Establishing Post Orthodontic Norms for Incisor Positioning In South Indian Population Using Tetragon Analysis
Nitin V Muralidhar1*, Jyothi Kiran H2, Raghunath N3
1 Reader, Department of Orthodontics & Dentofacial Orthopaedics, JSS Dental College and Hospital, JSS Academy of Higher Education & Research
Karnataka, Mysuru � 570015, India.
2 Department of Orthodontics & Dentofacial Orthopaedics, JSS Dental College and Hospital, JSS Academy of Higher Education & Research, Karnataka, Mysuru � 570015, India.
3 Prof & Head of Department, Department of Orthodontics & Dentofacial Orthopaedics, JSS Dental College and Hospital, JSS Academy of Higher Education & Research, Karnataka, Mysuru � 570015, India.
*Corresponding Author
Nitin V Muralidhar, MDS,
Reader, Department of Orthodontics & Dentofacial Orthopaedics, JSS Dental College and Hospital, JSS Academy of Higher Education & Research Karnataka, Mysuru � 570015, India.
Tel: +9448413146
E-mail: dr.nitinvmuralidhar@jssuni.edu.in
Received: September 15, 2021; Accepted: November 28, 2021; Published: December 07, 2021
Citation: Nitin V Muralidhar, Jyothi Kiran H, Raghunath N. Establishing Post Orthodontic Norms for Incisor Positioning In South Indian Population Using Tetragon Analysis. Int J Dentistry Oral Sci. 2021;8(12):5197-5200. doi: dx.doi.org/10.19070/2377-8075-210001042
Copyright: Nitin V Muralidhar, MDS�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This study aims at providing ideal cephalometric norms to position the maxillary and mandibular incisors at the end of orthodontic
treatment in the ethnic south Indian population.
Materials and methods: 65 individuals having Class I malocclusion with bimaxillary protrusion were considered for this
study with 20 males and 45 females, who needed orthodontic treatment with extraction of all the first pre molars. Fastlitch�s
Tetragon analysis (U1-PP,U1-L1,L1-MP,MP-PP, Pt -Or /Pt -PNS, Pt-PNS/PP, PP- Pt/Or) was employed to identify the
changes brought about due to orthodontic treatment.
Results: The orientation of the maxillary incisors in the South Indian population was found to be similar to that of the norms
given by Fastlitch, but the Lower incisors were more proclined and as a result there was decreased interincisal angulation noted
and with a predominantly low angle individuals were noted.
Conclusion: This study provides the clinician a definitive end point to orient the maxillary and mandibular incisors in case of
ethnic south Indian population after orthodontic treatment.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Cephalometric Norms; Planned Incisor Positioning; Tetragon Analysis.
Introduction
The position of the upper central incisor plays a vital role in smile
esthetics, Ramos [1] Orthodontists rely on the normative values
based on cephalometric analysis ever since Broadbent [2] introduced
lateral cephalometric radiography in 1931. Inspite of the
norms most of the times it is not possible to achieve the ideal
incisor position as prescribed.
Only a skillful orthodontist with an artistic viewpoint will be able
to successfully place the incisors aesthetically. To support the
decision of the orthodontist, many researchers like Steiners [3],
Downs [4], Tweeds [5] and many others have put fort their analysis
for an ideal upper incisor position.
Steiner [3] was the one of the first researchers to imply that cephalometric
norms of one ethnic group need not necessarily be
applied to other ethnic groups. Gradually many researchers and
clinicians started noticing the variations in the normative values
in their respective population groups. Following which a number
of cephalometric analysis specific to their ethnic groups were put
forward like Paek�s [6] study of Korea population, Nanda�s [7]
study of north Indians, Garcia�s [8] study of the Mexican Americans
and so on. All these studies indicate that the normative values
of one ethnic group cannot be applied to the other groups
as normative values due to differences on facials patterns. Hence
customized cephalometric norms must be developed for each
ethnic group.
