Reliability of SAR Angle in Assessing Anteroposterior Apical Base Discrepancy in Different Growth Patterns
Subashree Rathi Selvan1*, Dr. Arvind Sivakumar2, Balavenkata Bharathi Chaturvedula3
1 Department of Orthodontics and Dentofacial Orthopaedics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences(SIMATS),
Chennai, India.
2 Reader, Department of Orthodontics and Dentofacial Orthopaedics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences
(SIMATS), Chennai, India.
3 Department of Orthodontics and Dentofacial Orthopaedics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences (SIMATS),
Chennai, India.
*Corresponding Author
Subashree Rathi Selvan,
Department of Orthodontics and Dentofacial Orthopaedics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences(SIMATS),
Chennai, India.
Tel: +91 9384454146
E-mail: subashree.rathi@gmail.com
Received: September 18, 2021; Accepted: November 13, 2021; Published: November 23, 2021
Citation: Subashree Rathi Selvan, Dr. Arvind Sivakumar, Balavenkata Bharathi Chaturvedula. Reliability of SAR Angle in Assessing Anteroposterior Apical Base Discrepancy in Different Growth Patterns. Int J Dentistry Oral Sci. 2021;8(11):5113-5116. doi: dx.doi.org/10.19070/2377-8075-210001029
Copyright: Subashree Rathi Selvan�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim and Objective: The aim of this study was to compare and verify the accuracy of SAR angle in predicting sagittal jaw
discrepancy among subjects with different growth pattern.
Materials and Method: The study material includes lateral cephalometric radiographs of ninety individuals with thirty in
each group. It was further divided into three subgroups as hypodivergent, normodivergent and hyperdivergent with 10 samples
per group. The SAR angle was measured as given by the author using FACAD. The values of SAR angle obtained for each
subgroup was subjected for statistical evaluation.
Results: The mean of groups 1, 2 and 3 were 55.98�2.24, 50.18�2.70 and 63.65�2.25 respectively. Oneway ANOVA shows a
statistically significant difference between horizontal and vertical growth patterns in skeletal class III cases with a significance
value of 0.013 (P<0.05).
Conclusion: Within the limitations of the study, it is concluded that SAR angle can be used as a reliable alternative measurement
to determine the discrepancy in apical jaw bases.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
SAR Angle; Anteroposterior Jaw Relation; Apical Jaw Base Discrepancy
Introduction
Assessment of jaw relationship in all three planes (anteroposterior,
transverse, and vertical) forms an integral part of orthodontic
diagnosis treatment planning. Orthodontic diagnosis became
more reliable with the use of cepahlometrics along with proper
history taking, models and photographs [1, 2]. There are several
analyses used to assess the anteroposterior discrepancy with numerous
angular and linear measurements [3-13]. Few of the most
commonly used analyses are the ANB angle,Wits appraisaland
Beta angle. However, the validity of each of these parameters was
questionable because of the variability of landmarks with jaw rotation,
head posture, orthodontic treatment as well as growth.
Several studies have shown that the ANB angle is not reliable
because of the Nasion point, which is not fixed during growth
that affects the ANB angle. Rotation of the jaws due to growth
or orthodontic treatment also change ANB angle. The length of
cranial base, anterior facial height also affects ANB angle. ANB
angle decreases due to counter clockwise rotation of the mandible
with advancing age [14].
Wits appraisal overcomes the shortcomings of ANB angle. Perpendiculars
from Point A and B on the maxilla and mandible were
used in this analysis by Jacobson. Wits appraisal uses occlusal
plane, which is a dental parameter to describe skeletal jaw discrepancies.
Occlusal plane can be easily affected by tooth eruption or
by orthodontic tooth movement [15, 16]. Accurate identification
of occlusal plane is not easy or accurately reproducible [17, 18].
Beta angle, derived by Baik and Ververidou in 2004, assessed the
true apical base relationship independent of cranial reference
plane or occlusal plane. Although it gave a reliable picture of the
sagittal discrepancy, it used points A and B which were unstable
landmarks as they were subject to alveolar bone remodeling with
the change in position of incisors. Also, identification of the Condylion
point was not easily reproducible in cephalometric radiographs
[19]. Furthermore, in a study by shobha et al, in 2019, it
was found that Beta angle may not be a valid tool for assessment
sagittal jaw discrepancies in patients exhibiting vertical growth
patterns in skeletal class I and class II malocclusions [20].
