Vietnamese may develop type 2 diabetes with smaller increases in body mass index and waist circumference than Taiwanese
Shigeru Yamamoto 1*, Duc Son NT Le1,2, Tzu Fang Hsu1,3, Kuo Chin Huang4,Nguyen Viet Hung1,Yueching Wong5,PoChao Huang4
1 Asian Nutrition and Food Culture Research Center, Jumonji University, Saitama, Japan
2 Pham Ngoc Thach Medical University, Ho Chi Minh City, Vietnam
3 Department of Applied Cosmetology & Graduate Institute of Cosmetic Science, Hungkuang University,Taiwan.
4 Department of Family Medicine, Taiwan Adventist Hospital, Taipei, Taiwan.
5 Department of Nutrition, ChungShan Medical University, Taiwan.
*Corresponding Author
Shigeru Yamamoto
Asian Nutrition and Food Culture Research Center, Jumonji University, Saitama, Japan.
E-mail: shigeruy@jumonji-u.ac.jp
Article Type: Research Article
Received: March 18, 2013; Accepted: March 27, 2013; Published: March 29, 2013
Citation: Yamamoto S et al., (2013) Vietnamese may develop type 2 diabetes with smaller increases in body mass index and waist circumferencethan those in Taiwanese. Int J Diabetol Vasc Dis Res. 1(1), 1-4. doi: dx.doi.org/10.19070/2328-353X-130001
Copyright: Yamamoto S© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Obesity is associated with development of diabetes. However, it seems that the level of obesity in association with diabetes may differ from country to country.
Aim: To compare BMI and waist circumference in diabetic patients between Vietnamese and Taiwanese.
Methods: Subjects were found to be diabetes mellitus by the health examination and had not treatment before. They were 163 Vietnamese and 298 Taiwanese. Body weight, height and waist circumference were measured
Results: Compared with Taiwanese, the Vietnamese diabetes had significantly lower in BMI (23.1±4.1 vs. 25.9 ± 3.4 kg/m2, p< 0.001), and waist circumference (82.2 ± 10.2 vs. 86.8± 9.4 cm, p< 0.001; respectively).
Conclusion: Vietnamese people may develop diabetes at smaller increase of BMI and waist circumference than the increase in these indices to induce diabetes in Taiwanese, thus indicating that the factors of Type 2 DM in Vietnam such as BMI, genetic, dietary and life-style which have inter-correlate complexly. It requires further in-vestigations.
2.Materials and Methods
2.1 Subjects
2.2 Anthropometric measurements
2.3 Statistical analysis
4.Results
5.Discussion
6.Conclusions
7.Acknowledgments
8.References
Introduction
The incidence and prevalence of type 2 diabetes have been increasing and becoming one of the priority health problems in not only industrialized countries but also developing and newly industrialized countries. Ac -cording to International Federation of Diabetes (IDF), in 2011 there were 366 million people with diabetes, and this is expected to rise to 552 million by 2030 [1]. In the last three decades, Vietnam and Taiwan have ex -perienced rapid improvements in socio-economy. As a result, living condition, quality of life and lifestyle have also changed thus affecting on disease’s patterns. The chronic diseases due to the lack of adaptation with these changes have increased [2,3]. The increase in prevalence of diabetes by the time has also observed in both countries [4,5]. Generally, the increase is primarily the result of lifestyle changes known as the “Nutri -tion Transition,” characterized by over-consumption of food, increased consumption of total fat (lipids), protein, and lack of physical activity [6]. The associa -tion of overweight (defined by body mass index, BMI) and type 2 diabetes has been well-documented [7,8,6]. In addition, accumulation of body fat (BF) measured by bioimpedance analyzer (BIA) or CT scan, DEXA scan) and abdominal fat (measured by waist circum -ference, wait-to-hip ratio (WHR), MRI, CT scan) are also considered as risk factors for insulin resistance, [9] , pathophysiological factors for chronic lifestyle related diseases [10]. According to previous studies, with the same BMI level, the Asians have higher BF% compared to age and gender matched Caucasians [11]. It strongly corroborates the need for specific cutoffs of BMI and abdominal fat for Asian population. The lower cut point values for BMI to define overweight and obesity and lower wait circumference value to de -fine abdominal obesity have been proposed for Asian population [12]. Studies in Indians suggested that BMI of 23 (for both genders) and waist circumference of 87cm (for men) and 82cm (for women) were optimal cut point for identifying cardiometabolic risks (includ -ing diabetes, pre-diabetes) [13]. Wildman RP et al. also suggested that BMI value of 24 and a waist circum -ference value of 80 in both genders were appropriate for use in the identification of high-risk Chinese patients [14]. In addition, the BMI cut-off of 22-24 and waist circumference cutoff near 75-80cm for women and 80-85cm for men were suggested for overweight and central adiposity in Asian population [15-17]. In Vietnam, the BMI of both undiagnosed and diag -nosed diabetes were 23kg/m2 or lower [18]. Both the genetic and dietary factors which affect on these values of diabetes, are different in the world, even among the Asians.
