Temporomandibular Joint Dysfunction And Swallowing Difficulties In Stroke - An Observational Study� To International Journal Of Dentistry And Oral Science
Nithin Kumar S1*, D. Malarvizhi2
1 B.P.T Intern, SRM College of Physiotherapy, Faculty of Medicine and Health Sciences, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur-
603203, Kanchipuram, Chennai, Tamilnadu, India.
2 Professor, SRM College of Physiotherapy, Faculty of Medicine and Health Sciences, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur-
603203, Kanchipuram, Chennai, Tamilnadu, India.
*Corresponding Author
Nithin Kumar S,
B.P.T Intern, SRM College of Physiotherapy, Faculty of Medicine and Health Sciences, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur-603203, Kanchipuram,
Chennai, Tamilnadu, India.
Tel: +91-9677076622
E-mail: nithinostwal@gmail.com
Received: September 18, 2021; Accepted: November 13, 2021; Published: November 23, 2021
Citation: Nithin Kumar S, D. Malarvizhi. Temporomandibular Joint Dysfunction And Swallowing Difficulties In Stroke - An Observational Study� To International Journal Of Dentistry And Oral Science. Int J Dentistry Oral Sci. 2021;8(11):5109-5112. doi: dx.doi.org/10.19070/2377-8075-210001028
Copyright: Nithin Kumar S�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The prevalence of stroke patient having Temporomandibular joint dysfunction is 30%-60%. 23 % of the
subject have difficulty in swallowing after stroke. In stroke patient, the Temporomandibular joint function and Dysphagia are
prevalent, due to involvement of the masticatory muscles. Hence on rehabilitation of stroke patients, due consideration has
to be given to Temporomandibular joint function and dysphagia.
Objective: To observe the Temporomandibular joint dysfunction and swallowing difficulties in stroke.
Methodology: Non experimental design,10 subjects were selected by convenient sampling and Temporomandibular joint
function and swallowing difficulty were assessed.
Outcome: Craniomandibular Index (CMI) and The Modified Mann Assessment of Swallowing Ability (MMASA). RESULTS:
This study shows that 100% of the samples in this study were found to have temporomandibular joint dysfunctions associated
with stroke. 30% of the stroke population was found to have been affected with dysphagia as a cause of temporomandibular
joint dysfunction associated with stroke.
Conclusion: The study concluded that Temporomandibular joint dysfunction is present among the stroke patients with mild
swallowing difficulties of 30%. Hence stroke patients should also be assessed with Temporomandibular joint function and
swallowing difficulties to prevent dysfunction, stroke management protocol should include Temporomandibular joint treatment.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Stroke; Temporomandibular Joint Dysfunction; Dysphagia; Craniomandibular Index; MMASA.
Introduction
According to World Health Organization Stroke is defined as
�rapidly developing clinical signs of focal (or global) disturbance
of cerebral function, with symptoms lasting 24 hours or
longer or leading to death, with no apparent cause other than
of vascular origin�[1]. In India, the stroke prevalence rate is 84-
262/100,000 in rural areas and 334-424/100,000 in urban areas.
According to recent population-based reports, the incidence rate
is 119-145/100,000.[2] The neurovascular anatomy of stroke is
regulated by two internal carotid and vertebral arteries, and the
pathophysiology of stroke is characterized as impaired perfusion
in the arteries of the brain.
Approximately 30%-60% of patients with stroke have temporomandibular
joint dysfunction.[3], 23 % of the subject have difficulty
in swallowing after stroke. Brunnstorm stages plays a major
role in stroke recovery, in this study stage two was taken as in this
stage depicts the appearance of basic limb synergies beginning
of spasticity.[4] Temporomandibular joint is formed by multiple
bones which includes mandible, zygomatic ,sphenoid, temporal
and hyoid bones.[5] Both osteokinematic and arthrokinematics
movements are important for the normal functioning of the temporomandibular
joint which includes movements like depression,
elevation, retrusion, protrusion, left and right lateral excursions,
gliding and distraction of the mandible.[6]
The temporomandibular joint is one of the most commonly used
joint which is engaged during mastication, swallowing, speaking.
Primary and secondary muscles of temporomandibular joint are
supplied by the mandibular nerve which is branch of trigeminal
nerve and facial nerve from cranial nerve.The superficial temporal,
anterior tympanic, deep temporal, auricular posterior, transverse
facial, middle meningeal, and maxillary arteries, as well as
their branches, are the primary arterial outlets for the lateral and
medial temporomandibular joints, according to research.[7] Abnormalities
of the intra-articular discal location, as well as dysfunction
of the underlying musculature, are symptoms of temporomandibular
joint dysfunction. Painful joint noises, limited or
deviated range of motion, and cranial or muscle pain, also known
as orofacial pain, are some of the symptoms and signs.
