The Effectiveness Of Laser Radiation On Curved Root Canals: A Review Study
Priyadarshini SK1*, Sathasivasubramanian S2, Murali V3
1 Lecturer, Department of Oral Medicine & Radiology, Dhanalakshmi Srinivasan Dental College and Hospitals, Perambalur � 621113, India.
2 Former HOD � Department of Oral Medicine & Radiology and Former Vice-principal - Sri Ramachandra Faculty of Dental sciences, Sri Ramachandra University, Porur, Chennai � 600116, India.
3 Chief Medical Physicist cum RSO, Apollo Speciality Hospitals, 320 Padma complex, Teynampet, Chennai- 600035, India.
*Corresponding Author
Dr. Priyadarshini S K MDS,
Lecturer, Department of Oral Medicine & Radiology, Dhanalakshmi Srinivasan Dental College and Hospitals, Perambalur � 621113, India.
Tel: 09944038464
E-mail: priya_kedar@yahoo.co.in
Received: October 08, 2021; Accepted: November 25, 2021; Published: November 30, 2021
Citation: Priyadarshini SK, Sathasivasubramanian S, Murali V. Measurement Of Surface Dose To The Thyroid Gland In Intraoral Radiography. Int J Dentistry Oral Sci. 2021;8(11):5175-5178. doi: dx.doi.org/10.19070/2377-8075-210001039
Copyright: Dr. Priyadarshini S K MDS�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Intra-oral periapical radiographs are the most frequently requested radiographic examination and an indispensable
tool in the diagnosis of dental diseases. The repeated exposures to these radiographic examinations pose a risk especially
to the thyroid gland due to the proximity to dental structures. This study was conducted to evaluate the surface dose received
by the thyroid gland during intra-oral periapical (IOPA) radiographic exposures.
Aim: To measure the entrance surface dose to the thyroid gland and compare the mean surface dose received by the thyroid
during maxillary and mandibular anterior & posterior intraoral periapical radiography.
Materials & methods: The study comprised 64 participants. Thermoluminiscent dosimeter (TLD) cubes were used to measure
the surface dose to the thyroid gland. The dose recorded by the TLD-s were measured using Harshaw 4500 TLD reader.
Results: The mean surface dose to the thyroid gland was high during maxillary anterior and posterior quadrants compared to
mandibular anterior and posterior radiographic exposures.
Conclusion: The surface dose received by the thyroid gland during intraoral radiography may be considered low but the frequency
of such exposures may pose a risk to the radiosensitive thyroid gland. Therefore, the thyroid gland should be protected
during routine IOPA radiographic techniques.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Thyroid Surface Dose; Dosimetry; Thermoluminescent Dosimeter; Intra-Oral Periapical Radiography.
Introduction
Imaging plays an integral part in the diagnosisand treatment planning
in dental practice.Dental radiographs comprise the most frequent
diagnostic radiographic examination [1] and among them
intra oral radiographs are the most common and frequently taken
radiographs.[2] The purpose of these examinations range from
diagnostic, restorative purpose, to treatment planning and follow
up. Although the exposure from dental x-rays are minimal the
radiographic examination should be justified and the principle
of �As low as reasonably achievable� should be followed as repeated
exposure to low-dose radiation may also result in deleterious
stochastic effects. The salivary glands and the thyroid gland
are considered the organs at risk in dental radiographyas they
are close to the dental structures. Particularly the thyroid gland
is the prime and most radiosensitive organ in dental radiography
especially during intra-oral radiography of the maxillary anterior
region as it is present within the primary x-ray beam and has high
susceptibility to radiation induced carcinogenesis.[3, 4] Although
it is considered that the radiation dose from dental radiology is
minimal the unwarranted and repeated exposure of this gland
during dental radiographic procedures may lead to thyroid dysfunction
resulting in autoimmune thyroiditis and papillary thyroid
carcinoma in young women and also thyroid cysts in women of
all ages.[3]Although with increasing age at exposure the risk of
radiation induced thyroid cancer decreases,[5] thyroid protection
is recommended in dental radiography when it does not interfere
with the exposure and the quality of the image.[6]
The aim of the study is to measure the entrance surface dose
to the thyroid during intra oral periapical (IOPA) radiographic procedures.
