Comparing The Effect Of Primary Enamel Deproteinization Before And After Acid Etching On The Shear Bond Strength - An In-Vitro Study
Ola Abd El-Geleel*
Lecturer, Pediatric Dentistry and Dental Public Health Department, Ain-Shams University, Cairo, Egypt.
*Corresponding Author
Ola Abd El-Geleel,
Lecturer, Pediatric Dentistry and Dental Public Health Department, Ain-Shams University, Cairo, Egypt.
Tel: 202 01006086830
E-mail: ola@dent.asu.edu.eg/olapd@asfd.asu.edu.eg
Received: September 30, 2021; Accepted: October 29, 2021; Published: November 08, 2021
Citation: Ola Abd El-Geleel. Comparing The Effect Of Primary Enamel Deproteinization Before And After Acid Etching On The Shear Bond Strength - An In-vitro Study. Int J Dentistry Oral Sci. 2021;8(10):4912-4916. doi: dx.doi.org/10.19070/2377-8075-21000993
Copyright: Ola Abd El-Geleel�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: The purpose of this in vitro investigation was to assess the effect of deproteinization before and after acid etching
on the shear bond strength when primary enamel is bonded to composite resin.
Materials and Methods: Forty-five enamel specimens were randomly distributed into 3 groups (15 each) according to the
surface treatment, in Group I: enamel is acid etched only, in Group II: specimens are acid etched then exposed to 1 minute
NaOCl deproteinizationin, and in Group III enamel specimens were deproteinized then acid etched. An adhesive was applied
(Adper Single Bond universal) was applied, nanohybrid composite (Z350) was placed using Tygon catheter. All the samples
were then subjected to the SBS test using a universal testing machine. Data analysis was performed using a one-way ANOVA
test followed by the Tukey test. P-values less than 0.05 were considered significant.
Results: Comparison of the mean SBS between the groups showed a statistically significant difference between all groups,
Group II displayed the highest mean value followed by Group III, while Group I where enamel was only etched with phosphoric
acid showed the least mean value.
Conclusions: Deproteinizing the enamel of primary teeth with NaOCl before or after acid etching showed a significant
increasein the SBS compared to the application of acid etch alone, moreover, deproteinization after acid etching yielded the
highest SBS values.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Shear Bond Strength; Primary Enamel; Deproteinization; Sodium Hypochlorite.
Introduction
In order to achieve adequate bonding to enamel, appropriate
preparation of the surface is required, which involves removing
the outer pellicle and surface roughening, in a process called conditioning.
Acid etching with phosphoric acid is one of the conditioning
techniques that uses acid gel to create micro-porosities on
the surface, that can render it more receptive to resin penetration
and thus better adhesion through micromechanical interlocking
[1].
The advancement of enamel pretreatment with orthophosphoric
acid by Buonocore in 1955 [2] is a benchmark in adhesive and
cosmetic dentistry. The breakthrough concerned enhancing the
adhesion of acrylic resins to enamelset the stage for abundant research
work to reach to a better understanding and improvements
in the quality of adhesive bonds to the tooth structure through
endeavors involving various materials and techniques.
The success of adhesive restorative materials and their long-term
clinical performance is challenged by the continuous exposure to
conditions that may affect their bond strength; as these materials
have to withstand high mechanical forces during masticationand
hence, a strong bond to the tooth structure is required [3].
It has been established that factors influencing bonding to enamel
include the type of etching agent, duration of etching, concentration
of acid being used, composition of the enamel surface and
removal of organic material [4]. And hence, higher amount of
protein content reported in defective enamel structureshas been
recognized by earlier studies to adversely affect the quality of the
bond [5, 6].
Given the structural differences between primary and permanent enamel regards the less mineral content, the presence of a thicker
outer layer of less organized primeless enamel and for most, the
higher amount of organic content. All these features compromise
the etching capacity, bonding mechanism, and bond efficacy of
the resinous material to primary enamel [7].
Enamel deproteinization has been proposed as a non-invasive
technique that aim to achieve a clinically successful etching pattern
and improve the bond strength through effectively removing
the organic content from the enamel surface [8-10].
Sodium hypochlorite (NaOCl) is recognized as potent protein denaturant,
it has been used efficiently to eliminate organic material
from the root canal spaces, and consequently it was thought of as
a possible maneuver to optimize adhesion to the tooth structure
through ridding enamel from the organic elements investing the
outer layer the enamel structure and the acquired pellicle [8].