Dysphagia is known as difficulty in swallowing, which is most
common in stroke patients where it shows clinical manifestation
such as choking, coughing, packing of food in cheeks. which
leads to malnutrition and dehydration.[8] Although 42-67% people
have been reported with swallowing difficulties, there may be
mild changes based on severity of condition, type of stroke (psychometric
evaluation). 23% of dysphagia was found to be in the
early stage of stroke and affects the quality of life. (Psychometric
evaluation).[9]
Involvement of lesion in brain stem can cause loss of sensation
of mouth, lip and check and loss of trigger response of laryngeal
elevation, closing of glottic and relaxation of cricopharyngeal,
voluntary control of the mastication can be interrupted by the lesion
of cortical region, and also cause contralateral impairment of
lip , tongue, muscle motor control by involvement of precentral
gyrus [10]. The second most noted dysfunction with stroke is craniomandibular
problem, musculoskeletal problem from of temporomandibular
joint disease to connective tissue pain syndrome
.In stroke patient, the TMD and Dysphagia are prevalent, due to
involvement of the masticatory muscles. These muscles should
be assessed and treated in stroke rehabilitation. This study helps
to assess and diagnose the temporomandibular joint dysfunction
and dysphagia.
Materials And Methods
This non -experimental study of observational type was conducted
among stroke patients. the sampling was done using convenient
sampling method. The sample consist of Ischemic stroke patients
between the age group of 45-55 years and under the brunnstrom
stage 2 of recovery. the data was collected between January and
march 2021.IEC 2227/IEC/2020 dated on 04.12.2020 was obtained
before starting the study and the participants were selected
based on the inclusion and exclusion criteria. An informed consent
was obtained after detailed explanation of the study and the
demographic data was collected.
Patients with unstable vitals, arthritis, deformity, fracture and
infections of the temporomandibular joint were excluded. the
following assessment tool was used for data collection. The test
evaluates higher centre function with the total scores of 30 points.
we selected moderate and above moderate, between the score of
18-30. Assessment was done with proper safety and precautionary
methods by using gloves, mask, and hand sanitizer. Index development
consists of two types, generation and definition. Scoring,
and testing. Abnormal findings were assessed from joints, muscles
in the initial phase. Craniomandibular index haven�t been concentrated
much in among stroke patients. This study enhances the influence
of inappropriate mandibulo- temporal joint function and
swallowing difficulties in stroke patients and Craniomandibular
Index and Modified Mandibular Swallowing Assessment is used
as a measurement tool to diagnose. The components of the Craniomandibular
Index are Dysfunction Index (DI), Palpation Index
(PI), the DI and PI includes restrictions of joint movements,
crepitus, along with palpation of the muscles respectively.
The Craniomandibular Index (CMI) was created to provide a
quantitative indicator of mandibular movement disorders, temporomandibular
joint noise, and muscle and joint tenderness for
use in epidemiological and clinical outcome studies.CMI has inter-
rater reliability of 0.84 for the Dysfunction Index, 0.87 for the
Palpation Index, and 0.95 for the Craniomandibular index (CMI),
intra-rater reliability of 0.92 for the Dysfunction Index, 0.86for
the Palpation Index, and 0.96 for the CMI.
The Modified MASA (MMASA) is developed as a screening tool
for dysphagia in stroke, it is an examination for evaluating dysphagia
in bed side and the components of this assessment shows the
standard risk for dysphagia and aspiration. It evaluates 12 skills on
oro-motor and sensory components. it�s aphysician-administered
screening tool for dysphagia in acute stroke with the validity of
0.82, sensitivity of 87-92% and specificity of 84-86%. [11]
Results
The purpose of the study is to determine the prevalence of temporomandibular
joint dysfunctions and swallowing difficulties in
stroke patients. Table 1 and Figure 1 represents the value of craniomandibular
index and it shows that 100% of the study samples
in this study were found to have temporomandibular joint
dysfunctions associated with stroke. Table 2 and Figure 2 depict
the score of Modified Mann Assessment of Swallowing Ability
(MMASA) and from this study 30% of the stroke population was
found to have been affected with dysphagia as a cause of temporomandibular
joint dysfunction associated with stroke.
