The Socket Shield Technique using Bone Trephine: A Case Report
Haseeb Al Dary1*, Abeer Al Hadidi2
1 Private practice, Amman, Jordan.
2 Faculty of Dentistry, The University of Jordan, Jordan
*Corresponding Author
Dr. Hasseb Al Dary BDS,
Private practice, Amman, Jordan.
Tel: +962797789924
E-mail: dary_haseeb@yahoo.com
Received: October 08, 2015; Accepted: October 30, 2015; Published: November 05, 2015
Citation: Haseeb Al Dary, Abeer Al Hadidi (2015) The Socket shield Technique using Bone Trephine: A Case Report. Int J Dentistry Oral Sci. S5:001, 1-5. dx.doi.org/10.19070/2377-8075-SI05001
Copyright: Haseeb Al Dary© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: To avoid tissue alterations of the ridge after tooth extraction the socket shield technique was first introduced in 2010 by Hurzeler. It was suggested that instead of extracting the whole tooth, the buccal aspect of the root could be left intact to pre-serve the buccal plate of bone and prevent post extraction resorption, at the same time an immediate implant is placed; this would lead to an optimal stable esthetic result after the final delivery of the restoration. To extract the tooth while keeping the buccal aspect intact, a fissure bur is used to cut the tooth mesiodistaly then the lingual aspect of the tooth is extracted leaving a socket where the implant is to be placed.
Materials and Methods: In this case report a bone trephine was used to take out the remaining root on tooth number 24 leaving an organized rounded section of the palatal/lingual extraction site with a semi lunar internal shape of the buccal aspect of the root that will receive an implant. Results after the implant prosthesis was delivered an unchanged emergence profile was noted. The pre operative cone beam computer tomography (CBCT) showed that there were no signs of infection and that the buccal plate was intact. The post-operative CBCT showed the same unchanged findings.
Conclusion: Socket shield represents a promising technique to preserve the buccal plate of bone allowing for immediate implant placement. This helps in achieving an ultimate aesthetic outcome that may imitate the natural emergence profile of the neighboring dentition. In this case report we demonstrate that preparing the shield with a tre-phine may be of a great advantage.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.Acknowledgement
7.References
Keywords
Socket Shield; Bone Trephine; Buccal Tooth Fragment; Immediate Implant.
Introduction
The contemporary concept of success in implant dentistry has evolved from the success of osseointegration to the esthetic success; where the final prosthesis is comparable in look and emergence profile to the natural tooth/teeth.
After tooth extraction the bony socket is subjected to morphologic and dimensional changes [1-5]. Bone resorption of the alveolar ridge contour is noted especially at the buccal plate of bone where remodeling is more pronounced than at the lingual plate [2, 4] this would compromise the esthetic look of the final restoration.
Many treatment approaches have been introduced and advocated to overcome the negative consequences of tooth extraction, such as immediate implants [4, 6] graft materials [7-11] and membranes [12, 13], however no technique of bone preservation or entire regeneration of the ex-traction socket has been documented.
Clinical studies have suggested that leaving remaining roots of hopeless teeth in their sockets may prevent or decrease tissue alterations and bone resorption after tooth extraction; this was documented by numerous publications [15-19].
Salama et al [20] described the Root Submergence Technique as a way of preserving bone especially to support the relatively thin buccal plate of bone from collapsing. By maintaining the root in the socket a much greater amount of surrounding tissue may be preserved than with the other commonly used socket preservation techniques. Remodeling of the alveolar ridge leads to crestal bone resorption and thus reduction of the height of the interdental papillae. Root Submergence Technique instead maintains the natural attachment apparatus of the tooth in the pontic site, which in turn allows for complete preservation of the alveolar bone frame [20].
In 2010 Hurzeler et al published their study introducing the socket shield technique. This technique modified the root submergence technique. The Buccal fragment of the remaining root is left in the socket after root sectioning is performed from the mesial to distal side of the remaining root as to separate it into 2 fragments; Buccal and Palatal/Lingual. The buccal root fragment is left while the rest of the tooth is extracted [14], leaving a space to place the implant behind it. This technique would give the benefit of preserving the surrounding tissues similar to the root submergence technique but allows the placement of the implant at the same time.
