Oral Prosthetic Rehabilitation with and without Implants after Radiation Therapy and Ablative Surgery
Gotfredsen K1*, Abdullah S2
1. Professor, Department of Oral Rehabilitation, School of Dentistry, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark.
2. Dentist, School of Dentistry, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark.
*Corresponding Author
Klaus Gotfredsen,
Professor, Department of Oral Rehabilitation,
School of Dentistry, Faculty of Health and Medical Sciences,
University of Copenhagen, Denmark.
Tel: +45 35 326746
E-mail: klg@sund.ku.dk
Received: July 31, 2015; Accepted: August 21, 2015; Published: August 25, 2015.
Citation: Gotfredsen K, Abdullah S (2015) Oral Prosthetic Rehabilitation with and without Implants after Radiation Therapy and Ablative Surgery. Int J Dentistry Oral Sci. S2:004, 21-25. dx.doi.org/10.19070/2377-8075-SI02004
Copyright: Gotfredsen K© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
To understand the impact of oral rehabilitation of patients treated for head and neck cancer, it would be beneficial to describe the patient-reported problems related to fixed and removable prostheses with and without implants and which impairments are improved by the treatment.
The aim of the present study was to evaluate the impact of oral rehabilitation with fixed versus removable prostheses with and without implants on Oral Health Related Quality of Life (OHRQoL) measured with OHIP-49 for patients treated with radiation therapy and/or ablative surgery.
The study cohort included 51 patients (35 males, 16 females) with a mean age of 66 years.
A significant improvement in OHRQoL was demonstrated after oral rehabilitation with fixed and removable dental prosthesis for patients after radiation and/or ablative jaw surgery. Thirty-nine of the 43 patients improved oral health related quality of life after prosthetic rehabilitation. Twenty-four patients improved with more than 20 points. The oral rehabilitation resulted in better appearance and chewing function.
No significant effect between fixed versus removable prostheses and no significant effect of implant on the OHIP-score. This may be explained by a limited sample size, a great variation between the included patients and the validity of the OHIP-49 questionnaire measure to demonstrate patient-reported improvements or deterioration of a prosthetic treatment in this group of very functional compromised patients.
2.Introduction
2.1.Hypotheses
3.Materials and Methods
3.1. Exclusion criteria
4.Results
5.Discussion
6.Acknowledgement
7.References
Keywords
Ablative surgery; Oral Health Impact Profile (OHIP); Oral Health Related Quality of Life; Oral Rehabilitation; Radiation.
Introduction
Head and neck (H&N) cancers are diagnosed for about 1400 patients in Denmark annually and within this group oral cancer account for 220 cases [1]. Risk factors are tobacco, alcohol consumption and human papilloma virus and the symptoms include ulceration, swallowing disability, pain, bleeding, tumor and lymphadenopathy in the neck. The primary treatment of H&N cancer is radiation therapy and jaw resection [2]. Odontogenic infections are a potential risk for patients, who receive cervicofacial radiotherapy. Thus, teeth with infection foci are extracted prior to the radiation therapy [3]. After radiation therapy and ablative surgery the patient are oral rehabilitated to obtain sufficient orofacial functions e.g. mastication, swallowing and speech, which are of great importance for the quality of life [4]. The treated patients have salivary hypofunction, taste disturbances, orofacial pain and chewing muscle pathology influencing the patient’s quality of life (QoL).
The Danish Health and Medicine Authority have described a treatment course for patients with cancers. Dental rehabilitation with fixed and removable prostheses including obturators is described as a final part of the treatment course [5]. A recent systematic review indicated that patients who have undergone radiotherapy or surgery for H&N cancer may particularly benefit from prostheses supported by dental implants, but studies analyzing the impact of dental rehabilitation with implants is missing [6]. Thus, it is of outmost importance to analyzed how various oral prosthetic reconstructions influence the oral functions and patient’s oral health related quality of life [7]. The most important goal is to improve the oral health related quality of life (OHRQoL) for the patient. The Oral Health Impact Profile (OHIP) questionnaire [8] is the most frequently used, validated questionnaire within dentistry to evaluate OHRQoL. It will be of great interest to analyze change in OHIP-49 scores for removable and fixed oral reconstructions supported with or without implants in relation to diagnoses, general health status, social and psychological aspects, extent and position of the intraoral defect and number of tooth units before and after treatment [9].
To understand the impact of oral rehabilitation of patients treated for H&N cancer, it would also be beneficial to describe the patient-reported problems related to fixed and removable prostheses and which impairments are improved by the treatment [10,11].