The principal aim of any analysis is to provide a simple, reliable
and reproduceable method. One such analysis was introduced by
Dr. Jorge Fastlicht [9] in the year 2000 known as the �Tetragon:
A Visual cephalometric analysis�. Since the Tetragon analysis was
carried out on Caucasian and White North American subjects
whose norms may differ with those of the ethnic Asian population,
hence this study was carried out on south Indian subjects
from Mysuru district, Karnataka, India, to find out the ideal cephalometric
parameters to position the maxillary and mandibular
incisors using the Tetragon analysis.
Aims & Objectives
To determine the normative values of maxillary and mandibular
incisor positioning using Tetragon analysis after orthodontic
treatment in South Indian Population.
Materials and Methods
The sample consisted of sixty-five individuals out which 20 were
males and 45 were females with an average age of 18-25 years.
Inclusion Criteria
Class I malocclusion with bimaxillary protrusion individuals.
Patients who needed fixed orthodontic therapy with extraction of
all first premolar teeth.
Subjects who are native of Mysuru district were selected for the
study.
Exclusion criteria
Subjects with craniofacial deformities.
Subjects requiring functional appliance therapy or orthopaedic
appliance therapy.
Subjects requiring orthognathic surgery for correction of jaw deformities.
Method of collecting the data
The patient�s pre-treatment and post-treatment cephalograms,
which were taken as a part of routine orthodontic treatment protocol,
were digitally analyzed using the Nemoceph software by a
single operator twice to avoid any operator variability. Due consent
was taken from the patients before commencing the study.
All the patients were treated with MBT 022� slot prescription.
Tetragon analysis was employed to decipher the pre-treatment
and post-treatment lateral cephalograms to evaluate the changes
in the orientation of incisors in relation to the jaw bases.
Tetragon (Fig 1&2)
U1-PP: The angle formed between the palatal plane (PP) with the
long axis of the maxillary central incisors.
U1-L1: Angulation between the long axis of maxillary and the
mandibular central incisors.
L1-MP: Angulation of the mandibular incisor long axiswith the
mandibular plane.
MP-PP: Angulation between the mandibular plane and the PP.
According to Fastlicht�s analysis, the Tetragon comprises of four
sides, forming four angles which will add upto 360�. If any of
the angle sare modified, either by growth or by orthodontic treatment,
the angles of the Tetragon will tend change, but their sum
will still remain 360�. In the advent that the angles are not adding
upto 3600, an inference can be inferred that either that the tracing
is inaccurate or that one or more angles have been calculated
incorrectly.
TRIGON (Fig 3)
Pt.-Or/Pt-PNS: Angulation between Pt-Or plane and Pt-PNS
plane.
Pt.-PNS/PP: Angulation between the Pt-PNS and the PP.
Pt.-Or/PP: Angulation between the Pt.-Or plane and the PP.
The Trigon consists of three sides, with three angles that will add
up to 180�. In any case, these 3 angles must always be 180�.
In a scenario where the Palatal plane and the Pt-Or plane are parallel,
theangulation between these two planes will be neutral or 0�,
but the sum of the remaining two r angles will still be 180�.
Statistical analysis used: Descriptive analysis � Mean and standard
deviation was used and Paired T-test was used to compare the
pre and post treatment changes.
Results
Paired t-test was used to compare between standard mean values
and post treatment values. It was observed that there was significant
difference between the standard mean values and post
treatment values of the mandibular plane to the palatal plane
(Go-Gn to PP), lower incisor inclination to the mandibular plane
(L1-IMPA) and the interincisal angulation (U1-L1) with p<0.05.
But there was no significant difference observed between standard
mean values and post treatment values of the upper incisor
inclination to the palatal plane (U1 to PP) with p value 0.511.
There was no difference between both males and females across
all parameters. (Table 1)
The Trigon values of the Pt-Or plane and Pt-PNS angle the Pt-
PNS/PP plane angle was statistically significant and the Pt-Or-PP
angle was not statistically significant. (Table 2)
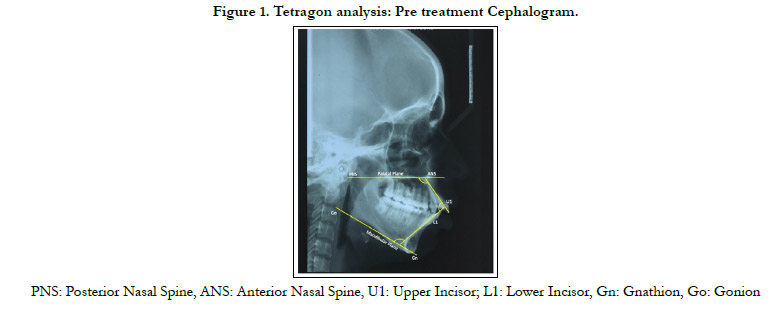

Figure 1. Tetragon analysis: Pre treatment Cephalogram.
