Frequency Of Dental Erosion Among Undergraduate Dental Students Of Pakistan
Dr. Hina Zafar Raja1*, Dr. Muhammad Nasir Saleem2, Dr. Ummara Manzoor3, Dr. Maryam Mumtaz4, Dr. Sarosh Ehsan5, Dr. Mariya6
1 Professor of Prosthodontics, Institute of Dentistry CMH Lahore Medical College, Abdul Rehman Road, Lahore Cantt, Lahore, Pakistan.
2 Professor of Prosthodontics, Institute of Dentistry CMH Lahore Medical College, Abdul Rehman Road, Lahore Cantt, Lahore, Pakistan.
3 FCPS-II Resident, Department of Prosthodontics, Institute of Dentistry,CMH Lahore Medical College, Abdul Rehman Road, Lahore Cantt, Lahore, Pakistan.
4 FCPS-II Resident, Department of Prosthodontics, Institute of Dentistry,CMH Lahore Medical College, Abdul Rehman Road, Lahore Cantt, Lahore, Pakistan.
5 Associate Professor, Department of Operative dentistry, College of dentistry,FMH Lahore Medical College, Lahore, Pakistan.
6 Assistant Professor, Department of Prosthodontics, Sardar Begum Dental College, Peshawar, Pakistan.
*Corresponding Author
Prof. Dr. Hina Zafar Raja,
Department of Prosthodontics, Institute of Dentistry, CMH Lahore Medical College, 198 G, Model Town, Lahore, Pakistan.
Tel: 0092-334-4222341
E-mail: hinazafarraja@gmail.com
Received: July 27, 2021; Accepted: November 10, 2021; Published: November 12, 2021
Citation: Dr. Hina Zafar Raja, Dr. Muhammad Nasir Saleem, Dr. Ummara Manzoor, Dr. Maryam Mumtaz, Dr. Sarosh Ehsan, Dr. Mariya. Frequency Of Dental Erosion Among
Undergraduate Dental Students Of Pakistan. Int J Dentistry Oral Sci. 2021;8(11):4983-4986. doi: dx.doi.org/10.19070/2377-8075-210001003
Copyright: Dr. Hina Zafar Raja�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Dental erosion is a form of tooth wear which occurs as a result of dissolution of dental hard tissues caused
by acids of non-bacterial origin. Erosion can occur due to intrinsic acids (within the body) or extrinsic acids (dietary intake).
Erosive lesion due dietary or gastric acids forms smooth lesions which typically appear as cupped occlusal/ incisal and concave
buccal/facial surfaces
Objective: The objective of this study was to evaluate the prevalence of dental erosion among undergraduate dental students
in various dental colleges of Pakistan.
Material and Method: This study was conducted at Institute of Dentistry, Combined Military Hospital Lahore Medical
College, Fatima Memorial Hospital College of Dentistry, Lahore and Sardar Begum Dental College, Peshawar. Sample size
calculated was 330 and data was collected over a period of two years. Signs for erosive lesion were observed during clinical
examination. Lesions graded according to Basic erosive wear examination (B.E.W.E.) index and reported.
Results: A sample of 330 dental students is taken with the mean age 21.62 � 1.17 years. There were 107 (32.4%) male and 223
(67.6%) female students in the sample. Prevalence of the erosion in the dental students was 14.8% (49/330).
Conclusion: 107 (32.4%) male and 223 (67.6%) female undergraduate dental students were examined for dental erosion .The
frequency of dental erosion among dental students was reported to be 14.8%.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Tooth Erosion; Students; Dental; Tooth Attrition; Tooth Wea.
Introduction
Tooth wear results in the loss of dental hard tissues from the
tooth surfaces. Factors other than carious lesion,dental trauma,
and developmental disorders can lead to this condition [1, 2]. It is
an irreversible, non-cariogenic origin process resulting in destruction
and functional loss of dental hard tissue. It can manifest as
abrasion, attrition, abfraction and erosion or a combination of
these processes [3].
Dental erosion is one of the main causes of tooth surface loss
of tooth due to exposure of tooth to extrinsic or intrinsic acids
which are not produced by bacteria. Severity of erosion can lead
to compromised esthetics and decreased vertical dimension of
occlusion [4]. The intrinsic acids are mostly originated as a result
of gastric reflux (GERD),vomiting along with anorexia, bulimia
nervosa, and rumination [5]. Extrinsic acids can act through carbonated
beverages, citrus fruit, and food pickled with vinegar.
Medications like vitamin C, iron preparations, inhalers used by
asthmatic patients and aspirincan also contribute to be a source
of extrinsic acid leading to dental erosion [6].
