The Effectiveness Of Laser Radiation On Curved Root Canals: A Review Study
Farshad Khosraviani1*, Mojgan Danyal Khosravi2, Tara Azimi3
1 D.D.S, University of California Los Angeles, School of Dentistry, California, USA.
2 Student Doctor, Arizona School of dentistry& Oral Health, Arizona, USA.
3 D.D.S, Shahid Beheshti University of Medical Sciences, School of Dentistry, Tehran, Iran.
*Corresponding Author
Farshad Khosraviani,
D.D.S, University of California Los Angeles, School of Dentistry, California, USA.
E-mail: farshad.khosraviani@g.ucla.edu
Received: June 26, 2021; Accepted: November 17, 2021; Published: November 29, 2021
Citation: Farshad Khosraviani, Mojgan Danyal Khosravi, Tara Azimi. The Effectiveness Of Laser Radiation On Curved Root Canals: A Review Study. Int J Dentistry Oral Sci. 2021;8(11):5168-5174. doi: dx.doi.org/10.19070/2377-8075-210001038
Copyright: Farshad Khosraviani�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Laser has an effective role in endodontic treatment. Most studies have examined the effects of laser radiation
on straight canals. The aim of this study was to review the therapeutic effect of laser radiation on curved root canals.
Methods: First, the related keywords were searched in four databases: Scopus, PubMed, WOS and Google Scholar. After
merging the collected titles, original eligible articles published by the end of February 2021 were scrutinized.
Results: Out of 16 collected titles, 10 articles met the study criteria. The lasers used included Er, Cr: YSGG (2780 nm), Nd:
YAG (1064 nm), Er: YAG (2940 nm) and diode (660,940,980 nm). The canal curvature in 6 studies was between 5-33�. Also,
the degree of curvature was described > 20� in three studies, and in one study it was 31� 9�. Therapeutic goals of laser irradiation
included root canal shaping, smear layer removal, anti-enterococcus faecalis and anti-candida albicans effect, levels of
filler and sealer penetration into dentin tubules. The results of the studies showed that the laser radiation was not effective for
curved root canal shaping; however, it was effective on other mentioned purposes compared to the control group.
Conclusion: Radiation of the above lasers in curved canals, despite the weakness in canal shaping, can be effective as an
adjuvant tool for canal cleaning, disinfecting and sealing improvement.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Laser; Curved Canal; Endodontics; Root Canal; Review.
Introduction
Proper shaping, cleaning and disinfecting and then achieving a
strong seal by obstructing the root canal system are essential steps
of a successful endodontic treatment [1].
The anatomical features of the root canal affect the success of
its treatment. Curved canals create constraints for proper biomechanical
preparation and sealing [2, 3]. These constraints are more
pronounced for canals with sever curvature [4, 5]. Fractures of
endodontic instruments, perforation, filling defects, buildup of
elbow or zip, failing to achieve the working length and defect in
debris removal are some of these constraints [4, 5] which lead
to infection, relapse of symptoms, and sometimes a re-treatment
[6]. Depending on the type of curvature measurement methods,
a varied prevalence of curved canals has been reported in studies.
Generally, this prevalence varies between 5 to 95% [7-9].
The use of manual steel files has a significant weakness in the
preparation of curved canals and in some cases the desired canal
shape and debris removal are achieved less than is expected [10,
11]. Although, Ni-Ti manual files have reduced the problems of
steel manual files, but they have not completely eliminated the disadvantages
of steel manual files [12]. Rotary instruments are more
effective than manual ones in preparing the curved canal. Rotary
instruments, by reducing the canal preparation time, reducing the
possibility of entrapment and fracture of the instrument inside
the canal, and preparing the canal with the optimal radius, provide
an easier and safer process for the dentist [12-14]. However, rotary
instruments are not completely effective in removing debris from
the root canal, and the use of adjuvant modalities may provide a
more appropriate treatment in their biomechanical preparation.
Laser radiation has found various applications in endodontic
treatment. Antibacterial effects, canal shaping, smear layer removal,
irritants activation and canal sealing are some of its advantages in endodontic treatment [15-19]. In addition, unlike conventional
irritants such as EDTA, laser does not result in an allergic reaction
and may be a good alternative choice for people who are allergic
to these substances [20, 21]. The effects of laser during endodontic
treatment depend on the type of laser, radiation setting and
canal morphology, and changes in any of these items can change
the treatment outcome [22].
Most studies have evaluated the effect of lasers on direct canals
and fewer findings are available on the use of lasers on curved canals
[23, 24]. The aim of this review was to evaluate the effectiveness
of laser irradiation on the treatment of curved root canals.
The results of this study can provide a summary of the available
evidence in this regard.
Methods
First, the following keywords and phrases were extracted using
MeSH and related articles. These were then searched in three databases:
Scopus, PubMed, and WOS.
(laser OR "laser radiation" OR "photodynamic therapy" OR "light
therapy") AND ("curved root canal" OR "root canal curvature")
The collected titles in the above databases were limited to original
articles published by the end of February 2021. The titles were
then combined electronically with Mendeley desktop software
(ver 1.19) to remove duplicates. Also, to increase the search scope,
the keywords were searched in the Google Scholar database, and
the 200 initial titles displayed were checked and non-duplicate related
titles were added to the search results.