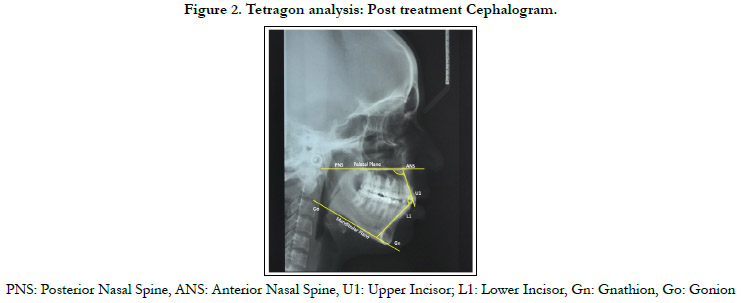
Figure 2. Tetragon analysis: Post treatment Cephalogram.
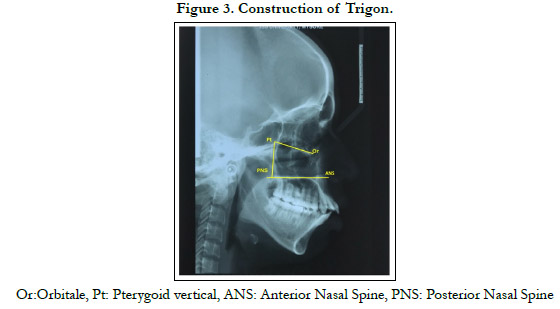
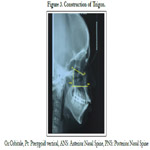
Figure 3. Study flow chart.
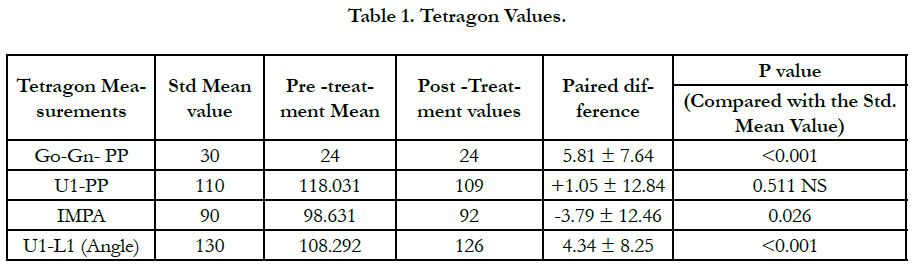

Table 1. Tetragon Values.
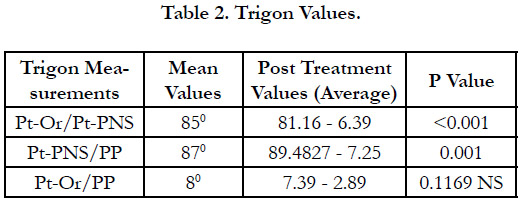
Table 2. Trigon Values.
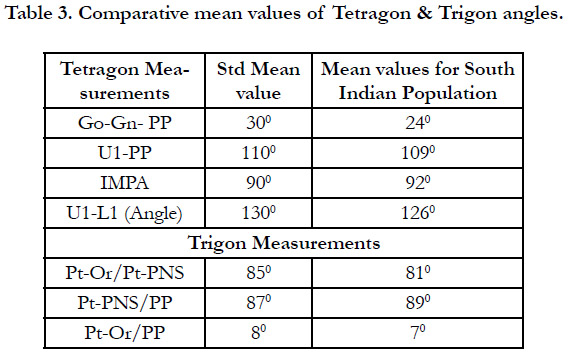
Table 3. Comparative mean values of Tetragon & Trigon angles.