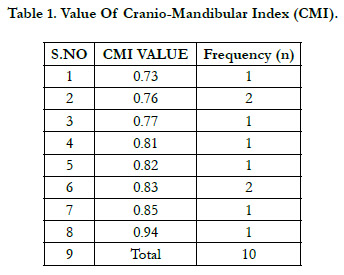

Table 1. Value Of Cranio-Mandibular Index (CMI).
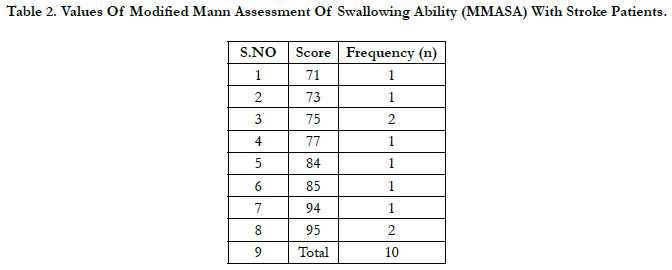
Table 2. Values Of Modified Mann Assessment Of Swallowing Ability (MMASA) With Stroke Patients.
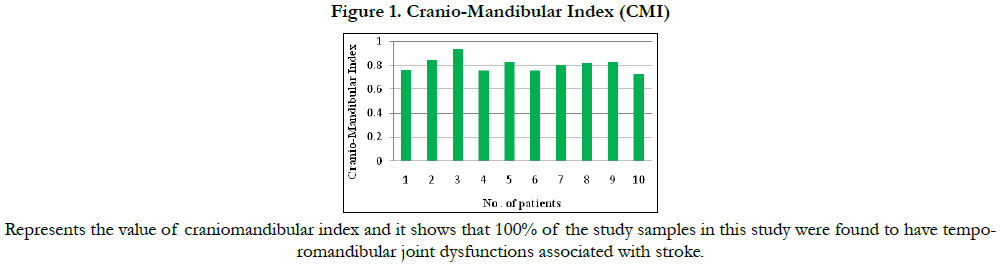

Figure 1. Cranio-Mandibular Index (CMI)
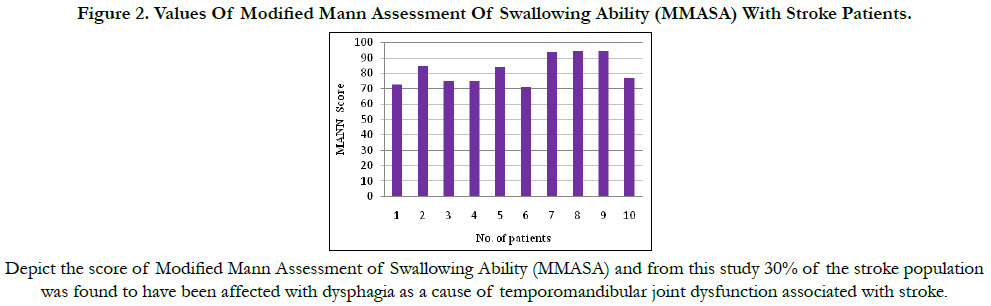

Figure 2. Values Of Modified Mann Assessment Of Swallowing Ability (MMASA) With Stroke Patients.
Discussion
In this study 15 patients with stroke were assessed and among
them only 10 subjects were selected based on the inclusion and
exclusion criteria. Among our population 100% of the patients
were affected with temporomandibular joint disfunction in associated
with 30% of the patients affected with dysphagia. To rule
out the temporomandibular joint dysfunction craniomandibular
index (CMI) was used. on assessing the temporomandibular
joint in stroke patients� wide range of movement difficulties were
found, while dysphagia is one among them with high risk in stroke
patients, the commonly found clinical features of temporomandibular
joint dysfunction and dysphagia are minimal mouth opening,
deviation and restrictions during opening of mouth. This can
lead to lack of appetite, dehydration and jaw deformities indirectly
related with patient�s health status.
Volkan Yilmaz et.al., (2020) have stated that patients affected
with haemorrhagic stroke were 73.3% and ischemic stroke were 26.7%. affected with temporomandibular joint dysfunction. Also
suggest the current therapeutic approach should also focus on
Temporomandibular joint alignment to prevent its dysfunction
which results in dysphagia.Interpretation and recovery of stroke
was assessed based on Brunnstrom stages. patients in this stage
have spasticity and mild involuntary movements appears towards
recovery so this stage were included with high feasibility of sample
size.
Paciaroni M Oh et.al., concluded the prevalence of dysphagia was
found to be moderately high. The scale of the lesion was more
significant than its placement in terms of anatomical-clinical association. Dysphagia was a major predictor of death and injury at
90 days as measured clinically. [12] The rhythmic movements of
the jaw with peripheral sensory inputs shows that central nervous
system CNS reflects the oral motor behaviours of mastication.