The SAR angle is a new parameter for assessing the sagittal apical
base discrepancy. It was put forth by Sonahita Agarwal in the year
2014. It uses the three skeletal reference points: Point M, Point
G and Point W [21]. The mean SAR angle was 53 to 59 degree
for skeletal class I, <53degree for skeletal class II and >59 degree
for skeletal class III. The SAR angle is not inflenced by growth,
jaw rotations, orthodontic treatment or any other factor previously
associatedwith other angles. The Walkers point was found
to be stableafter the age of five.Hence, the aim of this study was
to compare and verify the accuracy of SAR angle in predicting
sagittal jaw discrepancy among subjects with hyperdivergent, hypodivergent
and normodivergent growth patterns in skeletal class
I, class II and class III malocclusions.
Materials And Methods
The total sample size was set as 90 with a power of 95% and alpha
error of 0.05. This study consisted of three groups with sample
size of 30 each based on skeletal malocclusions. It was further
divided into three subgroups as hypodivergent, normodivergent
and hyperdivergent with 10 samples per group. The age group
was from 18.3 years to 38.7 years. Ethical approval was obtained
from the Institutional Ethical Committee prior to the start of the
study. All the lateral cephalograms obtained for evaluation were
checked for its standard. They were taken with the patients Frankfurt�s
horizontal plane parallel to the floor, mandible in centric
occlusion and their lips at rest.
The SAR angle
Point M: Midpoint of the premaxilla.
Point G: Center of the largest circle that is tangent to theinternal
inferior, anterior, and posterior surfaces of themandibular symphysis.
The centre of premaxilla and mandibular symphysis were
identifid by constructing a template with concentric circleswhose
diameters increased in 0.5 inch increments. Centerof the template
was marked, and Point M and Point G wereidentifid on the tracings.
Point W (Walkers Point): The mean intersection point of thelower
contours of the anterior clinoid processes and thecontour of
the anterior wall of sellaturcica.The three lines that would form
joining these points are:
� Line connecting Point M and Point G
� Line connecting Point W and Point G
� Line from point M perpendicular to the W-G line
The angle that would be measured will be between theperpendicular
line from point M to W-G line and the M-G lineis the SAR
angle (Figure 1).
A computerized cephalometric analysis was carried out with
FACAD(software). The values of SAR angle obtained for each
subgroup was subjected for statistical evaluation. All statistical
analyses were performed with the SPSS software package. For
each variable, the arithmetic mean and SD were calculated. Oneway
ANOVA and post hoc Tukey�s HSD analysis was performed
to check for statistical significance.
Results and Discussion
The mean and standard deviation of SAR angle for skeletal
Class I, Class II and Class III with normal, horizontal and vertical
growth patterns were significantly different (P<0.05). The
normal range of SAR angle values as given by the authors were
55.98�2.24, 50.18�2.70 and 63.65�2.25 for skeletal class I, class
II and class III respectively. The results of the current study are in
accordance with the original values.
One-way ANOVA shows that the SAR angle values were within
the normal range for skeletal Class I and Class II cases in all types
of growth pattern. However, there was a significant(P<0.05) difference
in SAR angle in skeletal Class III cases alone, between the
horizontal and vertical growth pattern (Table 1).
Interpretation of anteroposterior relationship of jaws plays a vital
role in orthodontic treatment planning. This relationship might
also get affected by the varied growth patterns. Many linear and
angular measurements were introduced in cephalometrics for this
purpose. The SAR angle purports to be unaffected by the varying
growth patterns. Thus the reliability of the accuracy of this angle
needs to be studied.
Figure 3 shows the distribution of SAR angle in Skeletal Class I, Class II and Class III individuals in the current study.
Subjects with average growth pattern exhibited good adherence
to SAR angle values. Individuals with horizontal and vertical
growth pattern in Class I and Class II cases also showed reliable
values closer to the normal range. Though the accuracy of this
value in a Class III case with horizontal and vertical pattern is low,
the values fall within the normal range. There were no previous
studies to compare the effectiveness of SAR angle and this happens
to be the first one.