The aim of the present study was to evaluate the impact of oral rehabilitation with fixed versus removable prostheses with and without implants on Oral Health Related Quality of Life measured with OHIP-49 for patients treated with radiation therapy and/or ablative surgery.
Oral prosthetic rehabilitation with implants will improve OHRQoL for patients after radiation and/or ablative jaw surgery. No differences in OHIP-49 change between patients treated with fixed or removable dental prostheses.
Material and Methods
The study cohort included 51 patients (35 males, 16 females) with a mean age of 66 years (range 42 – 84 years) referred to department of oral rehabilitation for prosthetic reconstruction of the teeth and supporting tissues after radiation therapy and/or jaw resection between 2007 and 2012. The group consisted of patients with 4 main diagnosis: 30 with oral cancer (59%), 14 with pharynx cancer (27%), 4 with skin cancer (8%) and 3 with other cancers (6%). Ten of the patients underwent reconstruction with obturator prostheses following maxillectomy (Figure 1a, b). Fortytwo of the patients had radiation therapy and 32 ablative surgeries.Seven patients had oral rehabilitation only in the lower jaw, 14 in the upper jaw and 30 had prostheses in both jaws. Six-teen had fixed prostheses, 5 fixed combined with removable prostheses and 30 had only removable prostheses. In twelve of the 51 patients dental implants were inserted for obtaining increased retention of the prostheses.
To be included in the study the patients should have a need for prosthetic rehabilitation caused by removal of teeth and tissue prior to radiation therapy for H&N cancer or resection of one of the jaws, and should have less than 10 occluding tooth units before oral rehabilitation.
The patient too debilitated for oral rehabilitation at the Dental School. The patient psychological status was inappropriate for oral rehabilitation.
After an introduction and before oral prosthetic treatment the 51 patients filled in the OHIP-49 questionnaire and one to three months after finalized oral prosthetic treatment 43 of the participants filled in the OHIP-49 and 9 additional questions. Fifth-teen patients dropped out or were excluded as they were not able to participate in the follow-up examination with the second questionnaire or the questionnaire was not sufficient filled out. The questions were answered on a scale from No problems (0) to very frequent problems (4) according to definition from OHIP-49 [8].
The primary outcome variable was the change in Oral Health Impact Profile (OHIP) score [8]. Other variables: Age, gender, diagnose for H&N cancer, resection therapy (+/-), radiation therapy (+/-), jaw (upper/lower), jaw zone for replacement (aesthetic/ masticatory), fixed (FDP) or removable (RDP) prosthesis, implant (+/-). The aesthetic zone was defined as incisors, canines and 1st premolar replacements, whereas the masticatory zone was replacement of 2nd premolar, 1st and 2nd molar.
To examine the frequency of experienced oral problems by the participants, the items with the highest accumulated scores to the OHIP-49 questions was calculated before and after treatment.
Goodness-of-fit tests (Kolmogorov Smirnow) showed that the OHIP score were not normally distributed. Non-parametric ANOVA tests and Turkeys post hoc test to align for multiple comparisons were used to test differences in OHIP scores between participants treated with RDP or FDP, with or without implants, radiated and/or resected, different diagnosis, upper or lower jaw, age, gender and jaw zone. Significance level p<0.05.
Results
Thirty-nine of the 43 patients had lower OHIP score after than before oral rehabilitation e.g. improved oral health related quality of life after prosthetic rehabilitation. Twenty-four patients improved with more than 20 points.
Overall a significant improvement in OHIP-49 scores e.g. a significant reduction in mean OHIP-49 scores, from a mean of 77 (95% Confidence Interval (C.I.) 51-98) to 40 (C.I. 16-82) was registered. No significant difference (p=0.08) was seen in OHIP-49 change for participants treated with fixed compared to removable prosthesis or between combination of FDP/RDP and FDP (P=0.92) or RDP (P=0.13). Patients treated with implants did not differ significantly (p=0.16) in OHIP change from patients without implant-supported prostheses neither for the fixed nor the removable reconstruction. The number of lost implants was 4 inserted in 2 patients, who were not very satisfied with the treatment. No significant differences were found for age, gender, diagnosis, therapy, jaw or jaw zone.