In this case report, a modified socket shield technique was utilized where a bone trephine in-stead of fissure bur was used to cut the tooth along the long axis. This creates an organized cylindrical shaped tooth fragment on the buccal side, to be left intact supporting the buccal bone. The rest of the root is extracted harvesting some bone fragments with it to be utilized where needed. If any lingual or palatal fragment was left after trephining and root extraction, then it should be removed when drilling the osteotomy for the implant fixture.
Case Report
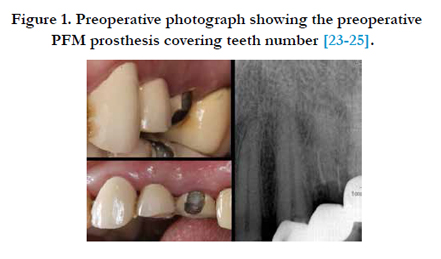
A 55 years old healthy female patient stepped into the office to replace an unstable 3 unit splinted Porcelain fused to metal (PFM) prosthesis on teeth [23-25] (Figure 1).

Clinical examination revealed that teeth number 23 and 24 were badly decayed with no ferrule effect. Tooth number 24 had no clinical crown, only a remaining root with no apparent mobility. Radiological examination revealed that the remaining root of number 24 is root canal treated with a short filling with no signsof a periapical infection (Figure 2).
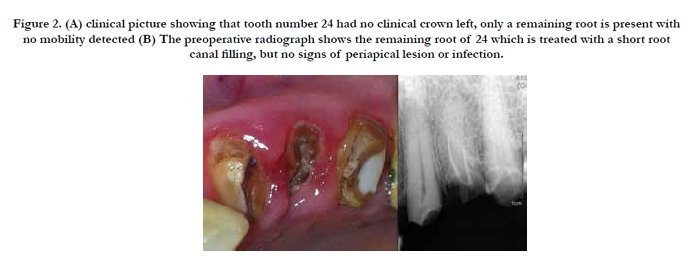
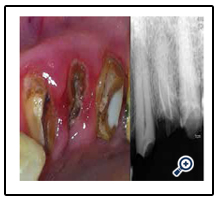
Figure 2. (A) clinical picture showing that tooth number 24 had no clinical crown left, only a remaining root is present with no mobility detected (B) The preoperative radiograph shows the remaining root of 24 which is treated with a short root canal filling, but no signs of periapical lesion or infection.
Treatment options were discussed with the patient, an implant was chosen and planned to replace the remaining root of number 24. This would allow for crowning each tooth separately giving better hygiene, esthetics and stability of the restorations.
Root canal treatment with a Fiber post and composite build up was performed on tooth number 23 and a root canal treatment with a composite filling was performed on tooth number 25; both to receive zirconium crowns.
As for tooth number 24 a modified socket shield technique was used. Separation of the root was executed using a bone trephine (stoma trephine burs from swallow dental supplies limited UK, diameter 4/5) with normal saline irrigation, 10 mm depth was reached from the edge of the exposed coronal part of the remaining root; the trephine cut was performed in a way parallel to the buccal side of the tooth following the long axis of the root (Figure 3), the cylindrical cut of the trephine was performed in a way leaving a semi lunar fragment attached to the buccal plate of the bone, and the bulk of the remaining root was extracted (Figure 4) except for the buccal shield fragment.
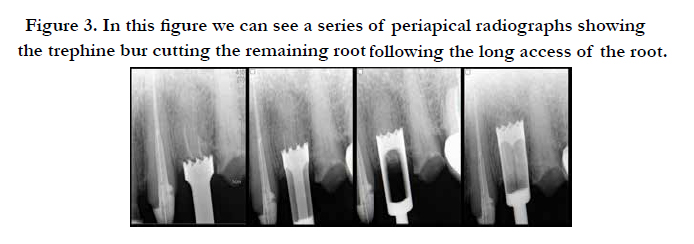
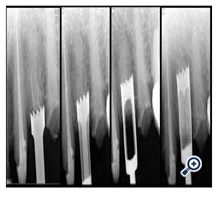
Figure 3. In this figure we can see a series of periapical radiographs showing the trephine bur cutting the remaining root following the long access of the root.