Titles were submitted electronically to two reviewers (A.A & B.B)
to select eligible articles. If there were no consensus between
the two reviewers on some of the titles, the third reviewer (C.C)
would decide on them.
Inclusion criteria included original articles, laser radiation, use of
root canals with a curvature of at least 5�, and in-vivo and ex-vivo
studies. Exclusion criteria included non-English language articles,
lack of access to the full text of articles, case report studies, studies
without control groups, and deficiencies in methodology or
result reporting.
Eligible articles were thoroughly examined by the third reviewer
and the results were extracted. Necessary information was extracted
from the articles including the type of study, the type of
tooth, the amount of canal curvature, the type of laser and its radiation
conditions, the therapeutic goals of laser radiation and its
effectiveness results. The effectiveness of the laser was reported
as effective (E) where a significant difference was observed with
the negative control group or where there was not a significant
difference in the positive control group, and was reported as
ineffective(I) if there was no significant difference in the negative
control group.
CONSORT 2010 Checklist was used to assess the quality of the
clinical trial studies 17. This checklist consists of 37 items. The
number of items obtained by each article is divided into total
items and expressed as a percentage. Cochrane Collaboration's
tool was used for assessing the risk of bias in the clinical trial
studies 18. Risk of bias was described as high (H), low (L), and
unknown (U). To the best of our knowledge, there was not a
qualified checklist to assess the quality and risk of bias in laboratory
studies. However, the use of inclusion and exclusion criteria
in selecting the articles could have greatly reduced the risk of bias
in this study.
Results
Search Results
Figure 1 shows a summary of the article selection process. 22
titles were found in three databases: Scopus, PubMed, and WOS.
22 titles were found, leaving 12 titles after deleting duplicate titles.
Four non-duplicate titles were also found on the Google Scholar
database. In the initial evaluation, 3 articles out of 16 titles were
excluded from the study the reasons for which are given in Figure
1. Out of the remaining 13 titles, one study was excluded due to
the use of resin block model to simulate the root canal, one study
due to the evaluation of thermal changes of laser radiation (nontherapeutic
intervention) and one study due to lack of access to
its full text. At the end, ten articles were thoroughly reviewed.
Table 1 shows a summary of the final ten articles.
Type of studies
All studies were performed on extracted human teeth in the laboratory.
Laser and radiation conditions
In studies lasers of 2780 nm Er, Cr: YSGG, [25, 26, 29, 34], 2940
nm Er: YAG [27, 33], 1064 nm Nd: YAG [27, 28, 33], and diodes
of 660 nm [30, 32], 940 nm [34] and 980 nm [31] were used. One
study used a combination of Er, Cr: YSGG - Diode lasers [34]. In
two studies, the diode laser was irradiated in the form of photodynamic
therapy (PDT) [30, 32]. Only five studies reported laser
radiation energy, which ranged from 25 to 150 mJ [27-29, 33] for
Er: YAG, Er, Cr: YSGG, and Nd: YAG lasers and 36 J for diode
lasers [30]. The range of radiation power in the studies varied
from 0.1 to 2 w.
Studies used specific laser endodontic fiber. In general, the fibers
were moved in upward- downward motion inside the canal.
The fiber diameters in the studies were 200, 300, 320, 400, 600
micrometers. In one study, the diode laser fiber ranged from 0.3
to 1 mm in diameter from base to tip [30].
Canal curvature
In one classification, the curvature of the evaluated canals was
5 to 15 � in three studies [25-27], and 15 to 33 � in three other
studies [29, 30, 32]. Also, three studies in their report used canals
with a curvature of more than 20� [28, 31, 33] and one study
used canals with an average curvature of 31 � 9� [34]. Six studies
determined the curvature of the canal with the Schneider method
and in other studies the method of measuring the curvature was
not mentioned [25, 32-34].
Endodontic treatment models
Canal shaping in two studies [25, 26], smear layer removal in five studies [25, 26, 29, 33, 34], antibacterial effects using Enterococcus
faecalis in two studies [27, 32], sealer penetration into dentin
tubules in two studies [28, 33], canal occlusion in one study [31]
and anti- Candida albicans effect in one study [30] were the subjects
of the studies.
Effectiveness
Laser radiation in nine studies in comparison to the negative control
group or the positive control group had effective and significant
therapeutic results, generally. In addition, in two studies laser
irradiation was effective for smear layer removal and was ineffective
for canal shaping [25, 26]. In one study, diode laser radiation
in the form of PDT did not show the appropriate antibacterial
effect compared to NaOCl [32]. Below is a summary of the main
results of the reviewed studies.
Canal shaping
Matsuka et al., in order to prepare root canals using Er, Cr: YSGG
laser, divided 20 mandibular incisor teeth into 10 and 15 degree
curvature groups. Canal preparation was done using laser irradiation
and air and water spray. First the 200 �m and then the
320 �m fiber entered the canal and then irradiation was done. In
stereoscope and SEM images, the laser in the 10�curvature group
produced superficial surface roughness without carbonization or
melting. In the 15 � curvature group, carbonization, longer irradiation
time, perforation and pseudo-canal formation were observed.
Such problems were fewer with the 200 �m fiber compared
with the 320 �m one. Also, in the curvature group of 15 �,
in order to reach the working length, the 320 �m fiber had been
broken in some cases [25].