The 10 most experienced problems before and after treatment are shown in Table I and II. The most frequent OHIP-49 reported problems before oral rehabilitation was: difficult chewing (Q1), appearance affected (Q4) and avoid eating some foods (Q28). A reduced frequency of problems was reported 1-3 month after treatment, but problems still existed. After treatment the most frequently reported problems was: food catching (Q7), avoid eating some foods (Q28) and difficult chewing (Q1). Phonetic problems were reported both before and after treatment and were mainly restricted to patients with maxillary obturator prostheses (Figure 1a, b). The oral rehabilitation resulted in better appearance and chewing function, as the appearance was not mentioned among the 10 most frequent problems and difficult chewing was reduced from 63% to 33% of the patients after the oral rehabilitation.
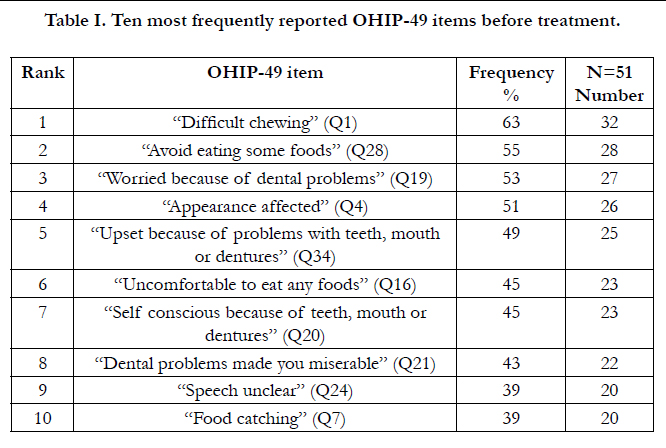

Table I. Ten most frequently reported OHIP-49 items before treatment.
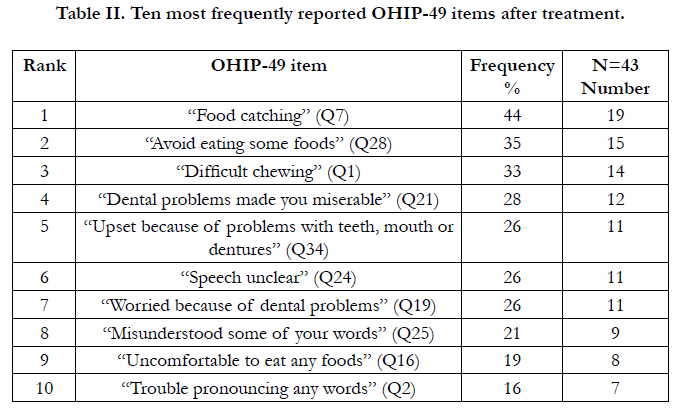
Table II. Ten most frequently reported OHIP-49 items after treatment.
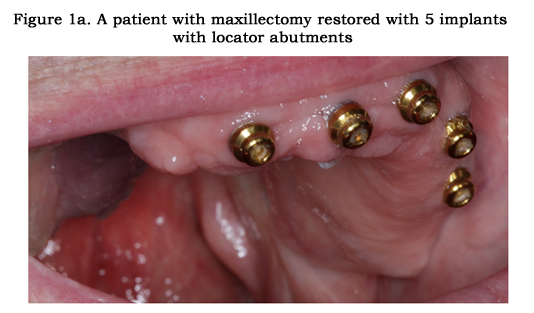

Figure 1a. A patient with maxillectomy restored with 5 implants with locator abutments.
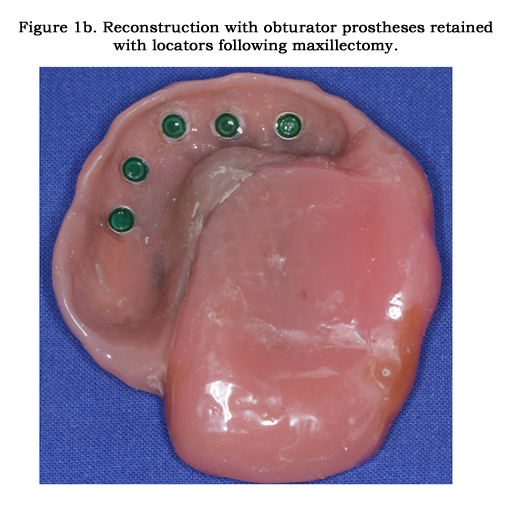
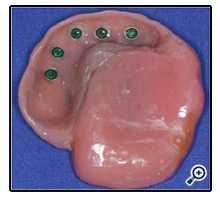
Figure 1b. Reconstruction with obturator prostheses retained with locators following maxillectomy.