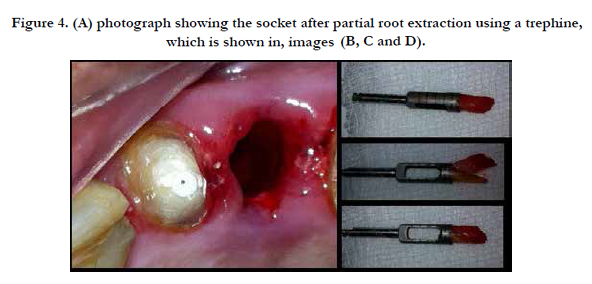
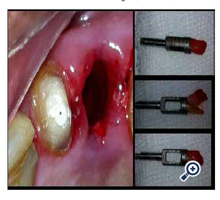
Figure 4. (A) photograph showing the socket after partial root extraction using a trephine, which is shown in, images (B, C and D).
Osteotomy was performed afterward to add another 4 mm depth from the bottom of the well that was created by the trephine cut, a subtotal of a 14mm height was obtained from the edge of thecoronal part of the root. The coronal part of the remaining intact segment "fragment" of the root was reduced to a level below the gingival margin with a coarse-grained diamond bur. After preparation of the implant bed a 4.3 x 12 mm BONITex® implant (Alphatech Systems Germany) was inserted, with a maximum torque of 25 Newton. The implant was placed at the same level of the exposed surface of the remaining healthy fragment, followed by placing a cover screw on the implant hex and leaving it unloaded (Figure 5).
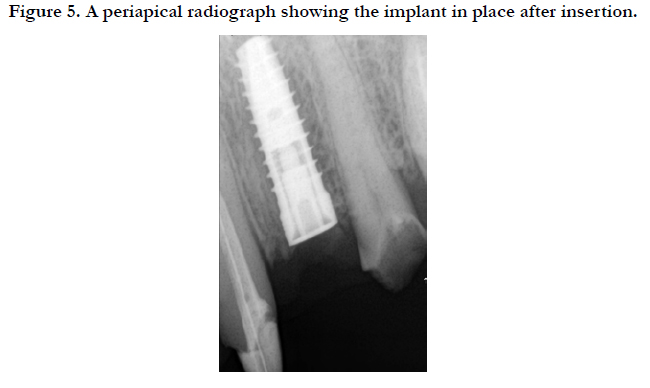
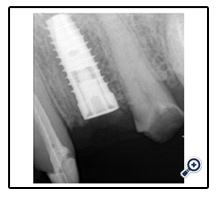
Figure 5. A periapical radiograph showing the implant in place after insertion.
An open healing was chosen and no sutures were necessary. As immediate loading was not indicated due to low primary stability, an acrylic temporary bridge was used to cover tooth number 23 and 24 and to replace number 25. A four-month period was spared before the final zirconium prosthesis was fabricated and delivered. After the implant prosthesis was delivered an unchanged emergence profile was noted (Figure 6).
The pre-operative cone beam computer tomography (CBCT) showed that there were no signs of infection and that the buccal plate was intact. The post-operative CBCT showed the same unchanged findings (Figure 8).
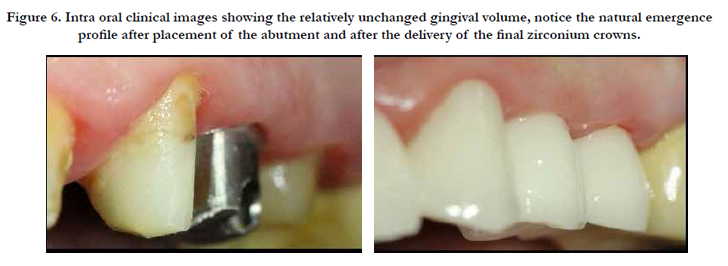

Figure 6. Intra oral clinical images showing the relatively unchanged gingival volume, notice the natural emergence profile after placement of the abutment and after the delivery of the final zirconium crowns.
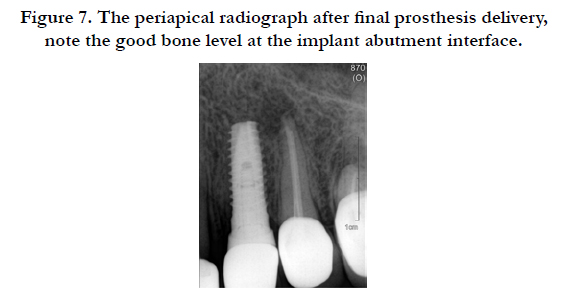
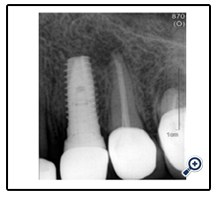
Figure 7. The periapical radiograph after final prosthesis delivery, note the good bone level at the implant abutment interface.
