Predictors of Dental Care Utilization in School Children in Al-Madinah, Saudi Arabia
Amal Aqeeli1,2*, Alla T. Alsharif2, Estie Kruger3, Marc Tennant4
1 International Research Collaborative, Oral Health and Equity, School of Human Sciences, The University of Western Australia, Perth, Western Australia, Australia.
2 Preventive Dental Sciences, Taibah University Dental College and Hospital, Madinah, Saudi Arabia.
*Corresponding Author
Amal Aqeeli,
International Research Collaborative, Oral Health and Equity, School of Human Sciences, The University of Western Australia, Perth, Western Australia, Australia.
Tel: +61432025197
E-mail: amal.aqeeli@research.uwa.edu.au
Received: October 19, 2021; Accepted: November 10, 2021; Published: November 20, 2021
Citation: Amal Aqeeli, Alla T. Alsharif, Estie Kruger, Marc Tennant. Predictors of Dental Care Utilization in School Children in Al-Madinah, Saudi Arabia. Int J Dentistry Oral Sci. 2021;8(11):5027-5032. doi: dx.doi.org/10.19070/2377-8075-210001013
Copyright: Amal Aqeeli�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: To explore the factors influencing dental care utilization including sociodemographic characteristics, and oral health
need in 9-12-year-old school children in Al-Madinah, Saudi Arabia (SA).
Methods: A stratified random sample was applied to select 10 schools in Al Madinah, SA and a total of 1000 students aged
9-12 years were included in the study. Information on sociodemographic factors and dental care utilization were collectedusing
and oral health related quality of life was recorded using the World Health Organization (WHO) questionnaire. A multiple
logistic regression model was used to examine the factors associated with dental care utilization.
Results: Almost a quarter of all participants (23.8%), have never received dental care before. Pain or trouble with teeth was
the most common reason for visiting the dentist (49.4%), while only 11.8% visited the dentist for routine check-up. Thepercentages
of both missing school, and difficulty in eating due to oral health problems, were significantly higher among those
who received dental care. Children from low-income families had a reduced likelihood of receiving dental care relative to
children from higher and middle-income families (OR=0.571, P=0.014). Children who have caries and who reported having
toothache in the past 12 months were more likely to visit the dentist (OR=1.599, P=0.028) &(OR=2.188, P>0.001).
Conclusion: Dental care utilization is primarily driven by symptomatic dental care. The prevalence of dental utilization was
relatively high among children from high- and middle-income families, children who have caries and children who reported
having toothache in the past 12 months.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Dental Care Utilization; Dental Care; Check-Up; Caries.
Introduction
Dental caries remains the most predominant oral disease in childhood
despite its decline worldwide [1]. Dental care utilization is
an essential component for preventing caries and improving oral
health and well-being.Understanding the factors affectingutilizationhas
been atopic of focus in dental public health.
Several studies have highlighted different reasons of utilization or
underutilization among children. Findings suggest that thereless
dental care use by males, racial minorities, and when lack of accessibility
and affordability exist [2, 3]. Children whose parents have
lower education and awareness and with low socioeconomic status
also underutilize dental care [4, 5]. Other investigations have
identified geographical location and distribution of the dental
care services as other important factors associated with the use
of dental care [6].
Dental care utilization patterns can also be influenced by the presence
of either normative or self-perceived oral health care needs
[7]. In addition, dental carerelated anxiety and fear and reduced
quality of life are also important factors that influence the pattern
of visiting the dentist; those who have dental anxiety end
up avoiding going to the dentist while those who have poor oral
health related quality of life visited a dentist with higher frequency
[5].
Limited data, however, are available on these factors related to
dental care utilization in SA. Saudi Arabia has a great burden of dental caries and a low rate of dental care utilization compared to
developed [8, 9]. In SA, only a small percentage of children visit
the dentist for regular check-ups while the majority go to the dentist
only because of pain, despite the free of charge dental services
provided by the government [10]. Data from El Bcheraoui et al
showed that only 11.5% visited the dentist regularly while AlAgili
et al reported thatone in four children have never visited a dentist
[11, 12]. Perceived barriers to dental care for Saudi children who
never went to a dentist included oral health illiteracy, dentist-related,
financial and transportation [12], while encouraging factors to
utilizing dental care are quality of dental care, reasonable fees for
dental services and close location of dental clinics [13].