Discussion
The present study demonstrates a significant improvement in OHRQoL after oral rehabilitation with fixed and removable dental prosthesis for patients after radiation and/or ablative jaw surgery. However, no significant effect between fixed versus removable prostheses and no significant effect of implant on the OHIP-score was found. This may be explained by a limited sample size, a great variation between the included patients and the validity of the OHIP-49 questionnaire measure to demonstrate patient-reported improvements or deterioration of a prosthetic treatment in this group of very functional compromised patients.
Most of the patients in the present study had only few remaining teeth after oral rehabilitation. Thus, there was a need for not only replacing teeth but also alveolar bone and mucosal tissue. In cases with great tissue loss a removable prosthesis may be more beneficial than a fixed prostheses [12]. When only few teeth were remaining fixed prostheses were frequently combined with RDP´s. An oral rehabilitation combining crowns and RDPs increase the function of the RDP as guided surfaces, rests, attachments and milled palatal ledges for clasps reciprocal arms can be incorporated in the crown abutments [13].
In contrast to a number of other studies [6], the present study could not find a significant effect of implants on the OHRQoL score. This may be caused by a high loss of implants in irradiated bone [14]. The number of lost implants in this study was, however, only 4 inserted in two patients but both patients responded negatively on the treatment and showed deterioration in OHRQoL. Although the 10 other patients with implant-supported reconstructions had improved OHRQoL after oral rehabilitation the sample size and the variation in the material was to great for demonstrating significant differences. Thus, the material indicated that by increasing the sample size significant benefits of implants would appear.
Measures of self-reported losses in health related quality of life provide a holistic approach to evaluate treatment effectiveness. The most frequently used measure within dentistry is the OHIP, but a great number of other measures have been used for patients exposed for radiation or ablative surgery [15]. Kornblith and coworkers used the obturator functioning scale (OFS) for patients with obturator prosthesis and combined it with Psychosocial Adjustment to illness Scale (PAIS), Mental Health Inventory (MHI), Impact of Event Scale, and Family Functioning Scale [16]. Other studies have used the EORTC QLQ-H&N 35 [17] and different depression scales e.g. Centre for Epidemiologic Studies Depression Scale (CES-D) and Illness intrusiveness ratings scale [18]. For a more generic description of HRQoL the EQ-5D has frequently been used. When oral health related quality of life is measured and compared between different groups, it is advantageous to use the same scale. OHIP-49 and different modification of this OHRQoL measure has been used for a number of different oral rehabilitation treatment modalities [11,19]. In a study by Özhayat 2011 [19] the OHIP-49 scores before treatment for patients without radiation therapy or ablative surgery was 35 for patients with FDP´s and 50 for RDP´s, respectively [19]. In the present study the mean OHIP-49 score was 77 before oral rehabilitation. Thus the starting point was worse in the present group of patients. On the other hand a high OHIP-score could be easier to improve than a low. In the present study the mean change or improvement was 37, whereas the improvement in the studies by özhayat was 20 for the RDP group and 13 for the FDP group [11].
The validity of the OHIP-49 for evaluating the patient-reported effect of oral rehabilitation with and without implants can be questioned for this group of patients. Thus, it has been found that items other than the ones in the OHIP-49 are important when performing interviews of the participants [20,21].
In studies examine treatments with RDP and FDP food catching and worried about the dental situation was the most frequently reported problems [11]. In the present study difficult chewing and avoiding eating some food were more prominent problems. Unclear speech was included in the ten most frequently reported problems both before and after treatment, whereas this was not an item in the top-ten for the RDPs and FDPs in the study by Özhayat and Gotfredsen [11]. This is not surprising as 10 of the patients underwent rehabilitation with obturators.
A number of studies have demonstrated an established relationship between satisfaction with the oral rehabilitation and personality profiles [15, 22]. Thus, psychological factors have a profound role in shaping patients satisfaction with oral rehabilitation and patients with higher levels of neuroticism will be less satisfied with dental treatment [22]. On the other hand, dental prostheses might be an important source of concern for the patients, and may affect their personality profile.
In summary, the present study demonstrated a significant improvement in OHRQoL after oral rehabilitation with fixed and removable dental prosthesis for patients after radiation and/or ablative jaw surgery. The variation between patients was, however, so large that more patients had to be included to demonstrate significant benefits of implants.
Acknowledgement
We would like to thank dental hygienist, Lisa Myung Pilegaard Hansen at the Department of Oral Rehabilitation, Faculty of Health and Medical Sciences at University of Copenhagen for helping with data collection and statistician Ulla Mogensen for help with the statistical analyses.
References
- Engholm G, Ferlay J, Christensen N, Storm HH, Pukkala E, et al. (2012) NORDCAN: Cancer Incidence, Mortality, Prevalence and Survival in the Nordic Countries, Version 5.1. Association of the Nordic Cancer Registries. Danish Cancer Society.