[13] The motor control of the masticatory muscles is more localized
and motor unit classifications is less distinct. by these special
features the masticatory muscles have a finer movement and gradation
of force that the trunk and limb muscle.
This study goes along with Duck-Won Oh et.al., (2013) suggested
that restoration of the head and neck, TMJ postural alignment
to improve the functional ability of stomatognathic alignment.
Patients with post-stroke hemiparesis may benefit from stomatognathic
alignment exercises to enhance temporomandibular joint
control and swallowing.
According Olmos SR et.al. stated thatthe complex of crania cervical
and mandibular region including muscles and ligament were
associated with postural abnormality causes temporomandibular
joint dysfunction in stroke patients.[14] The biomechanical analysis
of temporomandibular joint is the most unique in structure
and has complex function. The joint muscles,ligaments and articulating
capsules plays a major role in mastication.[15] The oromotor
stimulation is given to stroke patients to facilitate the muscles
in and around jaw,this technique will help to initiate mastication,
speech and swallowing. to execute this technique proper assessment
and diagnosis of oro-motor is needed. this study focuses on
the detailed examination and interpretation of temporomandibular
joint dysfunction and dysphagia among stroke patients.
Acknowledgments
I Thank my guide prof. Malarvizhiand Mr. Pavan kumar who
spared his time and helped me whenever I needed. I also thank
patients who spent there time and helped me in completion of
this study.
References
-
[1]. Truelsen T, Begg S, Mathers C. The global burden of cerebrovascular disease.
Geneva: World Health Organisation. 2000.
[2]. Pandian JD, Sudhan P. Stroke epidemiology and stroke care services in India. J Stroke. 2013 Sep;15(3):128-34. PubMed PMID: 24396806.
[3]. Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke. Br Med J (Clin Res Ed). 1987 Aug 15;295(6595):411-4.
[4]. Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke. Br Med J (Clin Res Ed). 1987 Aug 15;295(6595):411-4.
[5]. O'Sullivan SB, Schmitz TJ, Fulk G. Physical rehabilitation. FA Davis; 2019 Jan 25.
[6]. Levangie PK, Norkin CC. Joint stru
cture and function: a comprehensive analysis.
[7]. Fricton JR, Schiffman EL. Reliability of a craniomandibular index. J Dent Res. 1986 Nov;65(11):1359-64. PubMed PMID: 3478399.
[8]. Teasell R MD, Hussein N. Clinical consequences of stroke. Evidence-Based Review of Stroke Rehabilitation. Ontario: Heart and Stroke Foundation and Canadian Stroke Network. 2016:1-30.
[9]. Yilmaz V, Aras B, Umay E. Temporomandibular Joint Dysfunction and Impaired Stomatognathic Alignment: A Problem Beyond Swallowing in Patients With Stroke. Indian J Otolaryngol Head Neck Surg. 2020 Sep;72(3):329-334. PubMed PMID: 32728543.
[10]. Seo JH, Kim DK, Kang SH, Seo KM, Seok JW. Severe Spastic Trismus without Generalized Spasticity after Unilateral Brain Stem Stroke. Ann Rehabil Med. 2012 Feb;36(1):154-8. PubMed PMID: 22506250.
[11]. Antonios N, Carnaby-Mann G, Crary M, Miller L, Hubbard H, Hood K, Sambandam R, Xavier A, Silliman S. Analysis of a physician tool for evaluating dysphagia on an inpatient stroke unit: the modified Mann Assessment of Swallowing Ability. J Stroke Cerebrovasc Dis. 2010 Jan;19(1):49-57. Pub- Med PMID: 20123227.
[12]. Paciaroni M, Mazzotta G, Corea F, Caso V, Venti M, et al. Dysphagia following stroke. European neurology. 2004;51(3):162-7.
[13]. vanEijden TM, Turkawski SJ. Morphology and physiology of masticatory muscle motor units. Crit Rev Oral Biol Med. 2001;12(1):76-91. PubMed PMID: 11349964.
[14]. Olmos SR, Kritz-Silverstein D, Halligan W, Silverstein ST. The effect of condyle fossa relationships on head posture. Cranio. 2005 Jan;23(1):48-52. PubMed PMID: 15727321.
[15]. Soboleva U, Laurina L, Slaidina A. The masticatory system--an overview. Stomatologija. 2005;7(3):77-80. PubMed PMID: 16340271.