Identifying factors related to dental care utilizationwould help in
future public policy making and public health interventions. This
study aimed to investigate the factors associated with dental care
utilization including sociodemographic characteristics, and oral
health need in 9-12 years old schoolchildren in Al-Madinah, SA.
Materials and Methods
Ethical Approval
To access the de-identified oral health survey data, ethical approval
was obtained from the Taibah University Ethics Committee
in Al-Madinah, SA and ethical clearance from the University
of Western Australia Ethics Committee was attained. The study
was conducted in accordance with the principles of the World
Medical Association of Helsinki. Children�s parents� consent was
obtained, as well as a child agreement to participate, prior to interview
and examination. Participation in the study was voluntary
and every questionnaire and examination were anonymous.
Study design and data collection
Oral health survey data was collected by calibrated and trained
staff from the University of Taibah, Department of Preventive
Dental Sciences (DPDS). The survey and oralexaminations were
carried out in accordance with the international standards established
by the World Health Organization [14]. Instructors with
previous experience in oral health surveys and examination following
WHO�s guidelines directed the training.
As for the selection of participating schools, a stratified random
sampling design was applied to select schools. Schools were stratified
based on socioeconomic level of the school districtbased
on the knowledge of the disadvantage of the area; high and low
socio-economic. Afterwards, five schools from each stratum were
randomly selected and included in the survey. Thus, the stratification
of schools was done on area level, however, to carry out the
analysis with more specific data, an indication of individual level
of socio-economic status was also included based on family data.
Both levels included public and private schools.
Prior to each school visit, information sheets and questionnaires
were sent to all parents of 9-12-year-olds in the schools to invite
participation and obtain consent. All 9-12-year-old students who
attended the selected schools on the day of the survey, and whose
parents returned the consent form were included in the survey.
One thousand two hundredsixty-five students were invited to the
survey and the response rate was 83%, so it ended up with 1049
students. Uncompleted questionnaires were excluded from the
study, and it ended up with 1000 students. The final number of
participants per each school ranged from 98-119 adding up to
1000. The children were interviewed to obtain sociodemographic
data, and information on oral health need and quality of life using
the WHO oral health questionnaire for children.
Oral examinations were performed by 10 calibrated and trained
examiners following the standardized WHO Oral Health Survey
assessment form for oral health surveys [14]. Caries experience
was measured clinically by the dental examiners and recorded as
present if the child had at least one tooth as decayed, filled or was
missing due to caries. The interview questionnaire incorporated
information on sociodemographic characteristics, utilization of
dental care, and child self- perception of oral health.
Study Variables
The main outcome of interest in this study was dental care utilization
and was measured using a question about the frequency of
visiting the dentist within the past 12 months (once, twice, three
times, four times or more, or �I have never received dental care�).
A new binary outcome variable was created with all those who
reported dental visits as one category, and all other responses as a
second category (visited the dentist and never visited the dentist).
Independent variables comprised of oral health need variables
which included caries experience (examined need), self-perception
of oral health and toothache in the past 12 months (perceived
need). Caries experience was expressed as (yes or no) for
children with/without any caries experience.
Self-perception of oral health was measured by asking the child
to rate their perception of their oral health (excellent; good; faire;
poor; very poor or I don�t know) and for analytical purposes,
good and fair were merged to good, and poor and very poor were
also merged to poor.
Toothache in past 12 months were measured by asking the child
how often during the past 12 months �did you have toothache
or feel discomfort due to your teeth� (often; occasionally; rarely;
never or do not know). Often, occasionally, and rarely were
merged to yes, and never were recorded asno. Reduced quality
of life due to oral health problems was measured on appearance,
smiling, bullying, missing school and eating. For each variable, the
child had to choose (yes or no).