Taken together, whether it is appropriate to apply the same BMI and waist circumference cutoffs to all Asian populations needs to be addressed further. The purpose of this study was to compare the BMI and other anthropometric parameters of untreated diabetic patients (including both diagnosed and undiagnosed) between Taiwanese and Vietnamese.
In both countries, subjects were found to be diabetes mellitus by the health examination and had not treat-ment before. Totally, 163 Vietnamese and 298 Taiwan-ese were invited to participate in this study.
This study was approved by the Research and Ethnical Review Board of the Health Service of Ho Chi Minh City and also by the MJ Research Foundation Review Committee in Taiwan. A written informed consent was obtained from all participants. The diabetic patients will be referred to family physicians or endocrinolo-gists for receiving appropriate treatment after being enrolled into this study.
Body weight, height, waist and hip circumferences, and percent body fat were measured with the participant in the standing position wearing light clothing and no shoes. Body weight was determined using a digital scale Tanita 1609 (Tanita, Tokyo, Japan) to the nearest 0.1 kg. Height was measured with a portable Seca stadiometer 208 (Vogel & Halke, Hamburg, Germany) to the near -est 0.1 cm. Body mass index (BMI) was computed as the ratio of weight (kg) per height squared (m2). Waist circumference was measured at the minimum circum -ference between the umbilicus and iliac crest.The classification of diabetes and was carried out ac -cording to WHO criteria [19].
Data were presented as mean and standard deviation. The independent sample unpaired t-test was used to compare means and test for significant differences in anthropometric. General linear model adjusted for family age and gender was used to compare the differ -ence in anthropometric parameters in diabetic subjects between the Vietnamese and Taiwanese. A p-value < 0.05 was considered as statistical significance. Statistical analyses were performed using SPSS for windows 10.0 (SPSS, Chicago, IL).
Results
The anthropometric parameters are shown in Table 1. As compared with Taiwanese, the Vietnamese dia -betes are shorter (159.8 ±7.8 vs. 152.6 ± 6.5 cm, p< 0.001),lower in BMI (23.1±4.1 vs. 25.9 ± 3.4 kg/m2, p< 0.001), and waist circumference (82.2 ± 10.2 vs. 86.8± 9.4 cm, p< 0.001; respectively). These differences are still significant after adjustment for age and gender (Table 1).
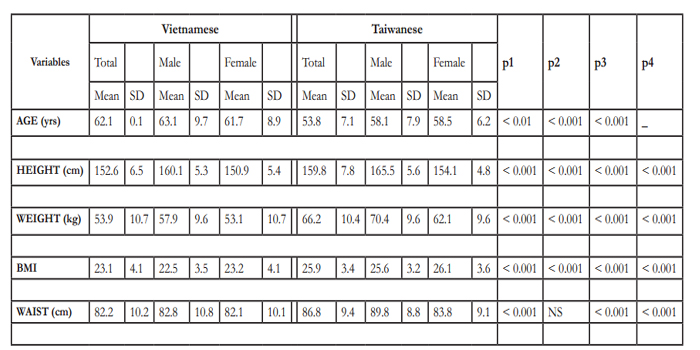

Table 1: The anthropometric parameters of study population.