Dental erosion can manifests as sensitivity, pain ,inefficient mastication,
accidental biting of soft tissues (cheek biting), fractured
teeth, increased chances of tooth decay, loss of vertical dimensions
of occlusion [7]. Early detection of dental erosion can help
to reduce and manage the lesion more efficiently.
Different indices can be used to measure tooth wear. Eccles [8]
classified tooth wear lesions as early, small and advanced, with
no strict criteria definitions, thus allowing wide interpretation.
Smith and Knight [9] developed a tooth wear indexto measure
and monitor multifactorial tooth wear. Xhonga and Valdmanis
[10] divided erosion lesions into four levels by measurement with
a periodontal probe but itdid not address the problem of inter- or
intra-examiner variability [11]. The index used to measure erosion
in this study is BEWE (Basic Erosive Wear Examination) index
[12]. BEWE index is a simple tool to use in general practice,it
records the most severely affected surface in each sextant. The
lesion is graded according to four level score and the cumulative
score classified and matched to risk levels which guide the
management of the condition. The BEWE allows re-analysis and
integration of results from existing studies [12].
In Pakistan, a study was conducted in Karachi about prevalence
of dental erosion in school children [13]. No significant studies
have been conducted in Pakistan to measure the prevalence of
dental erosion among undergraduate dental students,therefore, it
is the need of the day such study be conducted to evaluate the extent
of dental erosion in undergraduate dental students of Pakistan.
It will also impart awareness among young dental students to
diagnose and prevent erosion, its causative factors and methods
of reducing dental erosion. This study evaluates the prevalence
of dental erosion among undergraduate dental students in various
dental colleges of Pakistan and highlight the possible etiological
factors leading to dental erosion.
Methodology
This study was conducted at three dental institutes of Pakistan
including,Institute of Dentistry, Combined Military Hospital Lahore
Medical College, Fatima Memorial Hospital College of Dentistry,
Lahore and Sardar Begum Dental College, Peshawar over a
period of two years, starting from January 2019 till January 2021.
Sample size was calculated using WHO software for sample size
collection,which was 330. The margin of error was kept 5% and
confidence interval was 95%.Observational study design was used
and the subjects were selected on the basis of non-probability
convenient sampling technique. Undergraduate dental students
between the age of 19 to 25 years of age, with no systemic diseases
were included. Dental students with developmental enamel
defects, history of orthodontic treatment, having any dental
malocclusion,students taking any medications leading to xerostomia
(e.g. anti-hypertensive, anti- depressants, anti-cholinergics,-
anti-psychotics, anti-histamines) and history of radiotherapy were
not included.
Informed consent was taken verbally before examining the subject.
The clinical examination of first year, second year, third year
and final year undergraduate dental student was done using sterilized
dental mirrors only. The following areas were examined in
the mouth:
1.Palatal surfaces of maxillary anterior teeth
2. Lingual surface of mandibular anterior teeth in individuals suffering
from GERD.
3.Occlusal surfaces of posterior teeth.
The teeth were marked using the Basic Erosive Wear Examination
(BEWE) index. The BEWE scoring system records the most
severely affected surface in a sextant. The four level score (Table
1)12 grades the appearance or severity of wear on teeth from no
surface loss (0), initial loss of enamel surface texture (1), distinct
defect, hard tissue loss (dentine) less than 50% of the surface area
(2) or hard tissue loss more than 50% of the surface area (3) [12].
Erosion along with superimposed attrition was considered as erosive
lesions while attrition was recorded separately.
Results
A sample of 330 dental students was taken with the mean age
21.62 � 1.17 years. There were 107 (32.4%) male and 223 (67.6%)
female students in the sample (figure 1).
The frequency of dental erosion in the dental students was reported
to be 14.8% (49/330).However, attrition was present in
12.4% (41/330) of the whole sample. The frequency and percentage
for the presence of erosion and attrition is given in the
Table-2.
When the dental students were evaluated for the erosion through
BEWE index, 283 (85.8%) had no erosive tooth wear, 39 (11.8%)
had initial loss of surface texture, and 8 (2.4%) had distinct defect
that is hard tissue loss with less than 50% of surface area. It is
worthy to note that in the whole sample, no student had hard
tissue loss with more than 50% of surface area. The distribution
of males and females falling in each category of BEWE index is
displayed in figure 2. Out of 107 males, 93 (87%) had no erosion,
12 (11%) had initial loss, and 2 (2%) had distinct defect. Almost
same percentages are observed for the females.
The Chi-square test of association was applied between gender
and erosion that came out to be statistically non-significant. For
the males, the prevalence of the erosion was observed to be 14% (15/107) while for females, it was 15.2% (34/223). So, no significant
association was found between gender and status of erosion.