Sociodemographic variables included age, gender, school type,
and family occupation. Age was categorized as two groups: 9-10
years old and 11-12 years old. The type of school was dichotomized
as public or private schools. To determine level of socioeconomic
status, parents occupations were used as a proxy of
family monthly income, and divided into three categories, low,
medium and high, as described elsewhere [15].
Statistical Analysis
Dental care utilization was analyzed across sociodemographic,
oral health need and reduced quality of life due to oral health
problems. The difference between groups was assessed by using
Chi-square and significance levels was set at P value = 0.05. Logistic
regression model was carried out with dental care utilization
as the dependent variable and adjusting for sociodemographic characteristics and oral health. Software used for data entry (Microsoft
Office Excel 2018 for Windows, Microsoft Corporation,
Redmond, WA, USA) and all statistical tests were conducted using
IBM SPSS software (ver.25.0; IBM, Chicago, IL, USA).
Results
Of 1265 students aged 9-12 years old, a total of 1000 students
with completed questionnaires and oral examinations were analyzed
and included in the study (83% response rate).
Table 1 presents characteristics information for the sample and
the distribution of the variables across dental care utilization.
More than half of the participants (65.6%) were between 11-12
years old. Of the participants, 39.9% were females and 60.1%
were male. There was a high prevalence of dental caries experience
(85.1%), and 81.4% reported toothache in the past 12
months, however, two third of the participants were satisfied with
their oral health; and 62.2% reported good oral health. Pain or
trouble with teeth was the most common reason for visiting the
dentist (49.4%) while only 11.8% visited the dentist for routine
check-up.
The percentage of children who have never received dental care
was 23.8%, and of these, a higher percentage attended public
schools in contrast to private schools (27.1% Vs 20.5%; P=0.014)
(Table 2). Significantly more children from low-income families
had not received dental care (31.5%; P=>0.001).
Among oral health need, the percentage of children who received
dental care was significantly higher among those who have caries
experience and reported toothache in the past 12 months
(P=0.027 and P>0.001 respectively).
As presented in Table 3, reduced quality of life due to oral health
problems was highest in the aspect of feeling embarrassed due to
appearance of teeth (49.5%). The percentages of both a): missing
school; and b) difficulty in eating due to oral health problems,
were significantly higher among those who received dental care
(86.3%; P>0.001 and 79.9%; P=0.036 respectively). The results from the multiple logistic regression model are presented
in Table 4. After controlling for all other variables in the
model, children from low-income families had a reduced likelihood
of receiving dental care relative to children from higher
and middle-income families (OR=0.571; 95% CI: 0.365-0.892,
P=0.014). Children who have caries were more likely to visit the
dentist compared to those who don�thave caries OR=1.599; 95%
CI: 1.051-2.432, P=0.028), and children who reported having
toothache in the past 12 months were more likely to visit the dentist
(OR=2.188 95% CI:1.507-3.178, P>0.001).
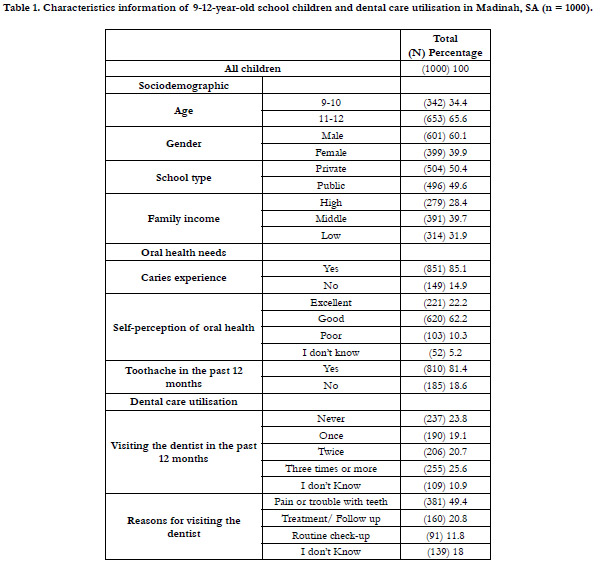

Table 1. Characteristics information of 9-12-year-old school children and dental care utilisation in Madinah, SA (n = 1000).