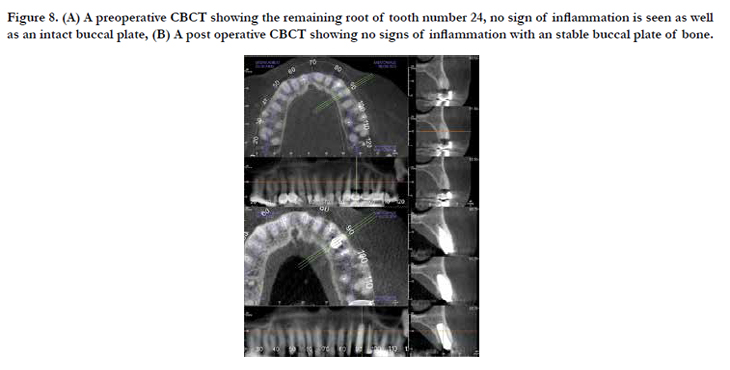
Figure 8. (A) A preoperative CBCT showing the remaining root of tooth number 24, no sign of inflammation is seen as well as an intact buccal plate, (B) A post operative CBCT showing no signs of inflammation with an stable buccal plate of bone.
Discussion
It has been documented in the literature that to retain root fragments in situ covered by mucosa represents a technique for alveolar ridge preservation [21, 22].
Socket shield technique to maintain the contour of the ridge was first described by Hurzeler in 2010 [14].
While human histological examination is needed to verify the preservation of buccal bone plate and tissue regeneration between the shield and the implant, many case reports in the literature showed the positive clinical outcome of the socket shield technique. The main advantage is to avoid noticeable alteration of ridge shapeafter tooth extraction [23-25].
Although Hurzeler et al [14] used a fissure bur to prepare the teeth into the shield; not much was illustrated in his study or in the literature about step by step procedure or instrumentation protocol which can be used to extract the root to leave an intact buccal fragment. The procedure itself, by using the fissure bur, is technique sensitive and depends on the skills of the dental practitioner. Precise and meticulous strokes are needed while sectioning the root as not to penetrate the buccal plate causing fenestration of bone or harm to the neighboring teeth. There is lack of clear visibility all the way to the apex of the root putting emphasis on tactile sensation of the practitioner [14].
Using bone trephines in implant dentistry is documented in the literature; a circular osteotomy is obtained by trephines helping to harvest discs or rings of bone to be used as grafts in the recipient sites planned [26].
In this case report the trephine was used to prepare the shield, by using the trephine instead of a fissure bur, a circular clean cut is obtained. Extreme care and time should be taken when using the free hand high speed fissure bur as not to fenestrate the bone or harm the adjacent teeth, while by using the trephine it is less technique sensitive and easier to stay on the track predetermined preoperatively. The borders of the cut may be predictable, resulting in an organized shape of the osteotomy that will receive theimplant fixture.
Also when using the trephine to extract the tooth, a bone fragment would be extracted with it; this fragment may be used as a graft material to be packed at the gap between the implant and the bone on the buccal aspect.
Conclusion
Socket shield represents a promising technique to preserve the extraction site associated with implant placement, leading to the ultimate esthetic outcome imitating the natural emergence profile and preserving the soft and hard tissue.
The shield technique protocol originally published utilized the high-speed surgical fissure bur, but this case report demonstrates that preparing the shield with a trephine may be of a great advantage. To completely judge the reaction of the tissues in humans and to compare the different armamentarium, a long-term clinical study and a human histological dissection are needed.
Acknowledgement
The authors reported no conflicts of interest related to this study.
References
- Amler MH, Johnson P, Salsman I (1960) Histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds. J Am Dent Assoc 61: 32-44.
- Pietrokovski J, Massler M (1967) Alveolar ridge resorption following tooth extraction. J Prosthet Dent 17(1): 21-27.