The pioneer attempt by Espinosa et al. back in 2008 [8], showed
that enamel pretreatment with 5.25% NaOCl for 60 seconds before
acid etching significantly improves both the quantity and
the quality of the etching namely duplicating the area of etched
enamel in addition to significantly increasing the proportion of
type I and II etching patterns that have greater retentive capacities
compared to type III. Thus, this modality was dubbed with
high potential to optimize adhesion and improve bond strengths.
The same researchers further affirmed their results with a following
study two years later using resin replica models showing a
high proportion of resin tag penetration equivalent to type I and
II etching in the samples that were subjected to deproteinization
prior to etching on larger areas of the etched enamel specimens
[12]. Moreover,adhesive resinshowed a significant penetrationin
artificial enamel carious lesions specimens evaluated by G�mez
et al.,when the conventional technique was complemented with
NaOCl deproteinization [12].
Although there is almost a unanimity that deproteinization improves
the quality of the bond of the tooth substrates to resin,
however, there is not a consensus regardingapplying the agent before
or after acid etching,as other researchers further substantiate
that deproteinization granted better results when conducted on
acid etched enamel specimens with relatively high protein content
as those of primary and immature permanent teeth [13-15].
Taking in consideration the uncertain sequence of application and
the paucity in literature investigating the bond strength of composites
bonded to deproteinized primary enamel rather than exploring
only the topographic changes, this study�smain objectives
is to test the null hypothesis that there is no difference concerning
the effect of primary enamel deproteinization before or after acid
etching on composite resin shear bond strength in addition to
validating the effect of that extra step on the bonding outcome.
Materials and Methods
This study is an experimental in-vitro study, comparing the shear
bond strength values of three groups of primary enamel specimens
bonded to composite resin where the specimens are subjected
to different conditioning methods prior to bonding.
Forty five (N=45) sound primary molars that were extracted due
to looseness caused by physiologic root resorption from patients
visiting the outpatient clinic of the Pediatric Dentistry and Dental
Public Health Department, Ain-Shams University, Cairo, Egypt,
were included in the study. The teeth with intact coronal portion
only were used in the study while those with enamel cracks or
fractures along the buccal aspect, malformations, carious lesions,
restorations or erosions were excluded.Teeth were washed under
running water and cleaned from any debris and attached soft tissue,
and immersed in saline solution which was daily renewed until
being tested [16].
Each tooth was cut 2mm below cement-enamel junction and sectioned
mesiodistally into two halves under copious air-water coolant
spray using a diamond disc mounted on a low speed straight
hand piece,the sectioned buccal surfaces were totally embedded
in chemical cured acrylic resin placed in polyvinyl ring such that
the dentin side was embedded within the acrylic and the buccal
enamel surfaces were exposed for bonding in order to allow for
standardized and secured placement during SBS testing and later
the specimens. [17].
A 320 grit Sand paper was used for flattening & a 400 and 600
grit sand paper were used for smoothening of the enamel surfaceunder
water coolant in order to obtain a smooth flat surface. The
specimens were cleaned with running water and ultrasonic cleaner
to ensure absence of any debris [15].
The enamel specimens were assigned numbers then randomly allocated
in the following groups as follows:
Group I: (control) The enamel surface was etched with 37%
H3PO4 , applied for 15 s with a microbrush, washed with sterile
water for 20 s, and then dried with compressed air for 15 s [15].
Group II: (acid etching followed by deproteinization)the samples
were etched as in group I, after achieving dryness, the surfaces
were treated with 5.25% NaOCl (Clorox�) applied with a sterile
cotton swab for 60 s, washed with sterile water, then dried for 10
s [16].
Group III: (deproteinization followed with 5.25% NaOCl)5.25%
NaOCl was applied with a sterile cotton swab for 60 s, washed
with sterile water, then dried for 10 s, then the samples are etched
as in group I.
Later, all the conditioned enamel surfaces were bonded to composite
as follows, A disposable micro brush was used to apply the
adhesive on the tooth structure for 20 seconds, followed by gentle
air drying for 5 seconds till complete evaporation of the solvent
which was assessed by the absence of motion of the adhesive layer
on the tooth upon application of air then it was light cured for
20 seconds with Elipar� light cure with a light intensity of 1200
Mw/cm2 .Rubber Tygon catheterof 2 mm internal diameter and
2 mm height was placed on the etched enamel surface to act as a
mould for building composite buttons on enamel surfaces. The
catheters were cut off using a sharp lancet, and the specimens
were stored in normal saline at 37�C for 24 hours before testing
[17]. The SBS was done using universal testing machine with
constant cross head speed of 1 mm/min using a chisel driving
the load onto the specimen at the enamel- composite interface till
debonding. Shear bond strength values were recorded as Newton
(N) initially and then they were calculated as megapascals (MPa).