Jahan et al., Considering the degree of curvature greater than 5
� as a curved canal, and a curvature less than or equal to 5 � as a
direct canal, divided 40 molars into two groups of 20 performed
two types of preparatory interventions. The first group experienced
Er, Cr: YSGG laser irradiation without the use of an irrigant,
and the second group canal preparation with K files with
5.25%NaOCl and 3% H2O2. Irradiation setting included a power
of 2 w, a frequency of 20 Hz and 200, 320 and 400 micrometer
fibers for the apical, middle and coronal areas. In the stereoscope
and SEM images, the error rate including hyper-instrumentation
and edge and pseudo-canal creation was more observed in
the laser group. The success rate of reaching the working length
in the direct canal in the laser and control group was 100%, and
in the curved canals in the distal regions these rates were 62.5%
and 71.4% in the laser and control groups respectively, which
were not significantly different from each other. [26].
Smear layer removal
Nasher et al. investigated the simultaneous irradiation of two Er,
Cr: YSGG-diode 940 nm lasers in smear layer removal in cannals
with an average curvature of 31 � 9�. After preparing the canal
with a rotary instrument, the canals were divided into five groups:
1. Negative control group in which canals were only rinsed by
tap water, 2. Positive control group (17% EDTA and a final rinse
of 3% NaOCl), 3. Conventional group (with XP Endoshaper
and finisher with 17%EDTA), 4. Dual laser radiation of Er, Cr:
YSGG (1.25 W) and diode 940 nm (2 W) and 5. Dual laser radiation
group of Er, Cr: YSGG (2 W) and diode 940 nm (2 W).
In microscopic laser scan images, all interventions removed the
smear layer significantly compared to the control group. The laser
group had better and more significant results than the positive
control group but had not any significant differences with
the conventional group. The fifth group produced the best result.
Also, group five showed a significantly better performance
than group four. In group four of Er, Cr: YSGG laser with 1.25
w power, complete smear layer removal was observed in cervical
and middle areas, but in apical areas, smear layer removal was
poor. In their other findings, the use of an intracanal entry cycle
in the fifth group compared to the four entry cycles in group four
provided protection against laser fiber breakage [34].
Sabari Murugesun et al., evaluated the effect of flat and conical
fiber tip on smear layer removal from the root canal of mandibular
premolars with a curvature of 15 to 30�. They first prepared
81 canals with rotary files and devided them in three groups of 27
of 17% EDTA, 3% NaOCl, and CHX. Each group was divided
into three subgroups of 9, including without laser irradiation, and
Er, Cr: YSGG laser irradiation with flat and conical tip. The laser
was irradiated on the irrigants for 5 seconds. In the findings,
by examining the apical third region using SEM images, the subgroups
without laser irradiation did not differ from each other in
the amount of smear layer removal and there remained significant
amounts of debris. The group without laser radiation was not
significantly different from the laser group with smooth tip fiber.
In the group of lasers with conical tip, 17% EDTA had a better
performance than the other two irrigants of CHX and NAOCL.
In comparing the conical tip group with the control group and the
flat type group, smear layer removal with the help of EDTA17%
activation showed the best results [29].
In other findings by Matsouka et al., Er, Cr: YSGG laser irradiation
in the 10� curvature group, smear layer was well removed.
Also, in the 15� curvature group, smear layer removal was significant,
but in the apical areas, smear layer removal was poor [25].
In the study of Jahan et al. smear layer removal was almost complete
in the Er, Cr: YSGG laser group, but in the control group
(5.25% NaOCl and 3% H2O2) the presence of the smear layer was
significant [26].
Anti-bacterial and anti-Candida albicans effects
Yasuda et al. divided 60 straight single root teeth (0-5�) and
curved canals (5-10�) in five groups of control (without treatment),
5.25% NaOCl, Nd: YAG laser (0.5 w and 50mJ -1 w and
100mJ) and Er: YAG laser (0.5 w and 50mJ - 1 w and 100mJ). The
canals were then infected with enterococcus faecalis. The rate of
colony reduction in the irrigant group in both direct and curved
canal was 100%. This rate was 75.8% and 73% (p> 0.05) respectively
in the Nd: YAG group (0.5 w and 50mJ), 88.2 and 84.5%
(p> 0.05) respectively in the Nd: YAG group (1 w and 100mJ),
86.6 and 76.1% (p <0.05) respectively in the Er: YAG group (0.5
w and 50mJ) and 94.6 and 86% (p<0.05) in the Er: YAG group
(1 w and 100mJ). Nd: YAG laser irradiation did not make a significant
difference between the direct and curved groups, but the
bactericidal effect of Er: YAG in the curved group was significantly
lower than the direct group. Although the results of Er:
YAG were slightly better than Nd: YAG, the difference between
them was not significant [27].
Ballout et al. divided 50 maxillary incisors infected with Enterococcus
faecalis into five groups: negative control, plasma jet, dielectric
barrier discharge, PDT (660 nm diode laser) and positive
control group (NaOCl and ultrasound stimulation). In the apical
and coronal regions, the colony count in the plasma and photodynamic
therapy groups were similar to the negative control
group and did not differ significantly. Also, photodynamic therapy
showed a less significant effect than the plasma jet group. Only
NaOCl had the best colony reduction and was able to reduce it to
some extent [32].