P1: comparison perfomed between male subjects only
P2: comparison perfomed between female subjects only
p3: comparison performed on total population between 2 nations without any adjustment
p4: comparison performed on total population between 2 nations after adjustment for age, gender
Discussions
The prevalence of diabetes has been increasing rapidly and constitutes a significant public health problem and priority. Understanding the characteristics of diabetes is essential for developing programs to prevent and control this disease. In the current study, we found that although in the same Asian population, the BMI of Taiwanese with diabetes has significantly higher in BMI and waist circumference compared to those in Vietnamese.
In Vietnam, the BMI level of general population has slowly increased from 1980s to present; the average BMI of healthy Vietnamese was constant from 1985 to 1997 at low level [20,21] then has increased to 21.6 kg/m2 for males and to 21.4 kg/m2 for females” [22]. In addition, the waist circumference has also increased by 5cm, but is still in normal range (73.6cm for women and 76.6cm for men). In the present study, the BMI and waist circumference of Vietnamese with type 2 diabetes were 23 kg/m2 and 82cm; they are greater ap-proximately 1.5 (for BMI) and 5cm (for waist circum -ference) than those of healthy Vietnamese.
In Taiwan, according to Tu YK et, al., the BMI and waist circumference of healthy subjects have been constant for ten years (1996 – 2006) and the average BMI and waist circumference are 24kg/m2
for male and 22kg/m2 for female. While, the waist circumference in female subject has been constant (70.2 vs. 70.4cm), this index has increased by 2cm (from 80 to 82cm) in male subjects [23]. The results of this study show that the BMI and waist circumference of Taiwanese with type 2 diabetes were greater approximately 1.5kg/m2 (25.6 vs. 24.1 kg/m2) in male and 4.5 kg/m2 (26.1 vs. 21.5 kg/m2) in female subjects (for BMI); and 7cm (89.8 vs. 82.4cm) in male and 14cm in (83.8 vs. 70.4cm) female subjects (for waist circumference) than those of healthy subjects.
Taking together, it is suggested that the Vietnamese people may develop diabetes at small increase of BMI and waist circumference, while it requires more increase in these indices to induce diabetes in Taiwanese. Since the prevalence of diabetes in Vietnamese has rapidly increased in the last three decades, this finding is important point that needs to be paid more attention in the screening program for diabetes in Vietnam.
In order to early detection of diabetic patients, the screening program should include subjects with small increase in BMI and waist circumference even though their indices are in normal range. It suggests that there are other important factors other than BMI (obesity) and further investigation should conduct in the future.
The difference in genetic features between Taiwanese and Vietnamese may be contributed factors for devel -opment of diabetes with small increase of BMI and waist circumference in Vietnamese. Furthermore the lack of adaptation of dietary and lifestyle changes may be another explanation. During previous decades, the Vietnamese had spent a long period of time in lack of food, their body had to adjust with the difficult condition (especially from 1975-1985). As mentioned above,
with the increasing development and industrialization in Vietnam from 1990’s, the socio-economy had ameliorated. As consequence, a shift of traditional lifestyle (high levels of occupational and leisure time, lower fat meals) to a more Westernized one is taking place. The consumptions of energy, animal protein and lipid have significantly increased [24]. In addition, the change in consumption of brown-rice to well-polished rice has also been observed. The relationship between consumption of well-polished rice (high glycemic index) and increase postprandial blood glucose in general Vietnamese was observed [25]
As mentioned previously, cut point values of BMI to define overweight (>23 kg/m2) and obesity (>25 kg/m2) and wasit circumference (WC) to define abdominal obesity (>90 cm in men and >80 cm in women) have been proposed for Asians population [12]. However, the cutoffs for obesity indices for T2DM risk factors may differ between different Asian ethnicities. A study in Thailand suggested that the optimal cutoffs for diabetes, hypertension and dyslipidemia for men and women, respectively, are 22–23 and 24–25 kg/m2 for body mass index (BMI); 80–85 and 81–85cm for waist circumference (WC); 0.89–0.91 and 0.85–0.88 for waist–hip ratio (WHR); [26]. For Hong Kong Chinese, optimal cutoffs are 23.4 kg/m2 for BMI, and 78.2cm for WC, in men; and 23.4 kg/m2 for BMI, and 74.7cm for WC in women [27]. Li et al. recommended a BMI cutoff at 24 kg/m2 for both sexes and WC at 85cm for men and 80cm for women in a study of 13,817 adults living in Shanghai. Meta analysis of data from 13 pop -ulation-based studies in China and Taiwan showed that a BMI of 24kg/m2 had a sensitivity and specificity for identification of cardiovascular risk factors, and if this target is achieved it would prevent approximately 50% clustering of cardiovascular risk factor [28]. The pre -sent study has also enriched the literature to illustrate the potential limitations of applying uniform BMI and WC cut points to assess the health risk of individu-als globally. The cut points for BMI and WC are likely to be population specific as there are clear differences across ethnic populations in the relationship among overall adiposity, abdominal obe -sity, and visceral fat accumulation and dietary and lifestyle habits.