- Schropp L, Wenzel A, Kostopoulos L, Karring T (2003) Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent 23(4): 313-323.
- Araújo MG, Sukekava F, Wennstrom JL, Lindhe J (2005) Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol 32(6): 645-652.
- Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, et al. (2008) Dimensional changes of the alveolar ridge contour after different socket preservation techniques. J Clin Periodontol 35(10): 906-913.
- Botticelli D, Berglundh T, Lindhe J (2004) Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol 31(10): 820-828.
- Carmagnola D, Adriaens P, Berglundh T (2003) Healing of human extraction sockets filled with Bio-Oss. Clin Oral Implants Res14(2): 137-143.
- Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, et al. (2006) A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent 26(1): 19-29.
- Araújo M, Linder E, Wennström J, Lindhe J (2008) The influence of Bio- Oss collagen on healing of an extraction socket: an experimental study in the dog. Int J Periodontics Restorative Dent 28(2): 123-135.
- Fickl S, Zuhr O, Wachtel H, Bolz W, Huerzeler MB (2008) Hard tissue alterations after socket preservation: an experimental study in the beagle dog. Clin Oral Implants Res 19(11): 1111-1118.
- Araújo M, Linder E, Lindhe J (2009) Effect of a xenograft on early bone formation in extraction sockets: an experimental study in dog. Clin Oral Implants Res 20(1): 1-6.
- Lekovic V, Kenney E, Weinlaender M, Han T, Klokkevold P, et al. (1997) A bone regenerative approach to alveolar ridge maintenance following tooth extractions. Report of 10 cases. J Periodontol 68(6): 563-570.
- Lekovic V, Carmargo PM, Klokkevold PR, Weinlaender M, Kenney EB, et al. (1998) Preservation of alveolar bone in extraction sockets using bioabsorbable mebranes. J Periodontol 69(9): 1044-1049.
- Hurzeler MB, Zuhr O, Schupbach P, Rebele SF, Emmanouilidis N, et al. (2010) The socket-shield technique: a proof-of-principle report. J Clin Periodontol 37(9): 855-862.
- Filippi A, Pohl Y, Von Arx T (2001) Decoronation of an ankylosed tooth for preservation of alveolar bone prior to implant placement. Dent Traumatol 17(2): 93-95.
- Malmgren B, Cvek M, Lundberg M, Frykholm A (1984) Surgical treatment of ankylosed and infrapositioned reimplanted incisors in adolescents. Scand J Dent Res 92(5): 391-399.
- Malmgren O, Malmgren B, Goldson L (1994) Orthodontic Management of the Traumatized Dentition. Copenhagen, Munksgaard 587-633.
- Andersson L, Emami-Kristiansen Z, Hogstrom J (2003) Single-tooth implant treatment in the anterior region of the maxilla for treatment of tooth loss after trauma: a retrospective clinical and interview study. Dent Traumatol 19(3): 126-131.
- Bjorn H (1963) Free transplantation of gingiva propria. Sven Tandlak Tidskr 22: 684-689.
- Salama M, Ishikawa T, Salama H, Funato A, Garber D (2007 ) Advantages of the Root Submergence Technique for Pontic Site Development in Esthetic Implant Therapy. Int J Periodontics Restorative Dent 27(6): 521-527.
- Casey DM, Lauciello FR (1980) A review of the submerged-root concept. J Prosthet Dent 43(2): 128-132.
- Dugan DJ, Getz JB, Epker BN (1981) Root banking to preserve alveolar bone: A review and clinical recommendation. J Am Dent Assoc 103(5): 737-743.
- Chen CL, Pan YH (2013) Socket Shield Technique for Ridge Preservation: A Case Re-port. J Prosthodont Implantol 2(2): 16-21.
- Glocker M, Attin T, Schmidlin P (2014) Ridge Preservation with Modified “Socket-Shield” Technique: A Methodological Case Series. Dent J 2(1): 11-21.
- Al-Dary H (2013) The Socket Shield Technique: A Case Report. Smile Dent J 8(1): 32-36.
- Stevens M, Emam H, Alaily M, Sharawy M (2010) Implant Bone Rings. One-Stage Three-Dimensional Bone Transplant Technique: A Case Report. J Oral Implantol 36(1): 69-74