The findings of this study support the fact that SAR angle would
remain stable even when jaws are rotated. Clockwise and anticlockwise
rotation of mandible did not significantly affect the
SAR angle values and they remained within the limits making
it a reliable parameter. Unlike the findings by Shobha et al, that
beta angle may not be a valid tool for assessment of sagittal jaw
discrepancy in patients exhibiting vertical growth patterns with
skeletal Class I and Class II malocclusions, SAR angle was stable
enough in all types of growth pattern [20].
The accuracy of this angle could be due the three points chosen
that are not direct representatives of skeletal structures. Points M
and G have already been proven to be advantageous in locating
over points A and B, which are susceptible to remodeling changes
[21]. Several studies have shown that, the thirs point, the Walkers
point is stable after the age of five [22].Arat et al found out that
the mid cranial base (W-SE) remained unchanged during all stages
of pubertal growth [23].
The limitation of this study could be the use of FACAD software
owing to minor deviation in measurement of SAR angle
but within the acceptable range. SAR angle is an additional toolin
cephalometrics to aid in accurate diagnosis and treatment planning
in orthodontics.
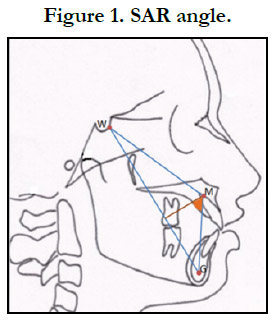
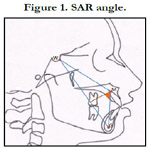
Figure 1. SAR angle.
Figure 2. A Sample Cephalogram Tracing Carried Out in FACAD.
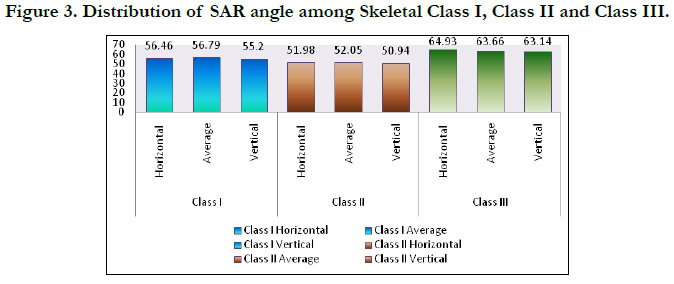

Figure 3. Distribution of SAR angle among Skeletal Class I, Class II and Class III.
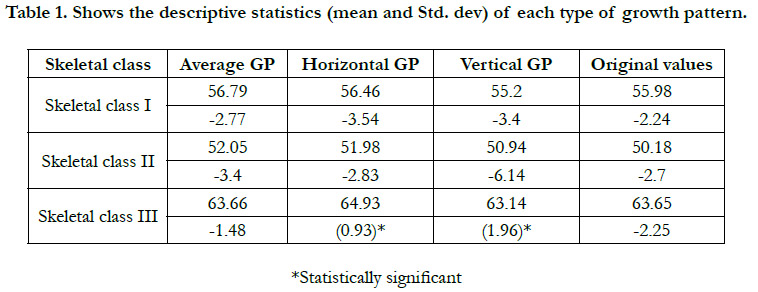

Table 1. Shows the descriptive statistics (mean and Std. dev) of each type of growth pattern.
Conclusion
SAR angle is a reliable indicator of sagital dysplasia in horizontal,
vertical and average growth patterns in skeletal class I and class II
individuals. However, in a skeletal class III condition the vertical
growth pattern showed significantly decreased SAR values than
horizontal growth pattern, but the values still being within the
acceptable range. SAR angle can be used as a reliable alternative
measurement or an additional aid to determine the discrepancy in
apical jaw bases.
References
-
[1]. Agarwal S, Bhagchandani J, Mehrotra P, Kapoor S, Jaiswal RK. The SAR
Angle: A ContemorarySagital Jaw Dysplasia Marker. Orthodontic Journal
of Nepal. 2014;4(2):16-20.