Conclusion
The present study indicates that in the same Asian pop -ulation, the influence of dietary intake, lifestyle may differ from one to another country in development of diabetes. For Vietnamese, the cut off values of BMI and waist circumference should be re-considered (to be lower) in establishment an appropriate screening and control program for the disease including edu -cation on their dietary patterns such as healthy food; gradually replacing well-polished white rice to brown rice; and active lifestyle.
Acknowledgements
The authors would like to thank the all volunteers for their participation and the clinical staff for their assistance.
References
- D.R. Whiting, L. Guariguata, C. Weil, and J. Shaw, IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030, Diabe tes Res Clin Pract 94 (2011) 311-321.
- C. Law, Early growth and chronic disease: a public health overview, Matern Child Nutr 1 (2005) 169-176.
- D.J. Barker, The fetal origins of type 2 diabetes mellitus, Ann Intern Med 130 (1999) 322-324.
- C.H. Chang, W.Y. Shau, Y.D. Jiang, H.Y. Li, T.J. Chang, W.H. Sheu, C.F. Kwok, L.T. Ho, and L.M. Chuang, Type 2 diabetes prevalence and incidence among adults in Taiwan during 1999-2004: a national health insurance data set study, Diabet Med 27 (2010) 636-643.
- N.T. Duc Son le, Diabetes and Metabolic syndrome in Ho Chi Minh City in 1992 - 2008, Journey of 20 years for Healthcare for community (2009)
- Khoi Huy Ha, Problems of Nutrition in Transition Period , in: Prob -lems of Nutrition in Transition Period in Vietnam, Medical Publishing House, Hanoi, 1996, pp. 153-226.
- R.M. van Dam, E.B. Rimm, W.C. Willett, M.J. Stampfer, and F.B. Hu, Dietary patterns and risk for type 2 diabetes mellitus in U.S. men, Ann Intern Med 136 (2002) 201-209.
- R.M. van Dam, W.C. Willett, E.B. Rimm, M.J. Stampfer, and F.B. Hu, Dietary fat and meatintake in relation to risk of type 2 diabetes in men, Diabetes Care 25 (2002) 417-424.
- J. Koska, N. Stefan, P.A. Permana, C. Weyer, M. Sonoda, C. Bogardus, S.R. Smith, D.R. Joanisse, T. Funahashi, J. Krakoff, and J.C. Bunt, In -creased fat accumulation in liver may link insulin resistance with subcuta -neous abdominal adipocyte enlargement, visceral adiposity, and hypoadiponectinemia in obese individuals, Am J Clin Nutr 87 (2008) 295-302.
- K.G. Alberti, P. Zimmet, and J. Shaw, The metabolic syndrome--a new worldwide definition, Lancet 366 (2005) 1059-1062.
- Appropriate body-mass index for Asian populations and its implica -tions for policy and intervention strategies, Lancet 363 (2004) 157-163.
