation of renal function and vice-versa.
Acknowledgements
We acknowledge the help rendered by Dr. John Benno, Ophthalmologist, for his thoughtful comments on the Fundus examination and Zenith Khasim in the data collection. We also thank V. Narayan Rao and Dhivya Muthu Kumar in the preparation of manuscript.
Conflict of Interest
There are no conflicts of interest.
References
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projection for 2030. Diab. Care 2004; 27: 1047-1053
- West K, Erdreich L, Stober J. A detailed study of risk factors for retinopathy and nephropathy in diabetes. Diabetes 1980; 29: 501-508
- Kornerup T. Retinopathia diabetica proliferans. Acta Ophthalmol 1958; 36: 87-101
- Estacio RO, McFarling E, Biggerstaff S, Jeffers BW, JohnsonD, Schrier RW. Overt albuminuria predicts diabetic retinopathy in Hispanics with NIDDM. Am J of Kidney Disease 1998; 31: 947-953
- Myers BD, Winetz JA, Chui F, Michaels AS. Mechanism of proteinuria in diabetic nephropathy: A study of glomerular barrier functions. Kidney Int 1982; 21: 633-641
- Krolewski AS, Warram JH, Christlieb AR, Busick EK, Kahn CR. The changing natural history of nephropathy in type 1 diabetes. Am J Med 1985; 78: 785-794
- Brodansky HJ, Cudworth AG, Drury PL, Kohner EM. Risk factors associated with severe proliferative retinopathy in Insulin dependent diabetes mellitus. Diab. Care 1982; 5: 97-100
- Adler AI, Stratton IM, Neil HA, Yudkin JS, Matthews DR, Cull CA, et al., Association of systolic blood pressure with macrovascular and microvascular complications of type2 diabetes (UKPDS 36):prospective observational study. BMJ 2000; 321: 412-419
- Parving HH, Gall MA, Skott P, Jorgensen HE, Lokkegaard H, Jorgensen F, et al., Prevalence and causes of albuminuria in non insulin dependent diabetic patients. Kidney Int 1992; 41:758-762
- El-Asrar AM, Al Rubeaan KA, Al-Amor SA, Moharram OA, Kangave D. Retinopathy as a predictor of other diabetic complications. International Ophthalmology 2001; 24: 1-11
- Rossing P, Hougaard P, Parving HH. Risk factors for the developmentof incipient and overt diabetic nephropathy in type 1 diabetic patients:A 10 year prospective observational study. Diab. Care 2002; 25:859-864
- Villar G, Gracia Y, Goicolea I, Barquees J. Determinants of development of microalbuminuria in normotensive patients with type 1 and type 2 diabetes. Diabetes and Metabolism 1999; 25: 246-254
- Wilkinson CP, Ferris FL, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales. Ophthalmology. 2003; 110:1677-1682.
- Young MJ, Veves A, Breddy JL, Boulton AJM. The prediction ofdiabetic foot ulceration using vibration perception thresholds: Prospectivestudy. Diabetes Care. 1994; 17:557-560.
- American Diabetes Association. Economic costs of diabetes in the US in 2002. Diab. Care 2003; 26: 917-932
- Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Giarach A. Epidemiology of diabetic retinopathy and macular edema: a systematic review. Eye 2004; 18: 963-983
- Ritz E, Orth SR. Nephropathy in patients with type2 diabetes mellitus. N Eng J Med 1999; 341: 1127-1133
- Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR. UKPDS Group. Development and progression of nephropathy in type2 diabetes. The United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int 2003; 63: 225-232
- Looker HC, Krakoff J, Knowler WC, Bennett PH, Klein R, Hanson RL. Longitudinal studies of incidence and progression of diabetic retinopathy assessed by retinal photography in Pima Indians. Diab. Care2003; 26: 320-326
- Gall MA, Hougaard P, Borch-Johnsen K, Parving HH. Risk factors for development of incipient and overt diabetic nephropathy in patients with non-insulin dependent diabetes mellitus: prospective, observationalstudy. BMJ 1997; 314: 783-789
- Morgan CL, Currie CJ, Stott NCH, Smithers M, Butler CC, Peters JR. The prevalence of multiple diabetes-related complications. Diab.Med. 2000; 17:146-151
- Muawyah DB, Maha AT, Khawla MS. Risk factors for diabetic retinopathy among Jordanian diabetics. Middle East Journal of Ophthalmology2008; 15: 77-80
- Klein R, Klein BE, Moss SE, Davis MD, DeMets DL. The WisconsinEpidemiologic Study of Diabetic Retinopathy II: prevalence and risk of diabetic retinopathy when age at diagnosis is less than 30 years. Arch Ophthalmology. 1984; 102: 520-526
- Klein R, Klein BEK, Moss SE, Davis MD, DeMets DL. The Wisconsin Epidemiologic Study of Diabetic Retinopathy II: prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmology 1984; 102: 527-532
- Trevisan R, Vedovato M, Mazzon C, Coracina A, Iori E, Tiengo A, et al., Concomitance of Diabetic Retinopathy and Proteinuria accelerates the rate of decline of Kidney function in Type 2 Diabetic patients. Diab. Care 2002; 25: 2026-2031
- Grauslund J, Green A, Sjolie AK. Proliferative retinopathy and proteinuria predict mortality rate in type 1 diabetic patients from Fyn country, Denmark. Diabetologia 2008; 51: 583-588