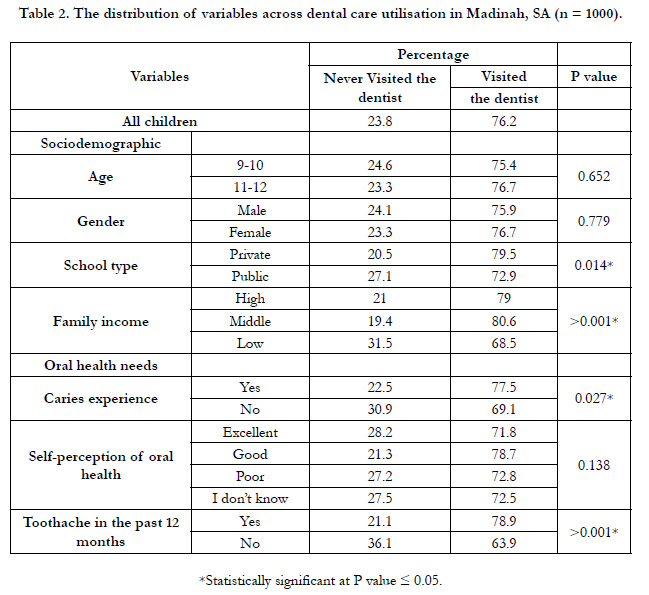
Table 2. The distribution of variables across dental care utilisation in Madinah, SA (n = 1000).
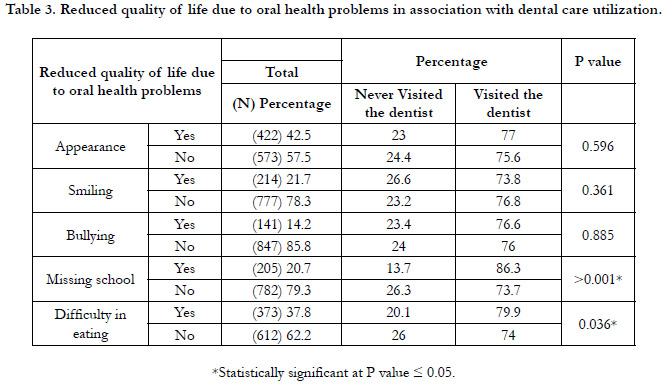
Table 3. Reduced quality of life due to oral health problems in association with dental care utilization.
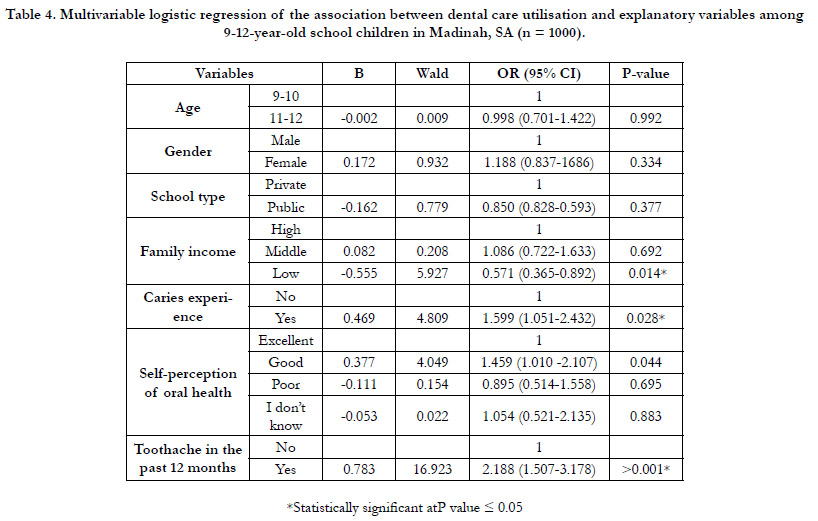
Table 4. Multivariable logistic regression of the association between dental care utilisation and explanatory variables among 9-12-year-old school children in Madinah, SA (n = 1000).