[2]. Arat M, K�kl� A, Ozdiler E, R�bend�z M, Erdogan B. Craniofacial growth and skeletal maturation: a mixed longitudinal study. Eur J Orthod. 2001 Aug;23(4):355-61. PubMed PMID: 11544785.
[3]. Baik CY, Ververidou M. A new approach of assessing sagittal discrepancies: the Beta angle. Am J OrthodDentofacialOrthop. 2004 Jul;126(1):100-5. PubMed PMID: 15224065.
[4]. Bhad WA, Nayak S, Doshi UH. A new approach of assessing sagittal dysplasia: the W angle. Eur J Orthod. 2013 Feb;35(1):66-70. PubMed PMID: 21303811.
[5]. Binder RE. The geometry of cephalometrics. J ClinOrthod. 1979 Apr;13(4):258-63. PubMed PMID: 296153.
[6]. DOWNS WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod. 1948 Oct;34(10):812-40. PubMed PMID: 18882558.
[7]. Frank S. The occlusal plane: Reliability of its cephalometric location and its changes with growth [Thesis]. University of Oklahoma, Oklahoma; 1983.
[8]. Haynes S, Chau MN. The reproducibility and repeatability of the Wits analysis. Am J OrthodDentofacialOrthop. 1995 Jun;107(6):640-7. Pub- Med PMID: 7771370.
[9]. Jacobson A. Application of the "Wits" appraisal. Am J Orthod. 1976 Aug;70(2):179-89. PubMed PMID: 1066054.
[10]. Jacobson A. The "Wits" appraisal of jaw disharmony. Am J Orthod. 1975 Feb;67(2):125-38. PubMed PMID: 1054214.
[11]. Jacobson A. Update on the Wits appraisal. Angle Orthod. 1988 Jul;58(3):205-19. PubMed PMID: 3056122.
[12]. J�rvinen S. The JYD angle: a modified method of establishing sagittal apical base relationship. Eur J Orthod. 1982 Nov;4(4):243-9. PubMed PMID: 6959814.
[13]. McNamara JA Jr. A method of cephalometric evaluation. Am J Orthod. 1984 Dec;86(6):449-69. PubMed PMID: 6594933.
[14]. Melsen B. The cranial base: the postnatal development of the cranial base studied histologically on human autopsy material. ActaOdont Scan. 1974; 32: Suppl.64.
[15]. Moore RN, DuBois LM, Boice PA, Igel KA. The accuracy of measuring condylion location. Am J OrthodDentofacialOrthop. 1989 Apr;95(4):344- 7. PubMed PMID: 2705415.
[16]. Neela PK, Mascarenhas R, Husain A. A new sagittal dysplasia indicator: the YEN angle. World J Orthod. 2009 Summer;10(2):147-51. PubMed PMID: 19582259.
[17]. Rathi SS, Sivakumar A. Comparison of macro lens with normal lens in digital single lens reflex cameras for orthodontic intraoral photographs. Drug Invention Today. 2019 Jun 15;11(6).
[18]. Rathi SS, Sivakumar A. Variation in Lip Thickness in Individuals with Angle's Class 1, Class II and Class III Malocclusion-A Cephalometric Study. Indian Journal of Public Health Research & Development. 2019;10(9):319- 23.
[19]. Richardson M. Measurement of dental base relationship. Eur J Orthod. 1982 Nov;4(4):251-6. PubMed PMID: 6959815.
[20]. Rushton R, Cohen AM, Linney AD. The relationship and reproducibility of angle ANB and the Wits appraisal. Br J Orthod. 1991 Aug;18(3):225-31. PubMed PMID: 1931857.
[21]. Steiner CC. Cephalometrics for you and me. Am J Orthod. 1953;39:729� 55.
[22]. Sundareswaran S, Kumar V. Reliability of Beta angle in assessing true anteroposterior apical base discrepancy in different growth patterns. J Nat SciBiolMed. 2015 Jan-Jun;6(1):125-30. PubMed PMID: 25810649.
[23]. Wylie WL. The assessment of anteroposterior dysplasia. Angle Orthod. 1947;17:97�109.