- I.A.f.t.S.o.O.I.O.T. World Health Organisation, The Asia-Pacific Per -spective: Redefining obesity and its treatment,(2000)
- V. Mohan, M. Deepa, S. Farooq, K.M. Narayan, M. Datta, and R. Deepa, Anthropometric cut points for identification of cardiometabolic risk factors in an urban Asian Indian population, Metabolism 56 (2007) 961-968.
- R.P. Wildman, D. Gu, K. Reynolds, X. Duan, and J. He, Appropriate body mass index and waist circumference cutoffs for categorization of overweight and central adiposity among Chinese adults, Am J Clin Nutr 80 (2004) 1129-1136.
- C.H. Tseng, Body mass index and blood pressure in adult type 2 diabetic patients in Taiwan, Circ J 71 (2007) 1749-1754.
- W.H. Pan, K.M. Flegal, H.Y. Chang, W.T. Yeh, C.J. Yeh, and W.C. Lee, Body mass index and obesity-related metabolic disorders in Taiwanese and US whites and blacks: implications for definitions of overweight and obesity for Asians, Am J Clin Nutr 79 (2004) 31-39.
- O.R. Moon, N.S. Kim, S.M. Jang, T.H. Yoon, and S.O. Kim, The rela -tionship between body mass index and the prevalence of obesity-related diseases based on the 1995 National Health Interview Survey in Korea, Obes Rev 3 (2002) 191-196.
- D.S. LE, K. Kusama, and S. Yamamoto, A community-based picture of type 2 diabetes mellitus in Vietnam, J Atheroscler Thromb 13 (2006) 16-20.
- K.G. Alberti and P.Z. Zimmet, Definition, diagnosis and classifica -tion of diabetes mellitus and its complications. Part 1: diagnosis and clas -sification of diabetes mellitus provisional report of a WHO consultation, Diabet Med 15 (1998) 539-553.
- T. Giay and H.H. Khoi, Use of body mass index in the assessment of adult nutritional status in Vietnam, Eur J Clin Nutr 48 Suppl 3 (1994) S124-S130.
- Lien Thi Kim Do, HK Thanh, and Giay Tu, Nutritional status of population in Thuong Tin Village, Ha Tay Province, Vietnam, Vietnam -ese Medicine Magazine 7 (1997) 13-17.
- Q.N. Nguyen, S.T. Pham, V.L. Nguyen, L. Weinehall, R. Bonita, P. Byass, and S. Wall, Time trends in blood pressure, body mass index and smoking in the vietnamese population: a meta-analysis from multiple cross-sectional surveys, PLoS One 7 (2012) e42825
- Y.K. Tu, L.K. Summers, V. Burley, K. Chien, G.R. Law, T. Fleming, and M.S. Gilthorpe, Trends in the association between blood pressure and obesity in a Taiwanese population between 1996 and 2006, J Hum Hypertens 25 (2011) 88-97.
- National Institute of Nutrition, National survey on nutritional status of Vietnamese 2009 - 2010, Medical Publishing House, Hanoi, 2010.
- P.Y. Lin, B.T. Nhung, N.C. Khan, N. Sarukura, D. Kunii, T. Sakai, A. Kassus, and S. Yamamoto, Effect of Vietnamese common diet on postprandial blood glucose level in adult females, J Nutr Sci Vitaminol (Tokyo) 53 (2007) 247-252.
- W. Aekplakorn, V. Kosulwat, and P. Suriyawongpaisal, Obesity indi -ces and cardiovascular risk factors in Thai adults, Int J Obes (Lond) 30 (2006) 1782-1790.
- S.Y. Ho, T.H. Lam, and E.D. Janus, Waist to stature ratio is more strongly associated with cardiovascular risk factors than other simple an -thropometric indices, Ann Epidemiol 13 (2003) 683-691.
- Z. Bei-Fan, Predictive values of body mass index and waist circum -ference for risk factors of certain related diseases in Chinese adults: study on optimal cut-off points of body mass index and waist circumference in Chinese adults, Asia Pac J Clin Nutr 11 Suppl 8 (2002) S685-S693.