Discussion
This study was conducted to investigate the factors associated
with dental care utilization among 9- to 12-year-old school children
in Al-Madinah, SA. The results indicate that the strongest
predictors of dental care utilization were family income, having
caries, and experiencing toothache.
In our study �s sample population, 23.8% or nearly a quarter never
received dental care in the past. Notably, this result is in agreement
with other studies conducted in SA. To elucidate, Al Agili et
al. reported that 26% of their study sample in Jeddah, SA never
visited the dentist previously [12]. After controlling for other variables,
our findings indicated that the greater the oral health need
for dental care expressed in having caries or experiencing toothache,
the higher the use of dental services among children. Our
results agree with AlHumaid et al., who found that significantly
higher odds of pain were associated with visiting when in dental
pain [10]. In this study, reduced quality of life due to oral health
problems was found to be one of the factors associated with visits
to the dentist. This finding supports the work of Goettems
et al.,who also found that individuals who had poor oral healthrelated
quality of life visited dentists more frequently [5].
Among those who visited the dentist previously,a very small
percentage of children visited regularly for routine check-ups
(11.8%). Meanwhile, majority visited the dentist to address pain or
to undergo follow-up. This is in line with other studies conducted
in SA [10, 11, 16]. Symptomatic dental visits seem to determine
dental care utilization among Saudi children despite thefree access
to dental care in the country and the increasing efforts to promote
preventive dental care visits among children. This irregular pattern
in the use of dental health services contributes to the high
prevalence of untreated dental caries in the population, where it
persists as the main dental health problem among Saudi children
[17]. Herein, it should be highlighted that the prevalence of dental
caries was very high (85.1%).
The reasons why children never visited the dentist before could
be attributed to several factors, includinglack of geographic accessibility.
In a study by Gafar et al., it was reported that far-situated
dental services was one of the perceived barriers to dental
visits [18]. In addition,one of the common reasons that lead to
the avoidance of dental care utilizationis dental-related anxiety.
Dental anxiety leads to avoidance behavior and is associated with
higher caries morbidity and need for oral rehabilitation [19].
Furthermore, parents� education and awareness areimportant factors
that influence dental service use by children [20]. In a study
by Alshammary et al., 58.3% of the respondents reported that
they would take their children to the dentist only if the child is
experiencing pain, while only 13% of the parents stated that they
take their children to the dentist twice a year [21]. Another study
reported that parental oral health illiteracy was the predominant
barrier to dental care use among children [12].
The quality of the provision of dental care plays a crucial role in
determining its utilization. It could influenceparents�satisfaction
which,in turn, could be considered as another perceived barrier
to children�sutilization of the free dental services provided by the
government. The results of a previous study found that parents
of children who never visited the dentist or who needed dental
care in the past 12 month but could not get it reported problems
with the dental health system, which included lack of a dentist or
a specialized dentist in the community, difficulty in getting a dental
appointment, and long wait times at the clinic [12]. In addition,
the unavailability of dentists, long waiting listsand a perception of low quality of dental care in the government�s dental clinics
compared with private dental offices were reported as barriers of
access to dental services in SA [22, 23].
It has been well documented that children from a low socioeconomic
status tend to have the greatest need for and the lowest accessto
dental services [24]. Our findings agree with the literature,
aschildren from low-income families were less likely to receive
dental care services than did children from high income families.
Similar findings have been observed in other countries like Japan
and Canada [25, 26].
These data must be interpreted with caution because the findings
are limited by the cross-sectional nature of this study which does
not support temporality or causality. Bearing in mind that the
study sample was restricted to 9- to 12-year-old primary school
children in Al-Madinah City, caution should be practiced in generalizing
the results to the entire country. However, considering
the cultural homogeneity and urbanity of the area, weexpect our
estimates to be relevant to the general child population in SA.