Discussion
In this study the maxillary incisor inclination to the palatal plane
(U1-PP) after the treatment was similar to the values of Fastlicht
[9]. However, the study conducted by John and Valiathan [10]
(1991) found increased proclination of the maxillary incisors in
case of Class II individuals. The reason maybe the difference in
type of malocclusion chosen for the study.
The interincisal angulation (U1-L1) was decreased and is statistically
significant as this value is dependent on both the maxillary
and mandibular incisor inclinations and maxillary incisor retraction
was more contributory towards increasing the interincisal incisor retraction.
In this study the value of the mandibular plane to the palatal plane
(Go-Gn-PP) shows statistically significant when compared with
the normative values but exhibited no change when compared
with the pre-treatment values. This indicates that there was no
alteration of dentition in the vertical dimension.
The Trigon values of Pt -Or /Pt -PNS and Pt-PNS/PP showed
statistically significant values but not clinically significant as there
was no major Orthopaedic treatment carried out like myo-functional
therapy and the palatal plane to the Pt-Or plane did not exhibit
any significant change indicating no alteration of the skeletal
jaw bases in the vertical dimension.
This study was conducted only on individuals having Class I malocclusion
with bimaxillary protrusion. Further studies with must
be carried out with a larger sample size and across all types of
malocclusions to derive the cephalometric norms for the Indian
population. Table 3.
Summary & Conclusion
According to this study the South Indian population exhibited a
more proclined mandibular incisors than the maxillary incisors
when compared to the established norms and accordingly there
was increased interincisal angulation. The study also revealed that
the South Indian Population exhibited a predominantly horizontal
growing individuals as compared to the Caucasian population.
References
-
[1]. Ramos AL, Sakima MT, Pinto Ados S, Bowman SJ. Upper lip changes correlated
to maxillary incisor retraction--a metallic implant study. Angle Orthod.
2005 Jul;75(4):499-505. PubMed PMID: 16097216.
[2]. Broadbent BH. A new x-ray technique and its application to orthodontia. The Angle Orthodontist. 1931 Apr;1(2):45-66.
[3]. Steiner CC. Cephalometrics for you and me. American journal of orthodontics. 1953 Oct 1;39(10):729-55.
[4]. DOWNS WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod. 1948 Oct;34(10):812-40. PubMed PMID: 18882558.
[5]. Tweed CH. The Frankfort-mandibular incisor angle (FMIA) in orthodontic diagnosis, treatment planning and prognosis. The Angle Orthodontist. 1954 Jul;24(3):121-69.
[6]. Park IC, Bowman D, Klapper L. A cephalometric study of Korean adults. Am J OrthodDentofacialOrthop. 1989 Jul;96(1):54-9. PubMed PMID: 2750721.
[7]. Nanda R, Nanda RS. Cephalometric study of the dentofacial complex of North Indians. Angle Orthod. 1969 Jan;39(1):22-8. PubMed PMID: 5250522.
[8]. Garcia CJ. Cephalometric evaluation of Mexican Americans using the Downs and Steiner analyses. Am J Orthod. 1975 Jul;68(1):67-74. PubMed PMID: 1056145.
[9]. Fastlicht J. Tetragon: A visual cephalometric analysis. J ClinOrthod 2000;34(6):353-60.
[10]. John KK, Valiathan A. Steiner�s analysis on adults from Kerala with normal, Class II and Class III occlusions�a comparison. J IndOrthod Soc. 1991;22:13-9.
[11]. Basciftci FA, Usumez S. Effects of extraction and nonextraction treatment on class I and class II subjects. Angle Orthod. 2003 Feb;73(1):36-42. Pub- Med PMID: 12607853.
[12]. Broadbent Jr BH, Golden WH, BROWN RG. Bolton standards of dentofacial development growth. Plastic and Reconstructive Surgery. 1977 Jan 1;59(1):115.
[13]. Riolo ML, Moyers RE, McNamara JA, Hunter AS. An Atlas of Craniofacial Growth, Centre for Human Growth and Development, University of Michigan. Ann Arbor, Michigan. 1974.
[14]. Schwarz AM.Roetgenostatics: A practical evaluation of X -ray headplate. Am J Orthod. 1961;47:561-585.