By measuring and comparing the entrance surface radiation dose
to the thyroid gland in intra oral periapical radiographic exposures
of the different quadrants we come to know the amount of radiation
that will reach the thyroid gland, and stress upon the need for
protecting the thyroid gland in routine dental practice.This study
will give us more knowledge on the surface dose to the thyroid
gland in routine diagnostic intra oral periapical radiographic exposures.
Materials And Methods
This was an observational study. Institutional ethical approval was
obtained prior to the study. A total of 64 subjects participated in
the study.Subjects were chosen so that they are equally distributed
in maxillary and mandibular posterior quadrants in right and left
side and in maxillary and mandibular anterior regions.Thermoluminescent
dosimeter (TLD) 100 (LiF:Mg,Ti) cubes of size 3mm
x 3mm x 1mm sealed and numbered in plastic foils were usedto
measure the entrance surface dose. Adult size 2, E speed films and
Satelec X-Mind intra oral x ray machine, circular collimator with
70 Kvp, 8mA was used for the study. Patients above the age of 20
years only were included in the study. Patients were not subjected
to any additional radiation and only those patients who were requested
for a diagnostic radiograph were included. Pregnant and
trauma patients were excluded from the study. The details of the
patient, the TLD number respective to the right and left side was
noted in the proforma tailored for the study.
The location of the thyroid gland was noted and two TLD�s were
placed over the thyroid collar with an adhesive tape in relation to
the right and left lobe of the thyroid respectively. The x-rays were
exposed using bisecting angle technique and the exposure time
for the anterior teeth was set to 0.6 seconds and for the posterior
teeth 0.8 seconds. After making the exposure the dose received
by the TLD was measured using Harshaw 4500 TLD reader. The
readings were done within 24 hours after exposure and the exposed
TLD-s were annealed before re-using.
Results
Statistical Analysiswas done using Independent t-test for comparing
the mean between the different groups.The mean surface dose
in anterior quadrants was 0.626 mGy and in posterior quadrants
was 0.669 mGy. On comparing the mean dose to the posterior
and anterior regions the P value is 0.757 which is not statistically
significant (Table 1). The mean dose during the maxillary anterior
exposures was 0.755mGy and during the mandibular anterior
exposures was 0.498mGy. On comparing the mean between the
upper and the lower anterior exposures the P value was 0.118
which was not statistically significant (Table 2). The mean surface
dose in relation to the maxillary posterior was 0.763 mGy and in
mandibular posterior was 0.574 mGy. On comparing the mean
doses, the P value was 0.399 which was statistically not significant
(Table 3). The mean surface dose in Right maxillary posterior was
0.659 mGy, Right mandibular posterior was 0.443 mGy with a P
value of 0.387 which was not statistically significant. The mean
surface dose to the Left maxillary posterior was 0.867 mGy and
left mandibular posterior was 0.706 mGy with a P value of 0.675
which was not statistically significant (Table 4).
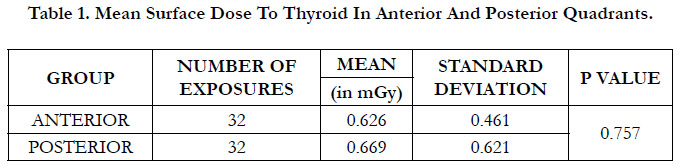

Table 1. Mean Surface Dose To Thyroid In Anterior And Posterior Quadrants.
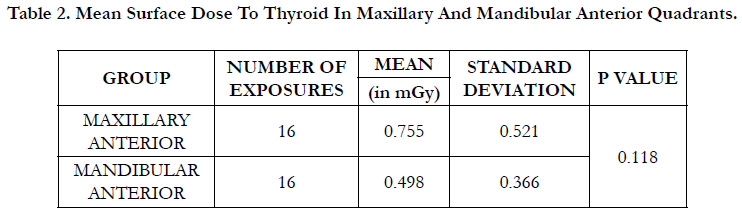
Table 2. Mean Surface Dose To Thyroid In Maxillary And Mandibular Anterior Quadrants./strong>
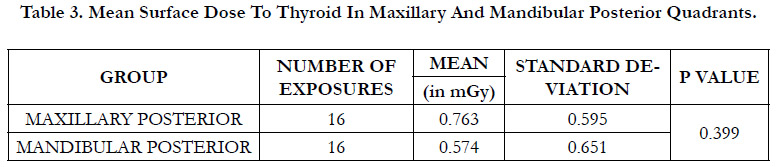
Table 3. Mean Surface Dose To Thyroid In Maxillary And Mandibular Posterior Quadrants.