Results
Statistical analysis was performed with IBM� SPSS� Statistics
Version 20 for Windows. Data normality was checked using Kolgomorv-
Smirnov test and Shapiro-Wilk test. One-way ANOVA
was used for comparison between groups followed by Tukey post
hoc test. p values less than 0.05 were considered significant.
Comparing the mean SBSs among the study groups showed that
the highest mean value was obtained in Group II, followed by
Group III, while the least value was obtained in Group I.
One-way ANOVA test performed to compare the mean shear
bond strength values among the study groupsshowed significant
difference between studied groups and Tukey post hock test
showed statistical difference between all pairs.
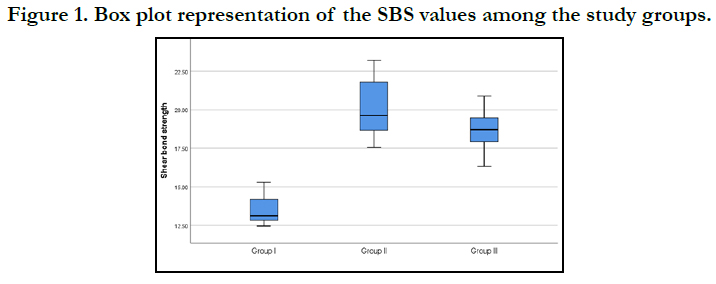

Figure 1. Box plot representation of the SBS values among the study groups.


Table 1. Comparison of clinical parameters and hydroxyproline between groups.
Discussion
The increased preference for composites application among clinicians
is credited to the conservative tooth preparation, good
physical properties, esthetics and also their adhesive capability to
tooth tissues [18]. A satisfactory bond strength between the tooth
structure and the restorative material is crucial for the clinical success
of the restoration, otherwise failure in form of recurrent caries,
tooth sensitivity, and defective restorations might result from
stresses created at the interface by resin contraction forces [19].
During its development, enamel is initially composed of a protein
rich matrix, and as enamel matures, the protein matrix is degraded,
and the preliminary hydroxyapatite crystals act as growth centers
around which minerals are deposited during enamel maturation.
In primary teeth however, the outermost enamel surface exhibits
an excess of protein content in addition to a layer of disorganized
aprismatic enamel which in turn negatively affect the etching
procedure and hence the bond strength [20]. Phosphoric acid etch
can demineralize the inorganic components of enamel, nevertheless
it does not eliminate the organic matter on the enamel surface
and from this point, deproteinizing agents came in interplay to
augment the bond strength to enamel surface [21].
In this study, shear bond strength test (SBS) was chosen to assess
the bond strength of composite resin to the preconditioned
enamel surfaces. This test is very popular because of its relative
simplicity as specimens do not need further processing following
bonding, moreover specimens in other testsare difficult to be
aligned in the testing machine without creating deleterious stresses.
Furthermore, a good correlation coefficient is documented
between annual failure rates of composite restoration and shear
bond strength [22, 23].
Although there is a multitude of studies investigating the effect of
different deproteinizing agents incorporated in the enamel conditioning
protocol prior to bonding, yet the results of which are
inconclusive and sometimes contradictory, which questions the
validity of adding another step to the already technique sensitive
procedure, furthermore, incorporating such step whether before
or after acid etching resulted in perplexing outcomes, that even
makes the sequence of application not a clear cut regimen.
The results of the current study showed that sodium hypochlorite
enamel conditioning for one minute prior to bonding significantly
improves the bond strength of composite to primary
enamel, whether this step was conducted prior to acid etching or
following it.This was found to go in harmony with the results of
Aras et al.[13], as the authors also concluded from their research
conducted on 3 different enamel types, that the deproteinization
of both primary and immature permanent enamel improved the
shear bond strength values to composite resin more than permanent
enamel,the later only showed in substantial improvement
with deproteinization. Their results could be explained through
assuming that the effect of NaOCl is only detectible ifapplied on
substrates higher in protein content.
And hence when this protein has been eliminated, the resultant
enamel surface would display detectable bond enhancement,
which is the case in primary and immature permanent enamels
compared to the permanent enamel which has comparatively
lower protein content.