Sabino et al. investigated the fungicidal effect of PDT (660 nm
diode laser) using methylene blue in the canals with a curvature
of 15-25�. The canals were prepared with a rotary instrument
and then laser irradiation was done with two types of fibers (diffuser
and the common type) for 2 minutes for each canal. Evaluation
of Candida albicans colony reduction using luminescence
and digital camera imaging showed that irradiation with diffuser
fiber tip caused 3.5 log and in the laser group with the common
tip caused 2 log further reduction of Candida colony compared
to the control group. The diffuser tip was able to reach its maximum
ideal fungicidal effect in less than two minutes, while the
maximum laser effect with the conventional tip at the end of six
minutes of irradiation showed a relative fungicidal effect [30].
Moon et al. Evaluated the effect of irrigants activation with Nd:
YAG laser on Gutta-percha sealing. 63 molar teeth with canal curvature
of more than 20 degrees were selected and prepared by rotary
instrument and divided into four groups of 17% EDTA and
5.25% NaOCl with and without laser irradiation. The canals were
then closed with Gutta-percha and fluorescent sealer. At 2 and 5
mm sections from the apex, the 17% EDTA group without laser,
the 5.25% NaOCl group with laser, and the 17% EDTA group
with laser showed the highest sealer penetration into the tubules,
respectively. Also, laser-stimulated NaOCl showed a significantly
better penetration than NaOCl without laser radiation [28].
Gupta et al. evaluated the effect of Er: YAG and Nd: YAG laser
on irritant activation on improving sealer penetration in curved
canals. They used two newly introduced irritants, including Largal
Ultra and BioPure MTAD. 140 human molars were divided in
seven groups including BioPure MTAD (Er: YAG and Nd: YAG
and irigant), Largal Ultra (Er: YAG and Nd: YAG and irigant)
and negative control (without laser and without irigant). Canals
were prepared with a rotary instrument. After contact with irrigants
and laser irradiation, the canals were filled with fluorescently
labeled gutta-percha and examined by CLSM. Compared to the
negative control group, laser improved the sealer penetration into
dentin tubules and Er: YAG irradiation and the use of BioPure
MTAD had better results [33].
Abdelgawad investigated the effect of irritants activation by 980
nm diode laser irradiation on the gutta-percha compaction using
gutta-core or single-cone instrument. 24 molar teeth with a
canal curvature of more than 20 � were prepared by a rotary instrument.
The teeth were then divided into two groups of activation
of 15% EDTA and 2.5% NaOCl with and without laser
irradiation and each group was divided into two subgroups of s
gutta-core or single-cone. By preparing sections from 2, 4, 6, 8
and 12 mm from the apex, the percentage of gutta-percha filled
area (PGFA) and the percentage of sealer filled area (PSFA) were
evaluated using a stereomicroscope. Their findings showed that
irrigant activation had the highest amount of PGFA. Gutta-core
and the laser activation group significantly produced the highest
filling level and the lowest sealer consumption in 4-6-8 mm sections
compared to other sections [31].
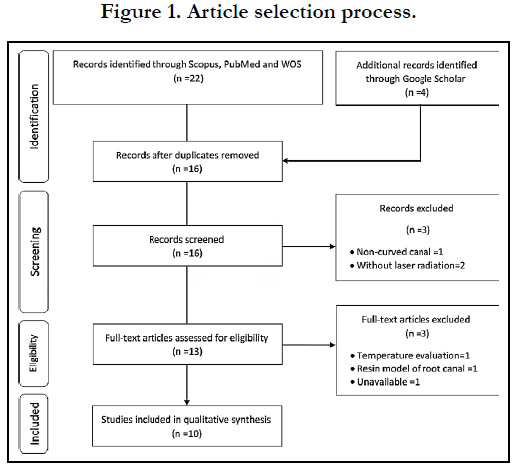
Figure 1. Article selection process.
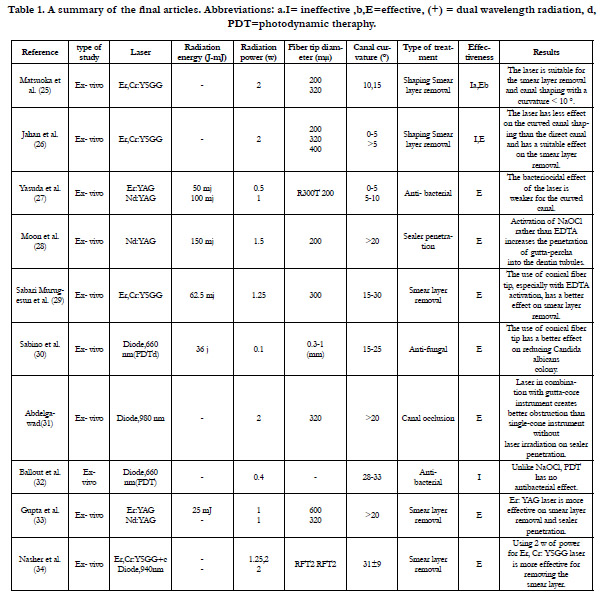

Table 1. Distribution of subjects according to gender.
Discussion
The results of ten reviewed studies showed that the irradiation
of Er: YAG, Nd: YAG Er, Cr: YSGG, and diode lasers in the
curved canals of human extracted teeth is effective generally for
the smear layer removal, antibacterial and antifungal ends, irritant
activation, filler compaction and sealer penetration into the dental
tubules, but it is not a suitable tool for the cutting and shaping of
the curved canals. Also, the efficacy of laser radiation in the above
studies was related to the severity of canal curvature, type of laser
and radiation setting, laser fiber tip and irrigants.