Moreover, we used self- reported data and father�s and mother�s
occupations as a proximity for family, which this could introduce
bias. And it is important to bear in mind the possible bias in these
responses.
Our findings emphasize that the free access to dental care in SA
does not guarantee theutilization of dental care by everyone who
is in need thereof. This study has identified the predictors of the
utilization of dental care services, which could help in formulating
strategies that are specifically geared towards the population
that is in need of dental care. Future studies are recommended to
further examine the underlying barriers to the utilization of dental
services by children, including the use of geographic analysis to
assess distribution and accessibility of dental services [27]. This
information can be used to inform the enactment of policiesand
todevelop appropriate and specific interventions to increase dental
care utilization among children.
Data Availability Statement
That data that support the findings of this study are available
from Department of Preventive Dental Sciences at Taibah University
Dental College and Hospital, Taibah University, Saudi Arabia,
upon reasonable request.
References
-
[1]. Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T.
Global epidemiology of dental caries and severe periodontitis - a comprehensive
review. J ClinPeriodontol. 2017 Mar;44Suppl 18:S94-S105. PubMed
PMID: 28266116.
[2]. Chen M, Wright CD, Tokede O, Yansane A, Montasem A, Kalenderian E, Beaty TH, Feingold E, Shaffer JR, Crout RJ, Neiswanger K, Weyant RJ, Marazita ML, McNeil DW. Predictors of dental care utilization in northcentral Appalachia in the USA.Community Dent Oral Epidemiol. 2019 Aug;47(4):283-290. PubMed PMID: 30993747.
[3]. Tchicaya A, Lorentz N. Socioeconomic inequalities in the non-use of dental care in Europe. Int J Equity Health. 2014 Jan 29;13:7. doi: 10.1186/1475- 9276-13-7. PubMed PMID: 24476233.
[4]. Edelstein BL, Chinn CH. Update on disparities in oral health and access to dental care for America's children. AcadPediatr. 2009 Nov-Dec;9(6):415-9. PubMed PMID: 19945076.
[5]. Goettems ML, Ardenghi TM, Demarco FF, Romano AR, Torriani DD. Children's use of dental services: influence of maternal dental anxiety, attendance pattern, and perception of children's quality of life. Community Dent Oral Epidemiol. 2012 Oct;40(5):451-8. PubMed PMID: 22537392.
[6]. Yuen A, Rocha CM, Kruger E, Tennant M. The equity of access to primary dental care in S�o Paulo, Brazil: A geospatial analysis. Int Dent J. 2018 Jun;68(3):171-175. PubMed PMID: 28913887.
[7]. Piovesan C, Antunes JL, Guedes RS, Ardenghi TM. Influence of self-perceived oral health and socioeconomic predictors on the utilization of dental care services by schoolchildren. Braz Oral Res. 2011 Mar-Apr;25(2):143-9. PubMed PMID: 21359493.
[8]. M Orfali DS, S Aldossary DM. Utilization of Dental Services in Saudi Arabia: A Review of the Associated Factors. Saudi J Oral Dent Res 2020;05:147�9.
[9]. John JR, Mannan H, Nargundkar S, D'Souza M, Do LG, Arora A. Predictors of dental visits among primary school children in the rural Australian community of Lithgow. BMC Health Serv Res. 2017 Apr 11;17(1):264. PubMed PMID: 28399864.
[10]. AlHumaid J, El Tantawi M, AlAgl A, Kayal S, Al Suwaiyan Z, Al-Ansari A. Dental Visit Patterns and Oral Health Outcomes in Saudi Children. Saudi J Med Med Sci. 2018 May-Aug;6(2):89-94. PubmedPMID: 30787827.