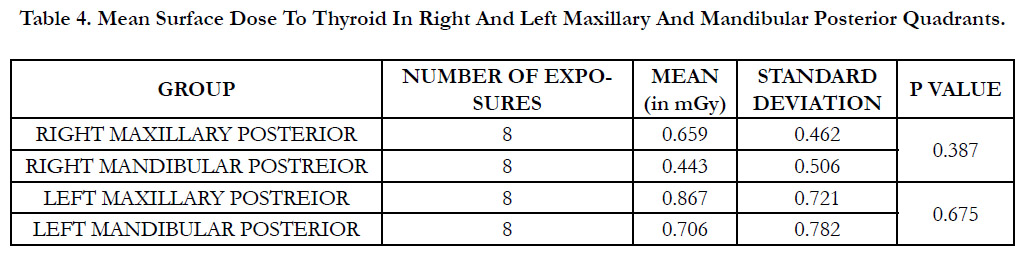
Table 4. Mean Surface Dose To Thyroid In Right And Left Maxillary And Mandibular Posterior Quadrants.
Discussion
Dental radiographs are an effective and imperative aid in the
diagnosis and management of various dental and oral diseases.
Although the radiation dose received from dental radiography is
low, low dose is not considered �safe dose� and a higher lifetime
prevalence and frequency of exposure can result in deleterious
stochastic effects, especially to the thyroid gland due its high radio-sensitivity and anatomic position.The only established environmental
risk factor for developing thyroid cancer is exposure
to moderate to high dose ionizing radiation. Repeated exposure
to low doses of ionizing radiation by dental radiographs has also
been associated with an increased risk of thyroid abnormalities
and thyroid cancer.[3, 7] Thus it is important for the dental practitioner
to justify the need of dental x-ray and optimise the patient
dose to ensure radiation protection.
In the present study the surface dose at the level of thyroid region
was evaluatedin routine diagnostic singlediagnostic intra oral
periapical radiograph of anterior and posterior quadrants and
their mean dose was compared.TLD-100 (LiF:Mg,Ti) was used
for measuring the dose, which is the recommended and most
commonly used thermoluminescent material for measuring the
entrance surface dose.[8] For the posterior IOPA exposures, the
dose received by the TLD nearest to the x ray source was taken
for statistical analysis, as the dose to the thyroid gland is mainly
related to the direction of the x-ray source.[9] For the anterior
IOPA exposure, the maximum dose received was considered for
statistical analysis.
According to the International Commission on Radiological Protection
(ICRP) the reference level for the entrance surface dose in
intra oral periapical radiography is 7mGy.[10]
In this study the mean entrance surface dose to the thyroid gland
in maxillary anterior and posterior IOPA exposures was high
compared to the mandibular quadrants.However, the difference
in the mean doses was not statistically significant.The mean surface
dose to the thyroid in this study was also less compared to
the results of the previous studies carried out in intra-oral radiography.
Mortazavi et al measured the surface dose to the skin
for the maxillary and mandibular IOPA exposures using 70Kvp,
7mA with exposure time of 0.16 to 0.41 seconds to be ranging
from 0.01 to 0.40mGy. [11] B.Poppe et al reported the entrance
surface dose in intra oral periapical radiographic exposures with
50Kv to 70Kv to be ranging from 1.2 to 2.7mGy. [12] Sheikh et
al calculated the entrance surface dose to the thyroid using pocket
dosimeter in full mouth intra oral periapical radiography by the
bisecting angle technique to be 1.093mGy and maxillary occlusal
radiography to be 0.15mGy. The surface dose to the thyroid at the
level of right lobe was 1.39mGy and at the level of the left lobe
was 1.2mGy. The exposure parameters that they used was 65Kvp,
10mA at 1 second. [13] Jibiri et al measured the entrance surface
dose to the skin of the eyes, parotid glands and thyroid gland during
intra oral radiography. The mean entrance surface dose to the
thyroid gland was 0.1869 � 0.082mGy. [14]
In this study, the entrance surface dose to the thyroid during anterior
IOPA ranged from 0.106mGy to 1.848 mGy and the surface
dose during posterior IOPA ranged from 0.126mGy to 1.997
mGy.
The entrance surface dose to the thyroid in maxillary anterior
ranged from 0.203mGy to 1.848mGy and maxillary posterior region
ranged from 0.143mGy to 1.917mGy.