- Grau C (2012) General strategies for diagnosis and treatment of head and neck cancer in Denmark. Danish Dental Journal 116: 412-417.
- Matras R, Specht L, Hillerup S (2008) Removal of odontogenic infectious foci prior to radiation therapy for head and neck. Danish Dental Journal 112: 502-511.
- Vissink A, Jansma J, Spijkervet FK, Burlage FR, Coppes RP (2003) Oral sequelae of head and neck radiotherapy. Critical reviews in oral biology and medicine 14(3): 199-212.
- Danish Regions. Status for pakkeforløb på kræftområdet 2010.
- Chambrone L, Mandia J Jr, Shibli JA, Romito GA, Abrahao M (2013) Dental implants installed in irradiated jaws: a systematic review. J Dent Res 92(12 Suppl): 119S-130S.
- Pace-Balzan A, Shaw RJ, Butterworth C (2011) Oral rehabilitation following treatment for oral cancer. Periodontology 57(1): 102-117.
- Slade GD, Spencer AJ (1994) Development and evaluation of the Oral Health Impact Profile. Community Dent Health 11(1): 3-11.
- Mericske-Stern R, Mericske E, Berthold H, Geering AH (1994) [Resection prosthodontics. Aspects of the treatment of patients with oral defects following tumor resection--a retrospective study]. Schweizer Monatsschrift fur Zahnmedizin = Revue mensuelle suisse d'odonto-stomatologie = Rivista mensile svizzera di odontologia e stomatologia / SSO 104(1): 58-72.
- Locker D, Gibson B (2006) The concept of positive health: a review and commentary on its application in oral health research. Community Dent Oral Epidemiol 34(3): 161-173.
- Ozhayat EB, Gotfredsen K (2013) Oral health-related quality-of-life in patients to be treated with fixed or removable partial dental prostheses. Acta Odontol Scand 71(1): 113-119.
- Wostmann B, Budtz-Jorgensen E, Jepson N, Mushimoto E, Palmqvist S, et al. (2005) Indications for removable partial dentures: a literature review. Int J Prosthodont 18(2): 139-145.
- Owall B, Jonsson L (1998) Precision attachment-retained removable partial dentures. Part 3. General practitioner results up to 2 years. Int J Prosthodont 11(6): 574-579.
- Ihde S, Kopp S, Gundlach K, Konstantinovic VS (2009) Effects of radiation therapy on craniofacial and dental implants: a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107(1): 56-65.
- Al-Omiri MK, Karasneh J (2010) Relationship between Oral Health-Related Quality of Life, Satisfaction, and Personality in Patients with Prosthetic Rehabilitation. J Prosthodont 19(1): 2-9.
- Kornblith AB, Zlotolow IM, Gooen J, Huryn JM, Lerner T, et al. (1996) Quality of life of maxillectomy patients using an obturator prosthesis. Head Neck 18(4): 323-334.
- Fierz J, Burgin W, Mericske-Stern R (2013) Patients with oral tumors. Part 2: Quality of life after treatment with resection prostheses. Resection prosthetics:evaluation of quality of life. Schweizer Monatsschrift fur Zahnmedizin =Revue mensuelle suisse d'odonto-stomatologie = Rivista mensile svizzera diodontologia e stomatologia / SSO 123(3): 180-191.
- Irish J, Sandhu N, Simpson C, Wood R, Gilbert R, et al. (2009) Quality of life in patients with maxillectomy prostheses. Head Neck 31(6): 813-821.
- Ozhayat EB, Gotfredsen K (2012) Effect of treatment with fixed and removable dental prostheses. An oral health-related quality of life study. J Oral Rehabil 39(1): 28-36.
- Ozhayat EB, Gotfredsen K, Elverdam B, Owall B (2010) Patient-generated aspects in oral rehabilitation decision making. II. Comparison of an individual systematic interview method and the oral health impact profile. Int J Prosthodont 23(5): 421-428.
- Ozhayat EB, Gotfredsen K, Elverdam B, Owall B (2010) Comparison of an individual systematic interview method and the oral health impact profile. Responsiveness and ability of describing treatment effect of oral rehabilitation. J Oral Rehabil 37(8): 604-614.
- Al-Omiri MK, Lamey PJ, Cooper C, Clifford T (2006) Relationship between personality and satisfaction with the dentition in tooth wear patients. Eur J Prosthodont Restor Dent 14(4): 179-184.