High power lasers, like erbium lasers, has an important role in
shaping straight canals and preparing the cavities by bone-cutting
[35, 36]. Laser irradiation in curved canals has limitations in
achieving the proper working length compared to hand or rotary
instruments because it requires a longer irradiation time and
increases the likelihood of technical errors such as wedge and
elbow formation, perforation, and laser fiber breakage [25, 26,
34]. The occurrence of laser technical errors in curved canals is
caused by reasons such as cumulative radiation dose, intensity of
canal curvature, the use of thicker fibers with less flexibility and
flat fiber tips compared to conical tips [25, 26]. In addition, the
laser fiber does not provide the proper signal to the dentist as
hand instruments, leading to hypo or hyper instrurmentation of
the canal. It seems that the formation of canals with a curvature
of more than 10 degrees by laser is not suitable, especially in the
apical areas [25, 26]. In these cases, the use of a rotary instrument
to form the canal is a more appropriate method, and the combination
of laser radiation with it to improve the smear layer removal,
increases its advantage [25, 35]. Air and water spray to reduce the
temperature of radiation due to the possibility of air and water
passing through the apical foramen and also damage to the apex
structure are other challenges of laser to shape a curved canal.
Therefore, radiation at a distance of 2-3 mm from the apical foramen
should be considered to reduce the incidence of subsequent
periapical problems due to laser [25].
In the reviewed studies, NaOCl, EDTA and H2O2 were used as
irrigants. The main role of an irritant is to remove debris and
microorganisms during endodontic treatment, which is caused by
chemical or mechanical effects. So far, various irrigants have been
introduced for endodontic treatment. These include acids, chelators
such as EDTA, and alkaline solutions such as NaOCl. EDTA
is more capable of harvesting inorganic matter in the smear layer
and debris than organic matter, and its combination with NAOCL,
which is more effective in harvesting the organic part of debris,
improves its performance [38]. However, the combination
of these two substances in the long run causes demineralization
of the dentin [39] and also reduces the active chlorine content of
NaOCl [40] The agitation of irigants for their better penetration
into the canal, especially the apical areas, improves the removal
of debris from the canal. Ultrasound and laser are effective tools
for agitating irrigants over syringe needle irrigation [41, 42]. In
the reviewed studies, the laser in the curved canals resulted in
smear layer removal alone [25, 26, 34] or through the agitation of the irrigants [25, 26, 29, 33]. The effect of laser activation of the
irrigants to remove the smear layer in curved canals seems to be
similar to that of laser radiation on direct canals as found in two
of the reviewed studies [25, 26], although its removal in the apical
areas is still limited [25, 26, 43, 44].
Proper root canal obstruction is one of the main goals of root
canal treatment. To this end, the main canal filler should have
a uniform density in the apical to coronal. A sealer also creates
a better seal by closing the remaining pores between the main
filler and the canal wall. Sealers also play an antimicrobial role by
penetrating dentin tubules in these areas but degenerate over time
[45]. Gutta-percha is the most common canal filler. In curved canals,
the density of the filler, especially in areas past the curvature
to the apical area, regardless of the filling technique, may not be
done properly [46, 47] and increase the likelihood of failure of
endodontic treatment [48]. In three reviewed studies, activation
of irrigants by Er: YAG, Nd: YAG, and 660 nm diode laser improved
root canal sealing using gutta-percha and sealer [28, 31,
33]. In a study by Moon et al. The best sealing was performed
by EDTA without Er: YAG laser and NaOCl produced a poorer
sealing without activation [28]. In the study of Gupta et al. Er:
YAG and Nd: YAG laser irradiation provided better penetration
for gutta-percha and sealer than for the control group [33]. Also,
in the Abdelgawad study, 660 nm diode laser radiation reduced
sealer consumption [31]. Better smear layer removal by creating
micro-bubbles from the evaporation of irrigants and opening of
the
tubules is one of the mechanisms involved in improving the canal
obstruction with laser. Also, microbubbles may potentially
facilitate filler movement to the apical area and its compaction
[31]. In the study of Yasuda et al. [27] the antibacterial effect of
Er: YAG laser decreased from 100% in the direct canal to about
85% in the curved canal and in the Nd: YAG laser group, the
effect decreased from 88.2 to 84.5%. [27]. In a study by Ballout
et al., unlike NaOCl, 660 nm diode laser irradiation in the form
of photodynamic therapy did not cause antibacterial effects [32].
Also, in the study of Sabino et al. 660 nm diode laser had anti-
Candida albicans effects [30]. As can be seen, the antimicrobial
effect of the laser depends on the wavelength, radiation setting
and microorganisms type, in a way that powers higher than 0.5 w
increase its effectiveness [27, 49]. In the study of Kasic et al. Er,
Cr: YSGG, Er: YAG and Nd: YAG, respectively, reduced enterococcus
faecalis in the direct canal by 100%, 100% and 62.1% [50].
The 660 nm diode laser appears to have moderate effects against
Enterococcus faecalis as the most common infectious pathogen
in the root canal compared to some diode laser wavelengths such
as 810 and 980 [49, 51].