The entrance surface dose to the thyroid in mandibular anterior
ranged from 0.106mGy to 1.229mGy and mandibular posterior
ranged from 0.126mGy to 1.997mGy.
Most of the previous studies have evaluated the entrance surface
dose to the thyroid, using panoramic radiography and full mouth
intra oral periapical radiography however there is no data evident
about comparison of the entrance surface dose to the thyroid
in anterior and posterior intra oral periapical radiography in patients.
In the present study, the entrance surface dose to thyroid
gland was measured for single diagnostic intra oral periapical radiograph
of anterior and posterior quadrants and their mean dose
was compared.
Conclusion
The results of the study reveal that the surface dose at the thyroid
level in intraoral periapical radiography is well below the reference
level given by ICRP 2001. However, repeated exposure to low
dose radiation such as dental x-rays cannot be neglected. Owing
to the high radiosensitivity of the thyroid gland and it�s position
- regardless of the region exposed, the thyroid gland has to be
protected in routine dental practice.
References
-
[1]. Horner K. Radiation protection in dental radiology. Brit J Radiol. 1994
Nov;67(803):1041-9.
[2]. Kalinowski P, R�zylo-Kalinowska I, R�zylo TK. Demographic structure of patients taking dental X-rays in the Lublin region. Ann Univ Mariae Curie Sklodowska Med. 2001;56:431-5. PubMed PMID: 11977354.
[3]. Memon A, Godward S, Williams D, Siddique I, Al-Saleh K. Dental xrays and the risk of thyroid cancer: a case-control study. Acta Oncol. 2010 May;49(4):447-53. PubMed PMID: 20397774.
[4]. Crane GD, Abbott PV. Radiation shielding in dentistry: an update. Aust Dent J. 2016 Sep;61(3):277-81. PubMed PMID: 26644147.
[5]. Kleinerman RA. Cancer risks following diagnostic and therapeutic radiation exposure in children. Pediatr Radiol. 2006 Sep;36 Suppl 2(Suppl 2):121-5. PubMed PMID: 16862418.
[6]. American Dental Association Council on Scientific Affairs. The use of dental radiographs: update and recommendations. J Am Dent Assoc. 2006 Sep;137(9):1304-12. PubMed PMID: 16946440.
[7]. Memon A, Rogers I, Paudyal P, Sundin J. Dental X-Rays and the Risk of Thyroid Cancer and Meningioma: A Systematic Review and Meta-Analysis of Current Epidemiological Evidence. Thyroid. 2019 Nov;29(11):1572- 1593. PubMed PMID: 31502516.
[8]. Mantuano ND, Canevaro LV, Maur�cio CL, CA S. Assessment of dose in thyroid and salivary glands in dental radiology using thermoluminiscent dosimetry. International nuclear Atlantic conference 2011. [9]. Burke K, Sutton D. Optimization and deconvolution of lithium fluoride TLD-100 in diagnostic radiology. Br J Radiol. 1997 Mar;70:261-71. Pub- Med PMID: 9166051.
[10]. Diagnostic reference levels in medical imaging: review and additional advice. Ann ICRP. 2001;31(4):33-52. PubMed PMID: 12685758.
[11]. Mortazavi SM, Shareghi A, Ghiassi-Nejad M, Kavousi A, Jafari-Zadeh M, Nazeri F, Mozdarani H (2004). The need for national diagnostic reference levels: Entrance surface dose measurement in intraoral radiography. Iran J Radiat Res 15(2):127-33.
[12]. Poppe B, Looe HK, Pfaffenberger A, Eenboom F, Chofor N, Sering M, R�hmann A, Poplawski A, Willborn K. Radiation exposure and dose evaluation in intraoral dental radiology. Radiat Prot Dosimetry. 2007;123(2):262-7. PubMed PMID: 16971397.
[13]. Sheikh S, Bhoweer AK, Arya S, Arora G. Evaluation of surface radiation dose to the thyroid gland and the gonads during routine full-mouth intraoral periapical and maxillary occlusal radiography. Contemp Clin Dent. 2010 Apr;1(2):83-7. PubMed PMID: 22114389.
[14]. Jibiri N, Adeleye B, Kolude B (2017). Radiation dose to the thyroid, eyes and parotid glands of patients undergoing intra-oral radiographic procedures in a teaching hospital in Ibadan, Oyo state Nigeria.Int J Radiat Res. 15(1):101-106.