Furthermore, a later study [14] on immature permanent enamel
also found a favorable outcome of deproteinization regardless
the sequence of application which was demonstrated as increased surface roughness of the pretreated enamel, even with lower concentration
of NaOCl (2.5% applied for one minute before or after
acid etching) and on top off all, the researcher utilized nonpolished
and uncut enamel specimens which presumably retain
thicker prismless enamel layer and organic pellicleat the surface,
yet the results still validated the process of deproteinization to
enhance the topographic features of enamel and make it more
receptive to composite bonding.
On contrary, the results of Ahuja et al. [10] and Harleen et al.
showed that enamel deproteinization before acid etching did
not favor a stronger interface between the substrate and composite
resin compared to specimens that are etched only, these
two studies depicted no significant change in the etching patterns
observed by scanning electron microscopy or the shear bond
strength values respectively. It is worth mentioning here that the
aforementioned researches utilized permanent enamel specimens
which inherently display less organic content and maybe more
abraded surfaces with less thickness of the aprismatic enamel
layer, these two factors could have rendered deproteinization as a
step withleast value in the bonding procedure.
Although, the contamination of the etched enamel surface can
jeopardize the bond between the conditioned enamel and compositeresin.
The highest shear bond strength values in this research
were obtained in group II in which NaOCl deproteinization
was appliedon etched enamel surface just before bonding, in
addition, these values were significantly higher than in the acid
etch group (control) and group III in which deproteinization was
intiated before acid etching. Therefore, it is evident that after acid
etching there might be a better chance for NaOCl to work on the
organic content and eliminate it from the etched surfaces, rather
than acting before hand on unetched surfaces with higher inorganic
content.
Regarding comparing the effect of different sequences of application
of the deproteinizing agent whether before or after acid
etching, Aras et al. [13] reached to the conclusion that NaOCl
deproteinization following acid etching conceded the highest SBS
values in primary enamel and immature permanent teeth specimens,
compared to the reversed sequence (NaOCl/ acid etch).
The authors further promoted this technique claiming that the
SBS values of immature permanent enamel specimens treated
with this exact sequence, approached those of permanent enamel
that were only acid etched. This inference would encourage clinicians
to advocate such protocol of enamel pretreatment specially
in immature permanent teeth which are known for their porous,
less mineralized and high in organic content enamel surfaces.
Later, Hasija et al. [15] demonstrated comparable results related to
the improvement in the bond strength to primary enamel adopting
the same sequence of application(acid etching/deproteinization
sequence). The researchers however tested the effect of
other deproteinizing agents (papain and bromelain proteolytic enzymes)
in addition to the NaOCl, and all the study groups showed
an enhancement in the mean values of SBS compared to the control
group in which no deproteinization was done. That is why the
authors advocated deproteinization after acid etching to achieve
better clinical outcomes though they did not investigate the effect
of applying the deproteinizing agent before etching.
Although deproteinization adds an additional step in the already
technique sensitive procedure of applying composite
restorations,which in turn increases the chair side time that could
be problematic in young patients, yet the benefit of significantly
enhancing the bond to primary enamel could encourage practitioners
to incorporate this procedure routinely when considering
primary enamel conditioning.
Conclusions
Considering the results of the current research the following conclusions
could be withdrawn.
� NaOCl deproteinization could be considered as a complementing
step to enhance the mechanical outcome of primary enamel
conditioning prior to bonding to composite resin.
� The shear bond strength values significantly increases when deproteinization
was preformed after acid etching compared to before
acid etching or when no deproteinization was done.
References
-
[1]. Canay S, Kocadereli I, Akca E. The effect of enamel air abrasion on the retention
of bonded metallic orthodontic brackets. Am J Orthod Dentofacial
Orthop. 2000; 117: 15�19. Pubmed PMID:10629515.
[2]. Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J DentRes 1955; 34: 849�853. Pubmed PMID:13271655.
[3]. Vasei F. Effect of chitosan treatment on shear bond strength of composite to deep dentin using self-etch and total-etch adhesive systems. Brazilian Dental Science. 2021;24(2).
[4]. Van Meerbeek B, Inouse S, Perdiago J, Lambrechts P, Vanherle G. Enamel and dentin adhesion. Fundamentals of Operative Dentistry. A Contemporary Approach. Chicago: Quintessence, 178-235, 2001.
[5]. Saroglu I, Aras S, Oztas D. Effect of deproteinization on composite bond strength in hypocalcified amelogenesis imperfecta. Oral Diseases 2006;12 (3): 305-308.