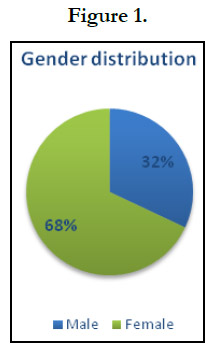
Figure 1.
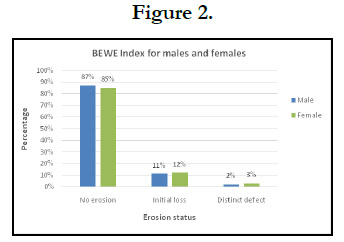
Figure 2.


Table 1. Criteria for grading erosive wear.
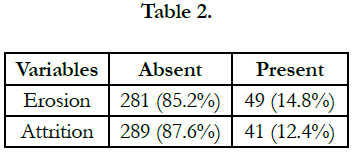
Table 2.
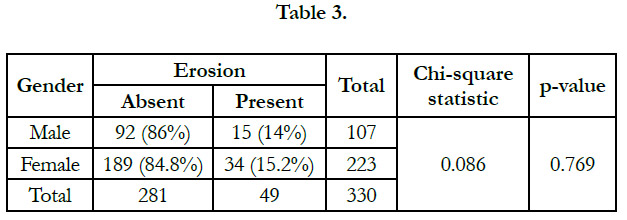
Table 3.
Discussion
The aim of this study wasto evaluate the extent of dental erosion
among undergraduate dental students and impart awareness
about the diagnosis, prevention and management dental erosion.
Basic Erosive Wear Examination (BEWE) Indexwas used to assess
the extent of dental erosion. It was found that 85.8% students
had �0� BEWE index score. This referred to no active erosive
lesion. 11.8% had initial tooth surface loss, while 2.4% had
distinct defect with hard tissue loss accompanying less than 50%
of surface area. However, it was noted that no subject had hard
tissue loss with more than 50% of surface area, which can bedue
to good oral hygiene practices.
In our study the frequency of dental erosion among undergraduate
dental students was found to be 14.8% which is far less than
that found in a similar study conducted in China [14] on nonmedical
university students, which was found to be 44%. This difference
in frequency can be subjected to better understanding of
oral health among dental students leading to better dietary habits,
restraining of acidic beverages , access to fluorinated water,
improved oral hygiene practices including the use a soft-bristled
tooth brush with fluoridated toothpaste and avoid using abrasive
toothpastes (some whitening toothpastes and charcoal-based
toothpastes are more abrasive).
An additional finding of attrition was also found among 12.4% of
dental students. In previous studies [15], it is reported to be 33.3%
among adolescents between the age of 14 to 19 years old. In our
study, the students between of 19 to 25 years have reduced stress
levels which can contribute low incidence of erosion. Stress can
cause vomiting, rumination, anorexia and bulimia nervosa which
can lead to dental erosion as well [16]. Decrease in stress level in
this age group can bebecause of cultural values and lifestyle, the
students mostly are dependent on their families and taken care by
elders. They have financial responsibilities to fulfil. Decrease in
incidence of dental attrition can also be due to increased awareness
of oral health among dental students. Habits like bruxism
are addressed earlier and intervened at earlier stages before it can
cause any harm. Better oral hygiene practices are encouraged like
the use of fluorinated toothpaste and soft tooth brushes. Students from Khyber Pakthunwan showed increased incidence of attrition
which can be attributed to increase chewing of tobacco.
The study also showed that dental erosion does not show predilection
towards gender bias. In the age group between 19 to 25
years of age the difference is not significant statistically, it is observed
to be 14% in males while in females its 15.2%. In a study
done in UK, it was found that females practice better oral hygiene
and brush more frequently then males [17].
Although the results found in our study are not alarming, the
prevalence of dental erosion among undergraduate dental students
among demands attention. Dentists should routinely assess
the risk of dental erosion among young population for diagnosis
and management. Preventive approach should be adopted among
dental students to further decrease its incidence and increase
awareness among dental students. Awareness among dental students
can be increased via seminars, dental conferences, social
media campaigns, brochure and poster competition etc.Measures
like regular monitoring need to be practiced as part of mini�mal
intervention dentistry. Once a preventive approach or any other
form of treatment is implemented, follow-up assessments should
be made to see if the measures undertaken are successful.18
Monitoring requires a complete reassessment where the history,
special tests, color photographs and dental casts are repeated, to
note either improvement or otherwise from the original assessment18.
Limitations
The limitation of this study is that dental erosion was checked
among a specific age group 19 to 25 years of age. General population
was not considered. The results could vary in different age
groups.
Recommendations
Dental erosion is multifactorial condition. As health providers it
is our prime responsibility to identify the possible risk factors and
make the community aware of the ways to prevent this condition.