[11]. El Bcheraoui C, Tuffaha M, Daoud F, Kravitz H, AlMazroa MA, Al Saeedi M, Memish ZA, Basulaiman M, Al Rabeeah AA, Mokdad AH. Use of dental clinics and oral hygiene practices in the Kingdom of Saudi Arabia, 2013.Int Dent J. 2016 Apr;66(2):99-104. PubMed PMID: 26749526.
[12]. Al Agili DE, Farsi NJ. Need for dental care drives utilisation of dental services among children in Saudi Arabia. Int Dent J. 2020 Jun;70(3):183-192. PubMed PMID: 31912900.
[13]. Al-Hussyeen AJ. Factors affecting utilization of dental health services and satisfaction among adolescent females in Riyadh City. Saudi Dent J. 2010 Jan;22(1):19-25. PubMed PMID: 23960475.
[14]. World Health Organization. Oral health surveys: basic methods. Fifth Edit. 2013.
[15]. Kassim S, Bakeer H, Alghazy S, Almaghraby Y, Sabbah W, Alsharif A. Socio- Demographic Variation, Perceived Oral Impairment and Oral Impact on Daily Performance among Children in Saudi Arabia. Int J Environ Res Public Health. 2019 Jul 10;16(14):2450. PubMed PMID: 31295837.
[16]. Alayadi H, Bernab� E, Sabbah W. Examining the relationship between oral health-promoting behavior and dental visits. Int J Health Sci (Qassim). 2019 May-Jun;13(3):40-43. PubMed PMID: 31123439.
[17]. Al Agili DE. A systematic review of population-based dental caries studies among children in Saudi Arabia. Saudi Dent J. 2013 Jan;25(1):3-11. Pub- Med PMID: 23960549.
[18]. Gaffar BO, Alagl AS, Al-Ansari AA. The prevalence, causes, and relativity of dental anxiety in adult patients to irregular dental visits. Saudi Med J. 2014 Jun;35(6):598-603. PubMed PMID: 24888660.
[19]. Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety--an epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006 Aug;33(8):588-93. PubMed PMID: 16856956.
[20]. Badri P, Saltaji H, Flores-Mir C, Amin M. Factors affecting children's adherence to regular dental attendance: a systematic review. J Am Dent Assoc. 2014 Aug;145(8):817-28. PubMed PMID: 25082930.
[21]. Alshammary F, Aljohani FA, Alkhuwayr FS, Siddiqui AA. Measurement of Parents' Knowledge toward Oral Health of their Children: An Observational Study from Hail, Saudi Arabia. J Contemp Dent Pract. 2019 Jul 1;20(7):801-805. PubMed PMID: 31597799.
[22]. Alshahrani A, Raheel S. Health-care System and Accessibility of Dental Services in Kingdom of Saudi Arabia: An Update. J Int Oral Heal 2016;8:883� 7.
[23]. Al-Jaber A, Da'ar OB. Primary health care centers, extent of challenges and demand for oral health care in Riyadh, Saudi Arabia. BMC Health Serv Res. 2016 Nov 4;16(1):628. PubMed PMID: 27809919.
[24]. Reda SF, Reda SM, Thomson WM, Schwendicke F. Inequality in Utilization of Dental Services: A Systematic Review and Meta-analysis. Am J Public Health. 2018 Feb;108(2):e1-e7. PubMed PMID: 29267052.
[25]. Nishide A, Fujita M, Sato Y, Nagashima K, Takahashi S, Hata A. Income- Related Inequalities in Access to Dental Care Services in Japan. Int J Environ Res Public Health. 2017 May 12;14(5):524. PubMed PMID: 28498342.
[26]. Ramraj C, Sadeghi L, Lawrence HP, Dempster L, Qui�onez C. Is accessing dental care becoming more difficult? Evidence from Canada's middle-income population.2013;8(2):e57377. PubMed PMID: 23437378; PMCID: PMC3577722.
[27]. Alsharif AT, Kruger E, Tennant M. Identifying and prioritising areas of child dental service need: a GIS-based approach. Community Dent Health. 2016 Mar;33(1):33-8. PubMed PMID: 27149771.