One of the concerns of laser radiation during root canal treatment
is the increase in dentin temperature and the possibility of
damage to periodontal tissue. Increasing the temperature by water
and air spray when working on the root canal with Er, Cr: YSGG,
Er: YAG and Nd: YAG lasers as well as the diode laser is less
than 10� [24, 52-55] that appears dose not to cause thermal damage.
In addition, creating time intervals between laser radiations
can cause fluctuating changes in temperature and better thermal
control.
Finally, the results of this review study show that Er, Cr: YSGG,
Er: YAG and Nd: YAG and diodes lasers are suitable as an adjuant
instrument for smear layer removal, reduction of bacterial
and Candida albicans colony, infiltration and compaction of the
main filler and the sealer in curved canals. This depends on the
type of laser, radiation setting and canal curvature severity. Also,
canal shaping with Er, Cr: YSGG laser is associated with complications
such as hyper instrumentation and perforation and is not
suitable for curved canals > 10�. The use of fiber with a conical
tip and smaller diameter can be associated with better therapeutic
results in this type of canals.
References
-
[1]. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated
teeth can fail. Int Endod J. 2001 Jan;34(1):1-10. PubMed PMI
D: 11307374. [2]. Haupt F, Meinel M, Gunawardana A, H�lsmann M. Effectiveness of different activated irrigation techniques on debris and smear layer removal from curved root canals: a SEM evaluation. Aust Endod J. 2020 Apr;46(1):40-46. PubMed PMID: 30907051.
[3]. Kosti E, Zinelis S, Molyvdas I, Lambrianidis T. Effect of root canal curvature on the failure incidence of ProFile rotary Ni-Ti endodontic instruments. Int Endod J. 2011 Oct;44(10):917-25. PubMed PMID: 21658071.
[4]. Stadler LE, Wennberg A, Olgart L. Instrumentation of the curved root canal using filing or reaming technique--a clinical study of technical complications. Swed Dent J. 1986;10(1-2):37-43. PubMed PMID: 3458317.
[5]. Ansari I, Maria R. Managing curved canals. Contemp Clin Dent. 2012 Apr;3(2):237-41. PubMed PMID: 22919234.
[6]. Imura N, Pinheiro ET, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007 Nov;33(11):1278-82. PubMed PMID: 17963946.
[7]. Martins JNR, Marques D, Silva EJNL, Caram�s J, Mata A, Versiani MA. Prevalence of C-shaped canal morphology using cone beam computed tomography - a systematic review with meta-analysis. Int Endod J. 2019 Nov;52(11):1556-1572. PubMed PMID: 31215045.
[8]. Estrela C, Bueno MR, Barletta FB, Guedes OA, Porto OC, Estrela CR, P�cora JD. Identification of Apical and Cervical Curvature Radius of Human Molars. Braz Dent J. 2015 Jul-Aug;26(4):351-6. PubMed PMID: 26312971.
[9]. Roy A, Astekar M, Bansal R, Gurtu A, Kumar M, Agarwal LK. Racial predilection of C-shaped canal configuration in the mandibular second molar. J Conserv Dent. 2019 Mar-Apr;22(2):133-138. PubMed PMID: 31142981.
[10]. Boijink D, Costa DD, Hoppe CB, Kopper PMP, Grecca FS. Apically Extruded Debris in Curved Root Canals Using the WaveOne Gold Reciprocating and Twisted File Adaptive Systems. J Endod. 2018 Aug;44(8):1289- 1292. PubMed PMID: 29908692.
[11]. Zmener O, Pameijer CH, Alvarez Serrano S, Hernandez SR. Cleaning efficacy using two engine-driven systems versus manual instrumentation in curved root canals: a scanning electron microscopic study. J Endod. 2011 Sep;37(9):1279-82. PubMed PMID: 21846548.
[12]. Glossen CR, Haller RH, Dove SB, del Rio CE. A comparison of root canal preparations using Ni-Ti hand, Ni-Ti engine-driven, and K-Flex endodontic instruments. J Endod. 1995 Mar;21(3):146-51. PubMed PMID: 7561658.
[13]. Sonntag D, Delschen S, Stachniss V. Root-canal shaping with manual and rotary Ni-Ti files performed by students. Int Endod J. 2003 Nov;36(11):715- 23. PubMed PMID: 14641434.
[14]. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005 Oct;38(10):743-52. PubMed PMID: 16164689.
[15]. DiVito E, Peters OA, Olivi G. Effectiveness of the erbium:YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Lasers Med Sci. 2012 Mar;27(2):273-80. PubMed PMID: 21120568.
[16]. Samiei M, Pakdel SM, Rikhtegaran S, Shakoei S, Ebrahimpour D, Taghavi P. Scanning electron microscopy comparison of the cleaning efficacy of a root canal system by Nd:YAG laser and rotary instruments. Microsc Microanal. 2014 Aug;20(4):1240-5. PubMed PMID: 24887536.
[17]. Onay EO, Gogos C, Ungor M, Economides N, Lyssaris V, Ogus E, Lambrianidis T. Effect of Er,Cr:YSGG laser irradiation on apical sealing ability of calcium silicatecontaining endodontic materials in root-end cavities. Dent Mater J. 2014;33(4):570-5. PubMed PMID: 25087664.