Dietary counseling should be done at an early stage in schools and
universities, such as, limiting the acidic foods and drinks and their
avoidance at night should be stressed. Habits such as frothing or
swishing the drink around the mouth or drinking in small sips can
be avoided. If a straw is used it can be wide bore and kept at the
back of the mouth in order to reduce the contact area between
the acid and the teeth. After consumption of an acidic food or
drink if tooth brushing is done immediately it would lead to rapid
loss of enamel surface.
Conclusions
The frequency of dental erosion among undergraduate the dental students was found to be 14.8% .However, attrition was present
in 12.4% (41/330) of the whole sample. This study suggested
percentage of students suffering from dental erosioncan have
severe adverse effects in future as the lesion progress.However,
no significant association was found between dental erosion and
gender of patient. This study will encourage clinicians, students
and general dental practitioners to pay more attention to erosive
wear and hence will be beneficial for patient care.
References
-
[1]. Litonjua LA, Andreana S, Bush PJ, Cohen RE. Tooth wear: attrition, erosion,
and abrasion. Quintessence Int. 2003 Jun;34(6):435-46. PubMed
PMID: 12859088.
[2]. Lussi A. Dental erosion: from diagnosis to therapy: Karger Medical and Scientific Publishers; 2006.
[3]. Imfeld T. Dental erosion. Definition, classification and links. Eur J Oral Sci. 1996 Apr;104(2 ( Pt 2)):151-5. PubMed PMID: 8804882.
[4]. Vailati F, Belser UC. Full-mouth adhesive rehabilitation of a severely eroded dentition: the three-step technique. Part 3. Eur J Esthet Dent. 2008 Autumn; 3(3):236-57. PubMed PMID: 19655541.
[5]. Li BK. Cyclic Vimiting Syndrome: Proceedings of the International Scientific Symposium on Cyclical Vomiting Syndrome Held at St. Bart: Lippincott- Raven; 1995.
[6]. Milosevic A, Young PJ, Lennon MA. The prevalence of tooth wear in 14-year-old school children in Liverpool. Community Dent Health. 1994 Jun;11(2):83-6. PubMed PMID: 8044716.
[7]. Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012 Jan 13;212(1):17-27. PubMed PMID: 22240686.
[8]. Eccles JD. Dental erosion of nonindustrial origin. A clinical survey and classification. J Prosthet Dent. 1979 Dec;42(6):649-53. PubMed PMID: 292776.
[9]. Smith BG, Knight JK. An index for measuring the wear of teeth. Br Dent J. 1984 Jun 23;156(12):435-8. PubMed PMID: 6590081.
[10]. Xhonga FA, Valdmanis S. Geographic comparisons of the incidence of dental erosion: a two centre study. J Oral Rehabil. 1983 May;10(3):269-77. PubMed PMID: 6575167.
[11]. L�pez-Fr�as FJ, Castellanos-Cosano L, Mart�n-Gonz�lez J, Llamas-Carreras JM, Segura-Egea JJ. Clinical measurement of tooth wear: Tooth wear indices. J Clin Exp Dent. 2012 Feb 1;4(1):e48-53. PubMed PMID: 24558525.
[12]. Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008 Mar;12 Suppl 1(Suppl 1):S65-8. PubMed PMID: 18228057.
[13]. Najmi N, Bugti AA, Nadeem M, Hannan H, Tanwir F, Shafiq F. PREVALENCE AND PREDICTORS OF DENTAL EROSION IN SCHOOL CHILDREN OF KARACHI PAKISTAN. International Journal of Dental Clinics. 2013;5(3).
[14]. Chu CH, Ng A, Chau AM, Lo EC. Dental Erosion and Caries Status of Chinese University Students. Oral Health Prev Dent. 2015;13(3):237-44. PubMed PMID: 25197728.
[15]. Casanova-Rosado JF, Medina-Sol�s CE, Vallejos-S�nchez AA, Casanova- Rosado AJ, Maupom� G, Avila-Burgos L. Dental attrition and associated factors in adolescents 14 to 19 years of age: a pilot study. Int J Prosthodont. 2005 Nov-Dec;18(6):516-9. PubMed PMID: 16335172.
[16]. Scheutzel P. Etiology of dental erosion--intrinsic factors. Eur J Oral Sci. 1996 Apr;104(2 ( Pt 2)):178-90. PubMed PMID: 8804885.
[17]. Al-Dlaigan YH, Shaw L, Smith AJ. Dental erosion in a group of British 14-year-old, school children. Part III: Influence of oral hygiene practises. Br Dent J. 2002 May 11;192(9):526-30. PubMed PMID: 12047125.
[18]. Kaidonis JA. Oral diagnosis and treatment planning: part 4. Non-carious tooth surface loss and assessment of risk. Br Dent J. 2012 Aug;213(4):155- 61. PubMed PMID: 22918343.