[6]. Aras S�, Ku�c�u�kes�men C�, Ku�c�u�kes�men HC. Influences of dental fluorosis and deproteinization treatment on shear bond strengths of composite restorations in permanent molar teeth. Fluoride2007; 40(4): 290-291.
[7]. Atkins CO Jr, Rubenstein L, Avent M. Preliminary clinical evaluation of dentinal and enamel bonding in primary anterior teeth. J Pedod 1986; 10: 239�246.
[8]. Espinosa R, Valencia R, Uribe M, Ceja I, Saadia M. Enamel deproteinization and itseffect on acid etching: An in vitro study. J Clin Pediatr Dent 2008;33:13-9.
[9]. Venezie RD, Vadiakas G, Christensen JR, Wright JT. Enamel pretreatment with sodium hypochlorite to enhance bonding in hypocalcified amelogenesis imperfecta: Case report and SEM analysis. Pediatr Dent 1994;16: 433-436.
[10]. Ahuja B, Yeluri R, Baliga S, Munshi AK. Enamel deproteinization before acid etching � A scanning electron microscopic observation. J Clin Pediatr Dent 2010;35:169-72.
[11]. Espinosa R, Valencia R, Uribe M, Ceja I, Cruz J, Saadia M, et al. Resin replica in enamel deproteinization and its effect on acid etching. J Clin Pediatr Dent 2010;35:47-51.
[12]. Go�mez S, Bravo P, Morales R, Romero A, Oyarzu�n A. Resin penetration in artificial enamel carious lesions after using sodium hypochlorite as a deproteinization agent. JClin Pediatr Dent 2014;39:51-6.
[13]. Aras S, Ku�c�u�kes�men C, Ku�c�u�kes�men HC, So�nmez IS. Deproteinization treatment on bond strengths of primary, mature and immature permanent tooth enamel. J Clin Pediatr Dent. 2013;37:275-9.
[14]. Abdelmegid FY. Effect of deproteinization before and after acid etching on the surface roughness of immature permanent enamel. Niger J Clin Pract. 2018 May;21(5):591-596. Pubmed PMID: 29735859.
[15]. Hasija P, Sachdev V, Mathur S, Rath R. Deproteinizing Agents as an Effective Enamel Bond Enhancer-An in Vitro Study. J Clin Pediatr Dent. 2017;41(4):280-283. PubmedPMID: 28650791.
[16]. L�pez-Luj�n NA, Munayco-Pantoja ER, Torres-Ramos G, Blanco-Victorio DJ, Siccha-Macassi A, L�pez-Ramos RP. Deproteinization of prim1/ary enamel with sodium hypochlorite before phosphoric acid etching. Desproteinizaci�n del esmalte primario con hipoclorito de sodio antes del grabado con �cido fosf�rico. Acta Odontol Latinoam. 2019;32(1):29-35.
[17]. Bahrololoomi Z, Kabudan M, Gholami L. Effect of Er:YAG Laser on Shear Bond Strength of Composite to Enamel and Dentin of Primary Teeth. J Dent (Tehran).2015;12(3):163-170. Pubmed PMID:26622267.
[18]. Heyman HO, Ritter AV, Roberson TM. Introduction to composite restorations. In: Roberson TM, Heyman HO, SwiftE. Sturdevant's Art and Science of operative dentistry. St.Louis: Mosby Elsevier, 6: 216-228, 2013.Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent 2003;28: 215-235. Pubmed PMID:12760693.
[19]. Kodaka T, Kuroiwa M, Higashi S. Structural and distribution patterns of surface Prismless enamel in human permanent teeth. Caries Res 1991;25 (1): 7-20. Pubmed PMID: 2070383.
[20]. Ramakrishna Y, Bhoomika A, Harleen N, Munshi AK. Enamel deproteinization after acid etching-Is it worth the effort?. Dentistry. 2014;4(2):1-6.
[21]. Sirisha K, Rambabu T, Shankar YR, Ravikumar P. Validity of bond strength tests: A critical review: Part I. J Conserv Dent. 2014;17(4):305-311.
[22]. Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A, et al. Relationship between bond-strength tests and clinical outcomes. Dent Mater. 2010;26:e100�21. Pubmed PMID: 20006379.
[23]. Harleen N, Ramakrishna Y, Munshi AK. Enamel deproteinization before acid etching and its effect on the shear bond strength � An in vitro study. J Clin Pediatr Dent. 2011;36:19-23. Pubmed PMID:22900439.