[18]. Anagnostaki E, Mylona V, Parker S, Lynch E, Grootveld M. Systematic Review on the Role of Lasers in Endodontic Therapy: Valuable Adjunct Treatment? Dent J (Basel). 2020 Jul 1;8(3):63. PubMed PMID: 32630217. [19]. Mohammadi Z. Laser applications in endodontics: an update review. Int Dent J. 2009 Feb;59(1):35-46. PubMed PMID: 19323310.
[20]. Walia V, Goswami M, Mishra S, Walia N, Sahay D. Comparative Evaluation of the Efficacy of Chlorhexidine, Sodium Hypochlorite, the Diode Laser and Saline in Reducing the Microbial Count in Primary Teeth Root Canals - An In Vivo Study. J Lasers Med Sci. 2019 Fall;10(4):268-274. PubMed PMID: 31875118.
[21]. Meire MA, Coenye T, Nelis HJ, De Moor RJ. Evaluation of Nd:YAG and Er:YAG irradiation, antibacterial photodynamic therapy and sodium hypochlorite treatment on Enterococcus faecalis biofilms. Int Endod J. 2012 May;45(5):482-91. PubMed PMID: 22243483.
[22]. Deleu E, Meire MA, De Moor RJ. Efficacy of laser-based irrigant activation methods in removing debris from simulated root canal irregularities. Lasers Med Sci. 2015 Feb;30(2):831-5. PubMed PMID: 24091791.
[23]. Olivi G. Laser Use in Endodontics: Evolution from Direct Laser Irradiation to Laser- Activated Irrigation. J Laser Dent J Laser Dent. 2013;2121(22):58� 71.
[24]. Guidotti R, Merigo E, Fornaini C, Rocca JP, Medioni E, Vescovi P. Er:YAG 2,940-nm laser fiber in endodontic treatment: a help in removing smear layer. Lasers Med Sci. 2014 Jan;29(1):69-75. PubMed PMID: 23212445.
[25]. Matsuoka E, Jayawardena JA, Matsumoto K. Morphological study of the Er,Cr:YSGG laser for root canal preparation in mandibular incisors with curved root canals. Photomed Laser Surg. 2005 Oct;23(5):480-4. PubMed PMID: 16262578.
[26]. Jahan KM, Hossain M, Nakamura Y, Yoshishige Y, Kinoshita J, Matsumoto K. An assessment following root canal preparation by Er,Cr: YSGG laser irradiation in straight and curved roots, in vitro. Lasers Med Sci. 2006 Dec;21(4):229-34. PubMed PMID: 17072516.
[27]. Yasuda Y, Kawamorita T, Yamaguchi H, Saito T. Bactericidal effect of Nd:YAG and Er:YAG lasers in experimentally infected curved root canals. Photomed Laser Surg. 2010 Oct;28 Suppl 2:S75-8. PubMed PMID: 20738170.
[28]. Moon YM, Kim HC, Bae KS, Baek SH, Shon WJ, Lee W. Effect of laseractivated irrigation of 1320-nanometer Nd:YAG laser on sealer penetration in curved root canals. J Endod. 2012 Apr;38(4):531-5. PubMed PMID: 22414844.
[29]. Murugesan MS, Rajasekaran M, Indra R, Suganthan P. Efficacy of Er , Cr : YSGG Laser with Conical Tip Design in Smear Layer Removal at the Apical Third of Curved Root Canals. 2013;3(August):55�9.
[30]. Sabino CP, Garcez AS, N��ez SC, Ribeiro MS, Hamblin MR. Real-time evaluation of two light delivery systems for photodynamic disinfection of Candida albicans biofilm in curved root canals. Lasers Med Sci. 2015 Aug;30(6):1657-65. PubMed PMID: 25060900.
[31]. Abdelgawad L. QUALITY OF SINGLE CONE AND GUTTA CORE OBTURATION IN CURVED ROOT CANALS AFTER NEEDLE OR DIODE LASER IRRIGANT ACTIVATION USING CONE BEAM COMPUTED TOMOGRAPHY AND STEREOMICROSCOPE. Egypt Dent J. 2016;62(1):1211�20.
[32]. Ballout H, Hertel M, Doehring J, Kostka E, Hartwig S, Paris S, Preissner S. Effects of plasma jet, dielectric barrier discharge, photodynamic therapy and sodium hypochlorite on infected curved root canals. J Biophotonics. 2018 Mar;11(3). PubMed PMID: 29024574.
[33]. Gupta R, Wadhwani KK, Tikku AP, Chandra A. Effect of laser-activated irrigation on smear layer removal and sealer penetration: An in vitro study. J Conserv Dent. 2020 Sep-Oct;23(5):451-456. PubMed PMID: 33911352.
[34]. Nasher R, Hilgers RD, Gutknecht N. Debris and Smear Layer Removal in Curved Root Canals Using the Dual Wavelength Er,Cr:YSGG/Diode 940 nm Laser and the XP-Endoshaper and Finisher Technique. Photobiomodul Photomed Laser Surg. 2020 Mar;38(3):174-180. PubMed PMID: 31968180.
[35]. Kokuzawa C, Ebihara A, Watanabe S, Anjo T, Bolortuya G, Saegusa H, Suda H. Shaping of the root canal using Er:YAG laser irradiation. Photomed Laser Surg. 2012 Jul;30(7):367-73. PubMed PMID: 22690799.
[36]. Moogi PP, Rao RN. Cleaning and shaping the root canal with an Nd: YAG laser beam: A comparative study. J Conserv Dent. 2010 Apr;13(2):84-8. PubMed PMID: 20859481.
[37]. Becker TD, Woollard GW. Endodontic irrigation. Vol. 49, General dentistry. 2001. p. 272�6.
[38]. Johal S, Baumgartner JC, Marshall JG. Comparison of the antimicrobial efficacy of 1.3% NaOCl/BioPure MTAD to 5.25% NaOCl/15% EDTA for root canal irrigation. J Endod. 2007 Jan;33(1):48-51. PubMed PMID: 17185130.
[39]. Ozdemir HO, Buzoglu HD, Calt S, Cehreli ZC, Varol E, Temel A. Chemical and ultramorphologic effects of ethylenediaminetetraacetic acid and sodium hypochlorite in young and old root canal dentin. J Endod. 2012 Feb;38(2):204-8. PubMed PMID: 22244637.
[40]. Rossi-Fedele G, Dogramaci EJ, Guastalli AR, Steier L, de Figueiredo JA. Antagonistic interactions between sodium hypochlorite, chlorhexidine, EDTA, and citric acid. J Endod. 2012 Apr;38(4):426-31. PubMed PMID: 22414823.
[41]. Rodrigues CT, Duarte MAH, Guimar�es BM, Vivan RR, Bernardineli N. Comparison of two methods of irrigant agitation in the removal of residual filling material in retreatment. Braz Oral Res. 2017 Dec 18;31:e113. Pub- Med PMID: 29267674.
[42]. Gu LS, Kim JR, Ling J, Choi KK, Pashley DH, Tay FR. Review of contemporary irrigant agitation techniques and devices. J Endod. 2009 Jun;35(6):791-804. PubMed PMID: 19482174.
[43]. da Costa Lima GA, Aguiar CM, C�mara AC, Alves LC, Dos Santos FA, do Nascimento AE. Comparison of smear layer removal using the Nd:YAG laser, ultrasound, ProTaper Universal system, and CanalBrush methods: an in vitro study. J Endod. 2015 Mar;41(3):400-4. PubMed PMID: 25600669.
[44]. Akyuz Ekim SN, Erdemir A. Comparison of different irrigation activation techniques on smear layer removal: an in vitro study. Microsc Res Tech. 2015 Mar;78(3):230-9. PubMed PMID: 25582378.
[45]. Komabayashi T, Colmenar D, Cvach N, Bhat A, Primus C, Imai Y. Comprehensive review of current endodontic sealers. Dent Mater J. 2020 Sep 29;39(5):703-720. PubMed PMID: 32213767.
[46]. Kersten HW, Fransman R, Thoden van Velzen SK. Thermomechanical compaction of gutta-percha. II. A comparison with lateral condensation in curved root canals. Int Endod J. 1986 May;19(3):134-40. PubMed PMID: 3460968.
[47]. Sobhi MB, Khan I. Penetration depth of nickel titanium and stainless steel finger spreaders in curved root canals. J Coll Physicians Surg Pak. 2003 Feb;13(2):70-2. PubMed PMID: 12685945.
[48]. Wu MK, Kast'�kov� A, Wesselink PR. Quality of cold and warm guttapercha fillings in oval canals in mandibular premolars. Int Endod J. 2001 Sep;34(6):485-91. PubMed PMID: 11556517.
[49]. Gutknecht N, Franzen R, Schippers M, Lampert F. Bactericidal effect of a 980-nm diode laser in the root canal wall dentin of bovine teeth. J Clin Laser Med Surg. 2004 Feb;22(1):9-13. PubMed PMID: 15117481.
[50]. Kasic S, Knezovic M, Beader N, Gabric D, Malcic AI, Baraba A. Efficacy of Three Different Lasers on Eradication of Enterococcus faecalis and Candida albicans Biofilms in Root Canal System. Photomed Laser Surg. 2017 Jul;35(7):372-377. PubMed PMID: 28426292.
[51]. Sarda RA, Shetty RM, Tamrakar A, Shetty SY. Antimicrobial efficacy of photodynamic therapy, diode laser, and sodium hypochlorite and their combinations on endodontic pathogens. Photodiagnosis Photodyn Ther. 2019 Dec;28:265-272. PubMed PMID: 31585175.
[52]. Kimura Y, Yonaga K, Yokoyama K, Kinoshita J, Ogata Y, Matsumoto K. Root surface temperature increase during Er:YAG laser irradiation of root canals. J Endod. 2002 Feb;28(2):76-8. PubMed PMID: 11833692.
[53]. Kobayashi K, Yamazaki Y, Tomita T, Tsuchida M, Ozawa T, Kohno A, et al. Temperature elevation on root surfaces during Nd:YAG laser irradiation in root canals. Int Congr Ser. 2003;1248(C):287�92.
[54]. da Costa Ribeiro A, Nogueira GE, Antoniazzi JH, Moritz A, Zezell DM. Effects of diode laser (810 nm) irradiation on root canal walls: thermographic and morphological studies. J Endod. 2007 Mar;33(3):252-5. Pub- Med PMID: 17320707.
[55]. Al-Zand S, Al-Maliky M, Mahmood A, Al-Karadaghy T. Temperature elevation investigations on the external root surface during irradiation with 940 nm diode laser in root canal treatment. Saudi Endod J. 2018;8(1):14�8.





